TLICS SCORE
Reading File
Finding Sources
Searching PubMed
TLICS thoracolumbar injury classification severity score
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Here is a comprehensive breakdown of the TLICS Score, synthesized from multiple authoritative orthopaedic textbooks:
TLICS Score - Thoracolumbar Injury Classification and Severity Score
Background
The TLICS was developed in 2005 by the Spine Trauma Study Group (Vaccaro et al.) as a modification of the earlier TLISS (Thoracolumbar Injury Severity Score). It was created to overcome the limitations of prior classification systems (like the AO classification), which failed to incorporate neurological status and could not guide clinical decision-making. The TLICS was the first classification to incorporate a scoring system to guide treatment.
The Three Domains
The TLICS score is the sum of three categories:
1. Fracture Morphology
| Morphology | Points |
|---|---|
| Compression fracture | 1 |
| Burst fracture | 1 (some sources: 2) |
| Translation / Rotation | 3 |
| Distraction | 4 |
Note: Injury morphologies are not additive - only the highest applicable score is used.
2. Posterior Ligamentous Complex (PLC) Integrity
| PLC Status | Points |
|---|---|
| Intact | 0 |
| Suspected / Indeterminate | 2 |
| Injured | 3 |
The PLC includes the supraspinous ligament, interspinous ligament, ligamentum flavum, and facet joint capsules. This is often the most difficult category to assess and is best evaluated with MRI (though MRI can overestimate injury).
3. Neurological Status
| Neurological Status | Points |
|---|---|
| Intact | 0 |
| Nerve root injury | 1-2 |
| Spinal cord / Conus medullaris - Incomplete | 3 |
| Spinal cord / Conus medullaris - Complete | 2 |
| Cauda equina injury | 3 |
Incomplete cord injury scores higher than complete, because surgery offers greater potential for neurological recovery.
Treatment Algorithm
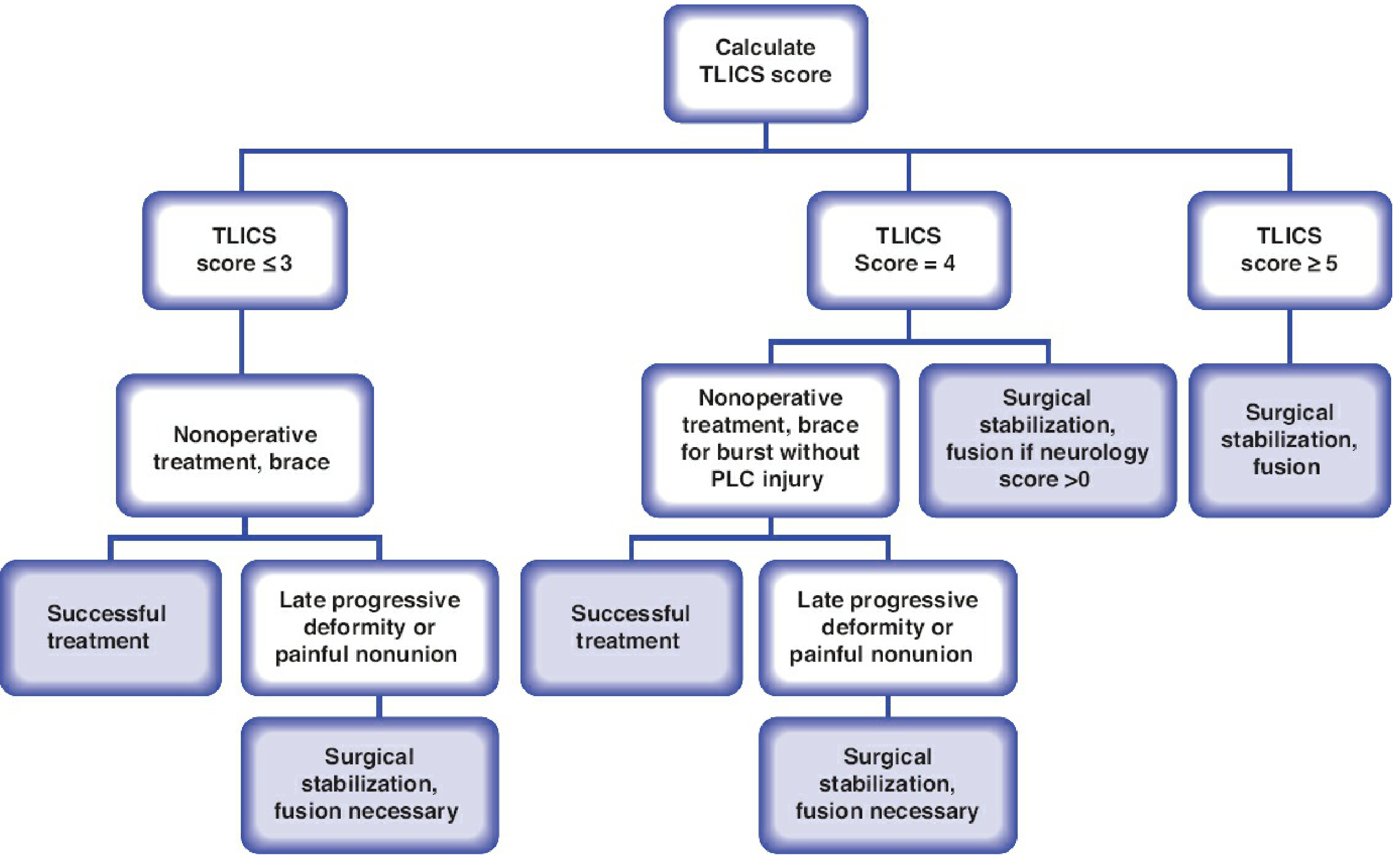
| Total Score | Recommendation |
|---|---|
| ≤ 3 | Non-operative treatment (brace/orthosis) |
| = 4 | Indeterminate - surgeon's discretion (either operative or non-operative) |
| ≥ 5 | Operative treatment (surgical stabilization + fusion) |
- For score = 4: approximately 60% of patients are treated surgically. Burst fractures without PLC injury may be managed non-operatively. If neurological score > 0, surgical stabilization and fusion is preferred.
- The Load-Sharing Classification (McCormack) is used alongside TLICS = 4 cases to assess structural stability in neurologically intact patients.
Limitations
