G6pd deficiency means?
Reading File
Finding Sources
Searching the Web
G6PD deficiency mechanism clinical features treatment 2024
Reading File
Reading File
Reading File
Loading Image
Reading File
Here is a thorough explanation of G6PD deficiency sourced from Harrison's and Lippincott Illustrated Biochemistry:
G6PD Deficiency (Glucose-6-Phosphate Dehydrogenase Deficiency)
What Is It?
G6PD deficiency is the most common disease-producing enzyme abnormality in humans, affecting over 400-500 million people worldwide. It is a hereditary condition caused by mutations in the G6PD gene on the X chromosome, resulting in reduced or absent activity of the G6PD enzyme in red blood cells.
- Inheritance: X-linked recessive - affects mostly males (hemizygous)
- Epidemiology: Highest prevalence in persons from tropical Africa, the Middle East, Asia, and the Mediterranean region
- Evolutionary advantage: G6PD deficiency confers partial protection against Plasmodium falciparum malaria, which explains its geographic distribution
The Biochemical Mechanism
The diagram below (from Lippincott Biochemistry) explains it visually:
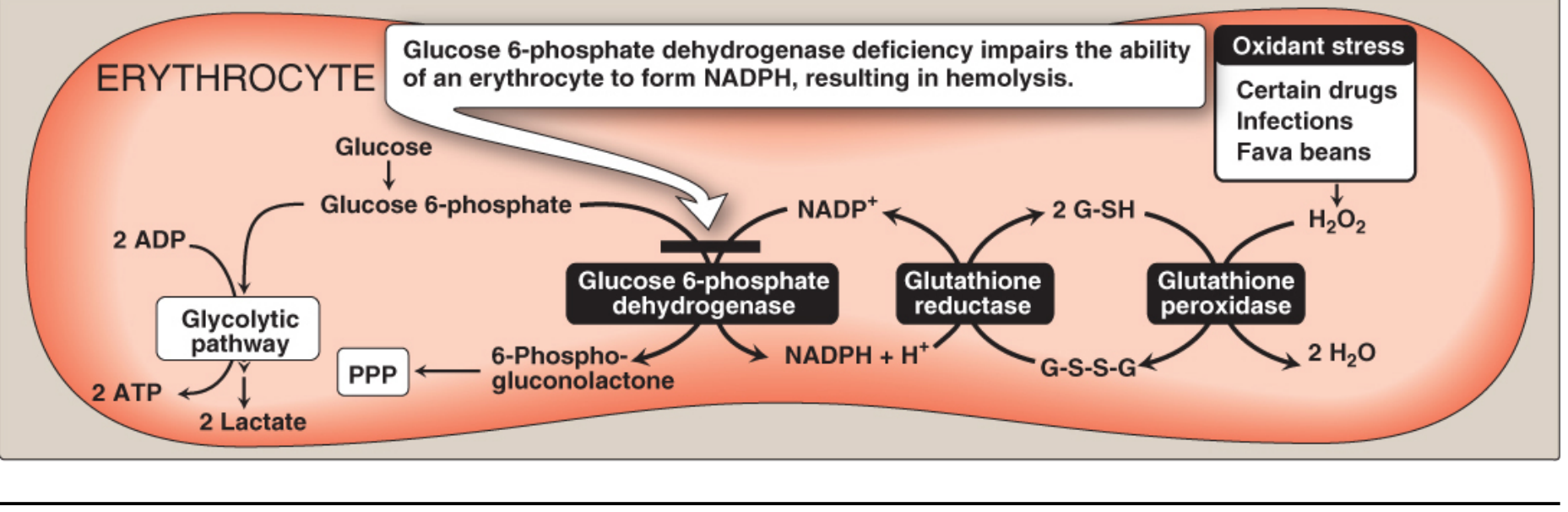
- G6PD is the first enzyme of the pentose phosphate pathway (PPP)
- It converts glucose-6-phosphate to 6-phosphogluconolactone, producing NADPH
- NADPH is needed by glutathione reductase to keep glutathione in its reduced (active) form (G-SH)
- Reduced glutathione (G-SH) neutralizes H2O2 and other free radicals via glutathione peroxidase
- Without G6PD: no NADPH → no reduced glutathione → oxidative damage accumulates → hemolysis
Red blood cells are uniquely vulnerable because:
- The PPP is their only source of NADPH
- They have no nucleus or ribosomes and cannot renew enzyme supply
- Lippincott Biochemistry, 8th ed., p. 445-449
Triggers (Precipitating Factors)
Most people are asymptomatic until exposed to an oxidant stress:
| Trigger | Examples |
|---|---|
| Oxidant drugs | Sulfa antibiotics, primaquine, dapsone, nitrofurantoin, some analgesics/antipyretics |
| Fava beans (Favism) | Especially the Mediterranean variant |
| Infection | Inflammatory response generates free radicals in macrophages that diffuse into RBCs |
Classification by Severity
| Class | Symptoms | Residual Enzyme Activity |
|---|---|---|
| I | Very severe - chronic non-spherocytic hemolytic anemia (CNSHA) | <10% |
| II | Severe - acute hemolytic anemia (e.g., G6PD Mediterranean) | <10% |
| III | Moderate (e.g., G6PD A-, most common in Africans) | 10-60% |
| IV | No symptoms | >60% |
Classes II and III are the most common forms.
Clinical Features
- Acute hemolytic anemia (AHA) - triggered by above factors, usually self-limiting in 8-14 days (because younger red cells have more G6PD activity and are spared)
- Neonatal jaundice (NNJ) - appears 1-4 days after birth, due to elevated unconjugated bilirubin; may be severe
- Heinz bodies - denatured hemoglobin forms insoluble masses (visible on special staining), leading to rigid, less deformable RBCs that are removed by the spleen and liver
- Chronic non-spherocytic hemolytic anemia (CNSHA) - only in Class I (rare)
- "Bite cells" - RBCs with a chunk removed by the spleen (seen on peripheral smear)
Diagnosis
- G6PD enzyme assay (quantitative) - gold standard
- Peripheral blood smear showing Heinz bodies and bite cells
- Note: Do NOT test during an acute hemolytic episode - the oldest (most deficient) cells are destroyed first, leaving younger cells with normal G6PD levels, giving a false-normal result
Management
- Acute episodes: Mostly supportive; remove the offending trigger. Blood transfusion if anemia is severe. Hemodialysis if acute renal failure develops
- Favism: Completely preventable by avoiding fava beans
- Drug-induced: Screen before prescribing known oxidant drugs; use alternative drugs
- Neonatal jaundice: Phototherapy or exchange transfusion (same management as NNJ from other causes)
- CNSHA (Class I): Folic acid supplements, hematologic surveillance; splenectomy has been beneficial in severe cases
- Harrison's Principles of Internal Medicine, 22E (2025), p. treatment section
Key Point Summary
G6PD deficiency = no NADPH → no reduced glutathione → RBCs cannot fight oxidative stress → hemolysis when triggered. Most people are fine until exposed to drugs, infections, or fava beans.
This is a shared conversation. Sign in to Orris to start your own chat.