bel's palsy
Reading File
Finding Sources
Searching PubMed
"Bell palsy"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive information to write a thorough answer. Let me compile it.
Bell's Palsy
Bell's palsy is the most common cause of acute unilateral facial paralysis. The name honors Sir Charles Bell, who first described the anatomy and function of the facial nerve.
Epidemiology
- Incidence: ~23-25 per 100,000 per year; approximately 1 in 60 persons over a lifetime
- Affects men and women roughly equally, at all ages
- Risk factors: diabetes mellitus, pregnancy (especially third trimester and first 2 weeks postpartum), and possibly hypertension
- Recurs in ~7-8% of cases, typically averaging 10 years between episodes
Anatomy Reminder
CN VII (facial nerve) supplies:
- Motor innervation to all muscles of facial expression and the scalp
- The stapedius muscle (sound dampening)
- Taste to the anterior 2/3 of the tongue (via chorda tympani)
- Parasympathetic fibers to lacrimal, submandibular, and sublingual glands
The nerve travels through the tight facial canal in the temporal bone - this anatomical constraint is central to why inflammation causes palsy.
Pathophysiology
Bell's palsy is a diagnosis of exclusion - "idiopathic" facial palsy. The dominant mechanism is:
- HSV-1 reactivation in the geniculate ganglion - HSV-1 DNA has been detected by PCR in endoneurial fluid surrounding CN VII in the majority of cases, and HSV inoculation in mice reproduces the syndrome
- VZV reactivation - accounts for up to one-third of cases (many without visible rash, distinguishing it from classic Ramsay Hunt)
- SARS-CoV-2 and HIV seroconversion have also been implicated
- Inflammation causes edema of the nerve within the rigid bony canal, producing compression ischemia
Clinical Manifestations
| Feature | Details |
|---|---|
| Onset | Acute; maximal weakness within 48 h (Harrison's) to 72 h (Tintinalli's) |
| Pain | Retroauricular pain 1-2 days before paralysis |
| Paralysis type | Lower motor neuron - weakness of BOTH upper and lower face (including frontalis), distinguishing it from central/UMN lesions |
| Taste | Impaired anterior 2/3 tongue (chorda tympani involvement) |
| Hyperacusis | Stapedius paralysis - sounds seem louder ipsilaterally |
| Lacrimation | May be reduced ipsilaterally |
| Numbness | Facial fullness/numbness reported subjectively; true sensory loss is rare |
Key bedside sign: In Bell's palsy, the patient cannot raise the eyebrow or close the eye on the affected side (LMN). In a stroke (UMN lesion), the forehead is spared because it receives bilateral cortical innervation.
Differential Diagnosis
These must be excluded before calling it Bell's palsy:
| Condition | Clue |
|---|---|
| Ramsay Hunt syndrome (VZV) | Vesicular rash in external auditory canal, pinna, palate; often more severe, worse prognosis |
| Lyme disease | Endemic area exposure, erythema migrans, can be bilateral; in endemic areas ≥10% of facial palsies |
| Sarcoidosis | Often bilateral; systemic features |
| Guillain-Barré syndrome | Bilateral facial palsy, ascending weakness, areflexia |
| Parotid/skull base tumor | Slowly progressive or recurrent palsy |
| HIV seroconversion | CSF pleocytosis present |
| Melkersson-Rosenthal | Recurrent facial palsy + facial edema + fissured tongue |
| Otitis media/cholesteatoma | Ear examination findings |
| Leprosy | Endemic areas, skin lesions |
Investigations
- MRI with gadolinium (fat-suppressed T1): Diffuse smooth linear enhancement of the facial nerve - geniculate ganglion, tympanic and mastoid segments - without a mass lesion (shown below). Note: similar enhancement can occur in Lyme, sarcoidosis, and perineural malignant spread, so it is supportive not diagnostic.