- Neurological exam unavailable in a significant proportion of multiply injured (polytrauma) patients, making the score inapplicable.
- PLC integrity is difficult to determine - even MRI can be falsely positive, leading to artificially elevated scores. Up to ~40% of cases remain "indeterminate."
- Does not describe fracture personality - can't guide the type of surgery needed.
- Based on a "North American" treatment philosophy - less generalizable globally (e.g., in settings where burst fractures without PLC injury or neurological deficit are routinely operated).
- Has limited inter- and intraobserver reliability for morphology classification.
TLICS vs. TLISS
| Feature | TLISS | TLICS |
|---|---|---|
| Category 1 | Mechanism of injury | Fracture morphology |
| Category 2 | PLC integrity | PLC integrity |
| Category 3 | Neurological status | Neurological status |
| Modification | Original (2005) | Refined version |
The switch from "mechanism" (TLISS) to "fracture morphology" (TLICS) was made to improve reliability, since mechanism requires observer interpretation and introduced variability.
Comparison with AO Spine TL Classification (TL AOSIS)
The newer AO Spine Thoracolumbar Injury Classification also uses a scoring system with type A (compression), B (distraction), and C (translational) injuries:
- Score ≤ 3: non-operative
- Score 4-5: either approach
- Score ≥ 6: operative
Studies show TL AOSIS more accurately characterizes injury severity, but TLICS remains widely used as a teaching tool and clinical decision aid.
Sources: Rockwood and Green's Fractures in Adults, 10th Ed. 2025; Campbell's Operative Orthopaedics, 15th Ed. 2026; Bradley and Daroff's Neurology in Clinical Practice
How do you assess PLC injury on imaging (CT vs MRI)?
Finding Sources
Searching PubMed
posterior ligamentous complex thoracolumbar MRI CT assessment
Finding Sources
Searching PubMed
posterior ligamentous complex thoracolumbar spine MRI accuracy
Finding Sources
Reading Article
PMID: 42432333
Reading Article
PMID: 36705382
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
I now have solid textbook and recent literature evidence to give a thorough answer. Here it is:
Assessing PLC Injury on Imaging: CT vs. MRI
What is the PLC?
The Posterior Ligamentous Complex includes:
- Supraspinous ligament (SSL)
- Interspinous ligament (ISL)
- Ligamentum flavum
- Facet joint capsules
These structures are the primary tension-band restraints of the posterior spine. Disruption leads to instability and is the single most important determinant of the TLICS score (up to 3 points).
