Thyroplasty essay answer 1000 words
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information from Cummings Otolaryngology. Let me write the essay.
Thyroplasty
Introduction
Thyroplasty refers to a group of phonosurgical procedures that alter the position or tension of the vocal folds by modifying the thyroid cartilage framework, without directly violating the endolaryngeal mucosa. The classification system most widely used today was developed by Isshiki and colleagues in 1974, who described four types based on the direction of the desired phonatory change. Of these, Type I (medialization thyroplasty) is by far the most clinically relevant and commonly performed, and it is now considered by many surgeons to be the procedure of choice for managing the paralyzed vocal fold.
Historical Background
The concept of external laryngeal framework surgery predates modern otolaryngology. Payr first described an approach using a flap of thyroid cartilage for vocal fold medialization in 1915. Subsequently, Meurman reported a series using autologous rib cartilage grafts placed between the thyroid ala and the inner perichondrium via a parasagittal incision, though this was associated with a high complication rate due to perichondrial and mucosal perforations. The modern era was ushered in by Isshiki, who formalized the four-type classification and described Type I thyroplasty in a landmark 1974 publication. His systematic framework transformed these procedures from sporadic surgical experiments into reproducible, teachable operations.
Isshiki Classification
Isshiki described four thyroplasty types, each addressing a different vocal fold deficiency:
- Type I (Medialization): The thyroid cartilage is windowed and an implant is placed to push the vocal fold medially. This addresses glottic insufficiency from paralysis, paresis, bowing, or soft tissue loss.
- Type II (Lateralization): The vocal fold is displaced laterally to widen the glottis, used in cases of bilateral adductor spasm (spasmodic dysphonia) or bilateral paralysis causing airway obstruction.
- Type III (Shortening/Relaxation): The vocal fold is shortened and relaxed by resecting a midline portion of the thyroid cartilage, lowering pitch — used for mutational falsetto or desired pitch reduction.
- Type IV (Lengthening/Cricothyroid Approximation): The cricothyroid distance is increased by suturing the cricoid to the lower thyroid cartilage, raising pitch — applied in feminization laryngoplasty.
Indications for Type I (Medialization) Thyroplasty
Medialization thyroplasty addresses glottic insufficiency — the failure of the vocal folds to meet adequately during phonation. Primary indications include:
- Unilateral vocal fold paralysis (most common indication) — from recurrent laryngeal nerve injury secondary to thyroid surgery, chest surgery, skull base tumor resection, vagal nerve damage, or idiopathic causes
- Vocal fold bowing due to presbylaryngis (aging)
- Cricothyroid joint fixation
- Sulcus vocalis
- Soft tissue defects from excision of pathologic tissue
- Palliative purposes — in patients with malignancy causing recurrent laryngeal nerve sacrifice, where medialization improves voice and reduces aspiration risk
Timing is a key consideration. For paralytic dysphonia, definitive surgery is indicated when recovery is negligible. When recovery is anticipated, medialization thyroplasty may still be considered for severe aspiration or dysphonia as an alternative to repeated vocal fold injections, though our experience has not shown an adverse effect in patients who have subsequently recovered function.
Preoperative Assessment
Thorough preoperative evaluation is essential. Videostroboscopy allows dynamic assessment of the vocal fold vibration, closure pattern, and phase symmetry — useful for both preoperative planning and postoperative evaluation. Laryngeal electromyography (LEMG) is the only available test to evaluate the integrity of the laryngeal motor unit, helping differentiate paralysis from mechanical fixation and providing prognostic information on reinnervation potential.
Surgical Technique
The operation is characteristically performed under local anaesthesia with the patient awake. This is a critical advantage: it allows intraoperative voice monitoring, with the patient phonating continuously so that the surgeon can optimize implant position in real time. Patient positioning is more anatomic when awake (versus supine under general anaesthesia), enabling better assessment.