- EMG/NCS (after 10 days): Denervation potentials suggest axonal loss - predicts prolonged recovery over months; absence favors neurapraxia and good prognosis
- CSF: Mild lymphocytosis in a minority (not routinely sampled)
- Routine blood work: consider fasting glucose, Lyme serology (endemic areas), HIV if clinically indicated
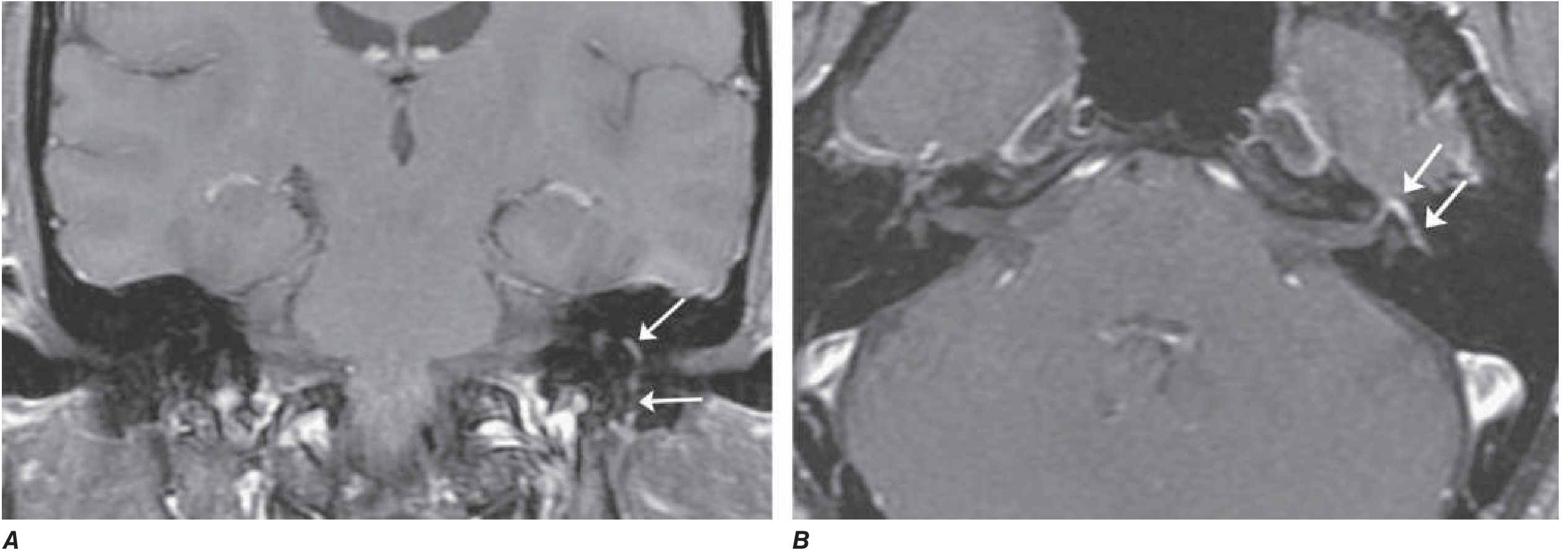
Axial and coronal gadolinium-enhanced T1 MRI with fat suppression showing diffuse smooth linear enhancement of the facial nerve (genu, tympanic, and mastoid segments) - arrows. Highly suggestive of Bell's palsy but not pathognomonic. (Harrison's, Fig. 452-4)
Treatment
1. Corticosteroids (first-line, evidence-based)
- Prednisolone 25 mg twice daily for 10 days (Goldman-Cecil) or 40-60 mg/day for 10 days (Adams & Victor)
- Must be started early (within 72 hours of onset, ideally within 24-48 h)
- Increases complete recovery from ~63% to ~83% at 3 months
- Mechanism: reduces nerve edema within the tight facial canal
2. Antiviral agents (adjunct - selected cases)
- Acyclovir (400 mg 5x/day for 7 days) or Valacyclovir added to steroids
- Acyclovir alone provides no independent benefit
- Evidence is mixed: Sullivan trial did not support antivirals + steroids; Hato et al. found additive benefit of valacyclovir + prednisolone in patients with complete facial palsy
- Most guidelines offer antivirals as optional adjunct to steroids in moderate-severe cases
3. Eye protection
- Essential in complete palsy where eyelid closure is impaired
- Artificial tears during day; lubricating ointment + eye patch at night
- Prevents exposure keratopathy and corneal ulceration
4. No role for surgical decompression
- No evidence of benefit; may be harmful (Adams & Victor)
5. Physical therapy / rehabilitation
- Recent systematic reviews and meta-analyses (2024-2025) support physical therapy for peripheral facial palsy, particularly neuromuscular retraining and mime therapy
- Electrical stimulation in the acute stage remains controversial - a 2026 meta-analysis (PMID: 41167647) assessed its role
Prognosis
- ~70-80% recover completely within a few weeks to months
- ~85% achieve near-normal function
- ~10% have poor recovery
- Favorable signs:
- Incomplete paralysis in the first week
- Any motor recovery within 5-7 days
- Return of taste within the first week
- Unfavorable signs:
- Complete paralysis from onset
- EMG denervation after 10 days (axonal degeneration - recovery takes 3+ months via regeneration)
- Pronounced gadolinium enhancement on MRI
- Complications of aberrant regeneration:
- Synkinesis (involuntary co-movements, e.g., eye closure when chewing)
- Crocodile tears (tearing when eating - misdirected regeneration to lacrimal gland)
- "Jaw winking" (eye closure on jaw movement)
Summary Table
| Feature | Details |
|---|---|
| Nerve affected | CN VII (facial nerve) |
| Type of palsy | LMN - upper + lower face involved |
| Most common cause | HSV-1 reactivation |
| Incidence | 23-25/100,000/year |
| Key treatment | Prednisolone within 72 h |
| Recovery rate | ~80-85% |
| Recurrence | ~7-8% |
Sources: Harrison's Principles of Internal Medicine 22E, p. 3598 | Adams and Victor's Principles of Neurology 12E, p. 1371 | Goldman-Cecil Medicine | Tintinalli's Emergency Medicine
Recent evidence: Physical therapy meta-analyses (PMID 37149416, 2024) support neuromuscular rehabilitation. Electrical stimulation in acute Bell's palsy was reviewed in a 2026 meta-analysis (PMID 41167647) - findings are pending clinical integration. Core steroid and eye care management remains unchanged.
causes
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
I now have comprehensive data. Here is a detailed breakdown of causes of facial (CN VII) palsy:
Causes of Facial (CN VII) Palsy
The question "causes" in the context of Bell's palsy means two things:
- The cause of Bell's palsy itself (its pathophysiology)
- The differential diagnoses - other causes of facial palsy that must be excluded
A. Cause of Bell's Palsy Itself
Bell's palsy is by definition idiopathic, but the current evidence strongly implicates:
| Cause | Evidence |
|---|---|
| HSV-1 reactivation (most common) | HSV-1 DNA found by PCR in endoneurial fluid of CN VII in ~11/14 surgical cases; HSV inoculation in mice reproduces the palsy |
| VZV reactivation (without rash) | Up to one-third of cases; VZV without a visible rash is called "zoster sine herpete" |
| SARS-CoV-2 | Increasingly reported post-COVID or post-vaccine |
| HIV seroconversion | Facial palsy can be the presenting feature |
The final common pathway: viral-induced inflammation and edema of CN VII within the tight, rigid facial canal in the temporal bone → compression ischemia → demyelination or axonal injury.