CT Scan - Indirect Signs Only
CT cannot directly visualize ligaments (they are soft tissue). Assessment is entirely indirect, based on bony surrogate markers:
| CT Finding | Significance |
|---|---|
| Interspinous widening | Widening between adjacent spinous processes suggests ISL/SSL disruption |
| Facet joint diastasis / subluxation / dislocation | Indicates facet capsule disruption |
| Increased interspinous distance ratio (vs. adjacent levels) | Ratio >1.5x adjacent level is suspicious |
| Focal kyphotic angulation | >15-20° segmental kyphosis suggests posterior distraction |
| Translation / listhesis | Vertebral offset implies PLC failure |
| Laminar fractures / spinous process fractures | Avulsion-type injuries imply ligament pull-off |
| Vertebral height loss, endplate angle | Combined with interspinous distance: useful screening combo |
CT Accuracy
- CT provides high sensitivity for bony injury but low sensitivity (~60-70%) for isolated ligamentous disruption
- A 2023 study (Guo et al., PMID 36705382) found that endplate angle + interspinous distance on CT had AUC >0.7 and can serve as a preliminary screening tool before MRI
- CT is the first-line imaging in trauma; PLC status is considered "indeterminate" until MRI is obtained
MRI - Gold Standard for Direct PLC Visualization
MRI is the definitive modality because it directly images ligamentous tissue.
Sequences Used
| Sequence | Role |
|---|---|
| T2-weighted | Ligament tears appear as T2 hyperintensity (edema/hemorrhage) within the ligament substance |
| STIR (Short Tau Inversion Recovery) | Fat-suppressed T2 - best for detecting edema and marrow signal; most sensitive for soft tissue injury |
| T1-weighted | Low signal in acute injury; useful to confirm anatomical disruption |
MRI Signs of PLC Injury
| Structure | MRI Finding |
|---|---|
| Supraspinous / Interspinous ligament | T2/STIR hyperintensity within or replacing the dark ligament stripe ("black stripe discontinuity") |
| Ligamentum flavum | Discontinuity or abnormal T2 signal |
| Facet capsules | Fluid signal in facet joints (joint effusion/capsular tear) |
| Posterior disc | T2 signal change, disc disruption |
| Bone marrow | STIR edema in posterior elements (spinous process, lamina) supports avulsion/traction injury |
The "Black Stripe Sign"
On T2/STIR, intact ligaments appear as dark (hypointense) continuous stripes. PLC injury shows:
- Discontinuity of the dark stripe
- Replacement by bright (hyperintense) signal - indicating edema, hemorrhage, or frank tear
A 2026 study (Aly et al., PMID 42432333) confirmed that MRI black stripe discontinuity is the reference standard, and found that CT-based interspinous widening measurements (including supraspinous distance, midspinous distance, interlaminar distance, and interspinous angle) all showed low AUC (<0.70) for detecting PLC injury - reinforcing that CT alone is insufficient.
Critical Limitation: MRI Overestimates PLC Injury
This is one of the most clinically important points in TLICS application:
"The use of MRI, which is more prone to false-positive diagnosis of PLC injuries, may produce falsely elevated TLICS scores, leading to a greater rate of operative treatment."
- Campbell's Operative Orthopaedics, 15th Ed. 2026
Why MRI Over-reads PLC Injury:
- Edema spreads beyond actual tear - reactive edema in adjacent soft tissue can mimic ligament disruption on STIR
- Partial tears vs. complete tears are hard to distinguish - both show hyperintensity
- Patient positioning and field strength affect signal
- Reader experience variability - even with MRI, inter-observer reliability for PLC integrity is only moderate
- Timing - acute hemorrhage (first 24-48h) and evolving edema can simulate injury
Practical Summary: CT vs. MRI
| Feature | CT | MRI |
|---|---|---|
| Direct ligament visualization | No | Yes |
| Bony injury | Excellent | Moderate |
| PLC sensitivity | ~60-70% (indirect) | High (~80-90%) |
| PLC specificity | Higher (fewer false positives) | Lower (false positives common) |
| TLICS impact | May score as "indeterminate" | May over-score as "injured" |
| Availability in acute trauma | Excellent | Limited / delayed |
| Recommended role | Initial screening; quantify bony anatomy | Definitive PLC assessment before surgery |
Clinical Approach (Recommended)
- CT first in all thoracolumbar trauma - assess morphology, bony alignment, interspinous distance
- If CT shows indirect signs of PLC disruption or morphology suggests instability (burst, distraction, translation) → get MRI
- Interpret MRI findings in clinical context - do not treat the MRI in isolation; correlate with mechanism, CT findings, and neurological exam
- In polytrauma or obtunded patients, MRI findings alone should be weighted carefully given the false-positive rate
- Score = 4 cases especially benefit from MRI - but remember that MRI-positive PLC does not always mandate surgery
Sources: Campbell's Operative Orthopaedics 15th Ed. 2026; Rockwood and Green's Fractures in Adults 10th Ed. 2025; Aly et al., Eur Spine J 2026 [PMID 42432333]; Guo et al., Medicine 2023 [PMID 36705382]
This is a shared conversation. Sign in to Orris to start your own chat.