The standard approach involves a horizontal neck incision at the level of the thyroid cartilage. After subplatysmal flap elevation, the strap muscles are divided in the midline and the thyroid cartilage is exposed. A window is created in the thyroid ala at a position corresponding to the midportion of the vocal fold. Key anatomical landmarks for window placement include the lower border of the thyroid cartilage (approximately one-third of the vertical height up from the inferior border) and a measured distance from the anterior midline depending on the patient's sex (men have a larger cartilage and require a more lateral window placement).
An implant is then placed through this window into the paraglottic space, lateral to the inner perichondrium, to medialize the vocal fold without disrupting its mucosal architecture. Implant materials in common use include:
- Silastic (silicone): Can be carved from block or pre-formed (Netterville or Montgomery systems). Offers the greatest flexibility for tailoring shape and degree of medialization.
- Gore-Tex (expanded polytetrafluoroethylene): A pliable strip placed through the fenestra or via an inferior approach; easily adjustable and well tolerated.
- Dense hydroxyapatite (VoCoM): Biocompatible ceramic implant; provides a rigid, stable medialization but is less flexible to reshape.
The procedure is potentially reversible — if the implant requires adjustment or the patient recovers vocal fold function, it can be removed or revised.
Adjunctive Procedures
Medialization thyroplasty alone may not achieve adequate glottic closure when the arytenoid cartilage is in a laterally displaced or rotated position, as commonly occurs with posterior glottic gap. In such cases, arytenoid adduction is added. This procedure involves placing a suture through the muscular process of the arytenoid to simulate the pull of the lateral cricoarytenoid muscle, rotating the arytenoid medially and anteriorly. Research in animal models indicates that in flaccid laryngeal paralysis, the acoustic and aerodynamic results of arytenoid adduction combined with thyroplasty are superior to those of thyroplasty alone. The efficacy of Type I thyroplasty alone for closing a posterior gap is controversial, and clinical observation supports that a posterior extension of the thyroplasty implant does not reliably address this gap.
Laryngeal reinnervation procedures may also be combined with, or used as an alternative to, thyroplasty. These aim to restore muscle tone by rerouting nearby motor nerve branches (e.g., ansa cervicalis to recurrent laryngeal nerve). Reinnervation can prevent vocal fold atrophy and maintain mucosal vibratory quality, though it does not restore active motion.
Postoperative Care and Outcomes
Type I thyroplasty can in most cases be performed as an outpatient procedure. Inpatient observation is warranted for patients undergoing bilateral procedures, those with obstructive sleep apnoea, those requiring anticoagulation bridging, and other high-risk co-morbidities. Voice outcomes are generally excellent, with significant improvements in fundamental frequency, maximum phonation time, and vocal intensity. Subjective measures — including the Voice Handicap Index (VHI) — consistently show marked improvement.
Complications
Complications, though relatively uncommon, include:
- Failure to achieve adequate medialization — the most frequent cause of revision
- Penetration of the endolaryngeal mucosa during window creation or implant placement
- Wound infection and chondritis
- Implant migration or extrusion
- Airway obstruction — the most feared complication, necessitating emergency airway management
- Revision thyroplasty — surgically feasible in cases of incomplete closure; alternatives at revision include vocal fold injection with autologous fat or Cymetra, reinnervation, and arytenoid adduction
Conclusion
Thyroplasty, particularly Type I medialization thyroplasty, represents the gold standard surgical intervention for glottic insufficiency. Its advantages — local anaesthesia with intraoperative voice monitoring, structural preservation of the vocal fold, and reversibility — make it superior in many scenarios to injection laryngoplasty. A thorough understanding of the Isshiki classification, patient selection criteria, implant options, and adjunctive procedures allows the otolaryngologist to tailor management to each patient and achieve durable improvements in voice, swallowing safety, and quality of life.