B. Full Differential of Facial (LMN) Palsy - by Category
1. Infectious
| Condition | Key Features |
|---|---|
| Ramsay Hunt Syndrome (VZV) | Vesicular rash in external auditory canal, pinna, palate; severe otalgia; often involves CN VIII too; worse prognosis than Bell's |
| Lyme disease (Borrelia burgdorferi) | Endemic area, tick bite, erythema migrans; can be bilateral (bilateral = Lyme until proven otherwise); CSF pleocytosis; ≥10% of facial palsies in endemic areas |
| HIV infection | Can occur at seroconversion; associated with CSF pleocytosis |
| Otitis media / mastoiditis | Ear pain, hearing loss, abnormal otoscopy; facial nerve runs through middle ear - suppurative inflammation tracks to it |
| Cholesteatoma | Chronic erosive process eroding the bony facial canal |
| Leprosy | Endemic areas; skin lesions; commonly involves facial nerve |
| Tuberculosis | Mastoid/petrous bone TB |
| Infectious mononucleosis | EBV; facial palsy 1-2 weeks after illness |
| Chicken pox | In children, facial palsy follows by 1-2 weeks |
| Malignant otitis externa | Pseudomonas in diabetics/immunocompromised; skull base osteomyelitis |
2. Neoplastic
| Condition | Key Features |
|---|---|
| Parotid gland tumors | Most common extratemporal cause; adenoid cystic carcinoma is notorious for perineural spread |
| Facial nerve tumors (schwannoma, hemangioma) | Intrinsic nerve tumors; ~5% of facial nerve dysfunction |
| Cholesteatoma | Erosive benign "tumor" of middle ear |
| Vestibular schwannoma (acoustic neuroma) | CPA tumor - facial palsy is rare/late; asymmetric SNHL is typical first symptom |
| Meningioma / CPA tumors | CPA or IAC location |
| Carcinomatous meningitis | Leptomeningeal metastases; often multiple cranial nerve palsies |
| Glomus jugulare / tympanicum | Paraganglioma of skull base |
3. Inflammatory / Autoimmune
| Condition | Key Features |
|---|---|
| Sarcoidosis | Often bilateral; systemic features (lymphadenopathy, skin, lungs); Heerfordt's syndrome (uveoparotid fever) = uveitis + parotitis + facial palsy |
| Guillain-Barré Syndrome | Often bilateral facial palsy; ascending paralysis, areflexia; Miller Fisher variant |
| Sjögren's syndrome | Cranial neuropathy as part of systemic disease |
| Amyloidosis | Infiltrative neuropathy |
| Melkersson-Rosenthal syndrome | Recurrent facial palsy + recurrent facial/labial edema + fissured tongue; cause unknown |
4. Traumatic
| Cause | Key Features |
|---|---|
| Temporal bone fracture | Longitudinal (most common) - often involves middle ear, oval window; transverse - more likely to injure CN VII directly |
| Birth trauma / forceps delivery | Neonatal facial palsy |
| Iatrogenic | Post-mastoidectomy (most common surgical injury, vertical segment); parotidectomy; CPA surgery |
5. Vascular
| Cause | Key Features |
|---|---|
| Pontine stroke | Affects CN VII nucleus - LMN palsy; associated with CN VI palsy and contralateral hemiparesis (Millard-Gubler or Foville syndrome) |
| Multiple sclerosis | Demyelinating plaque at the fascicular level in the pons |
6. Metabolic / Systemic
| Cause | Key Features |
|---|---|
| Diabetes mellitus | Facial palsy is more common in diabetics; may be part of diabetic cranial neuropathy |
| Hypertension | Possible risk factor |
| Pregnancy | Up to 3x increased risk in third trimester and early postpartum |
C. Red Flags Suggesting NOT Bell's Palsy
These features should prompt a search for an alternative diagnosis:
- Weakness evolving slowly over weeks (rather than <72 hours) - suggests tumor
- Bilateral facial palsy - think Lyme, GBS, sarcoidosis
- Recurrent palsy on the same side - think tumor, cholesteatoma, Melkersson-Rosenthal
- Palsy with other cranial nerve deficits - think CPA lesion, carcinomatous meningitis
- Intact forehead movement - think UMN/central lesion (stroke)
- Abnormal otoscopy (vesicles, perforation, mass) - think Ramsay Hunt, cholesteatoma, otitis media
- No recovery at 3-4 months - mandates imaging
D. Anatomical Level of Lesion - Localizing CN VII Palsy
| Lesion Level | Associated Findings |
|---|---|
| Cortex / UMN | Lower face only weak; forehead spared (bilateral cortical supply) |
| Pons | LMN palsy + ipsilateral CN VI palsy ± contralateral hemiparesis |
| CPA / IAC | LMN palsy + SNHL + tinnitus (CN VIII involvement) |
| Geniculate ganglion | LMN palsy + loss of taste + hyperacusis + reduced lacrimation |
| Distal to chorda tympani | LMN palsy + loss of taste; lacrimation preserved |
| Stylomastoid foramen (distal) | Pure motor LMN palsy; taste and lacrimation intact |
| Parotid | Branch-specific weakness patterns |
Sources: Harrison's 22E | Adams & Victor's Neurology 12E | Schwartz's Principles of Surgery 11E | Cummings Otolaryngology | Tintinalli's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.