Sources: Cummings Otolaryngology Head and Neck Surgery (pp. 1151–1244); K.J. Lee's Essential Otolaryngology
Carcinoma of Retromolar Trigone - ENT exam essay answer with diagrams-flowcharts 1000 words
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive information from Cummings Otolaryngology and KJ Lee's. I have the surgical images and TNM staging table. Let me write the full essay with flowcharts rendered in Markdown/ASCII and embed the textbook images.
Carcinoma of the Retromolar Trigone
Anatomy and Definition
The retromolar trigone (RMT) is a triangular area of mucosa overlying the ascending ramus of the mandible, beginning just posterior to the last lower molar tooth and extending superiorly to the maxillary tuberosity. Its boundaries are:
- Anterior: Posterior surface of the last mandibular molar
- Posterior/superior: Maxillary tuberosity
- Lateral: Continuous with the buccal mucosa
- Medial: Continuous with the anterior tonsillar pillar (pterygomandibular raphe)
Critically, only a thin layer of soft tissue separates the RMT mucosa from the underlying mandibular periosteum and bone, and the mandibular foramen lies in close proximity. Sensation is provided by the lesser palatine nerve (CN V2) and branches of the glossopharyngeal nerve (CN IX) — the latter explaining the characteristic referred otalgia. The primary lymphatic drainage is to the upper cervical jugulodigastric (level II) lymph nodes.
Epidemiology and Aetiology
RMT carcinoma constitutes approximately 5–10% of oral cavity malignancies. Its true incidence is difficult to determine because tumours at this site frequently involve adjacent subsites at presentation. The disease predominantly affects males in the fifth to seventh decades.
Risk factors:
| Factor | Detail |
|---|---|
| Tobacco | Cigarette, beedi, or smokeless (pan, tobacco chewing) — major factor |
| Alcohol | Acts synergistically with tobacco |
| Betel nut / areca nut | Particularly relevant in South and Southeast Asian populations |
| Poor oral hygiene | Chronic mucosal irritation |
| Previous oral potentially malignant disorders | Leukoplakia, erythroplakia, submucous fibrosis |
| HPV | Minor role compared to oropharynx |
Pathology
Over 90% of RMT carcinomas are squamous cell carcinoma (SCC), most commonly moderately differentiated. The differential diagnosis of lesions in this region also includes:
- Minor salivary gland neoplasms (adenoid cystic, mucoepidermoid carcinoma)
- Osteosarcoma
- Soft tissue sarcomas
- Lymphoma
Histopathologic prognostic factors include depth of invasion (DOI), degree of differentiation, perineural invasion (PNI), and lymphovascular invasion. PNI is associated with a threefold increase in locoregional recurrence and can spread along the inferior alveolar nerve (V3) toward the skull base.
Clinical Features
RMT tumours most commonly present as an ulcerated or exophytic mass in the posterior oral cavity. Presenting symptoms include:
- Odynophagia / oral pain
- Trismus — due to involvement of the medial pterygoid muscle (pathognomonic of pterygoid space invasion)
- Referred otalgia — via CN IX (Jacobson's nerve)
- Lip or chin paresthesia / hypoaesthesia — perineural spread to the inferior alveolar nerve at the mandibular foramen
- Dysphagia and weight loss in advanced disease
- Cervical lymphadenopathy (present in 10–50% at presentation depending on stage)
Spread and Natural History
PRIMARY TUMOUR (Retromolar Trigone)
│
┌───────┼────────────────────────┐
▼ ▼ ▼
Buccal Faucial arch / Mandible
mucosa Tonsillar fossa (ascending ramus / body)
│ │
▼ ▼
Tongue base / Perineural (V3)
Soft palate → Skull base
│
▼
LYMPHATIC SPREAD
Level II (primary)
Level I, III (secondary)
Bilateral if midline involvement
At presentation, up to 50% of patients have regional nodal disease. Because the mucosa lies directly over periosteum, mandibular invasion is common even in early tumours. As lesions enlarge, extension to the faucial arch, tonsillar fossa, and tongue base becomes frequent.
Investigations
Clinical:
- Full head and neck examination including bimanual palpation of the floor of mouth
- Palpation of the lesion for fixation to periosteum
- Assessment of trismus (inter-incisor distance <3.5 cm is significant)
- FNA of any cervical lymphadenopathy
Imaging:
- CT with contrast (neck and chest): Best modality for cortical bone erosion and cervical nodal assessment (sensitivity 100%, accuracy 97% for mandibular cortical invasion)
- MRI: Superior for soft tissue invasion and medullary bone involvement
- PET-CT: Staging for distant metastases; complementary to CT with contrast
- Orthopantomogram (OPG/Panorex): Adjunct assessment of mandibular involvement
Histology:
- Punch biopsy from the tumour perimeter
- Avoid central biopsy of necrotic tumour
TNM Staging (AJCC 8th Edition — Oral Cavity)
T Classification (includes Depth of Invasion)
| Stage | Criteria |
|---|---|
| T1 | ≤2 cm, DOI ≤5 mm |
| T2 | ≤2 cm with DOI >5–10 mm; OR >2–4 cm with DOI ≤10 mm |
| T3 | >4 cm OR any tumour with DOI >10 mm |
| T4a | Invades cortical bone, deep tongue musculature, maxillary sinus, or skin of face |
| T4b | Invades masticator space, pterygoid plates, skull base, or encases carotid artery |
N Classification
| Stage | Criteria |
|---|---|
| N0 | No regional nodes |
| N1 | Single ipsilateral node <3 cm, ENE− |
| N2a | Single ipsilateral node <3 cm ENE+, or >3–6 cm ENE− |
| N2b | Multiple ipsilateral nodes ≤6 cm, ENE− |
| N2c | Bilateral/contralateral nodes ≤6 cm, ENE− |
| N3a | Any node >6 cm, ENE− |
| N3b | Any node with ENE+ (other criteria) |
ENE = extranodal extension. ENE-positive status upstages N classification in the 8th edition.
Management Flowchart
DIAGNOSIS OF RMT CARCINOMA
│
┌───────┴───────┐
▼ ▼
EARLY (T1–T2) ADVANCED (T3–T4)
│ │
▼ ▼
Surgery OR Surgery + Adjuvant RT
RT alone (or Chemoradiation)
│ │
▼ ▼
NECK: NECK:
Elective ND Therapeutic ND
(Levels I–III) (Levels I–IV / V)
Surgical Options by Mandibular Involvement
RMT TUMOUR
│
├─── Periosteum only / minimal cortical erosion
│ │
│ ▼
│ L-shaped MARGINAL MANDIBULECTOMY
│ (preserves mandibular continuity)
│
├─── Gross cortical / medullary bone invasion
│ │
│ ▼
│ SEGMENTAL MANDIBULECTOMY
│ (reconstruction with fibula free flap)
│
└─── Extensive involvement
│
▼
HEMIMANDIBULECTOMY
± composite resection
Surgery in Detail
Early Lesions
For T1–T2 RMT lesions, both surgery and radiation are equally effective. Surgery is generally preferred to avoid the risk of mandibular osteoradionecrosis (ORN), a debilitating complication particularly relevant given the direct proximity of tumour to bone.
Access Approaches
- Transcervical: After raising a soft tissue flap, surgical access to the ramus is obtained from below
- Translabial (lip-splitting) with lateral mandibulotomy: Used for advanced lesions requiring wider exposure
Mandibular Resection
- L-shaped coronal marginal mandibulectomy: The superior aspect of the mandibular body — extending toward the angle and ascending the ramus — is resected, preserving the inferior cortex and thus mandibular continuity (see Fig. 91.20 below). Suitable when periosteum alone or minimal cortex is involved.
- Segmental mandibulectomy: Required for gross bone destruction; creates a discontinuity defect.
- Hemimandibulectomy: For the most extensive lesions.
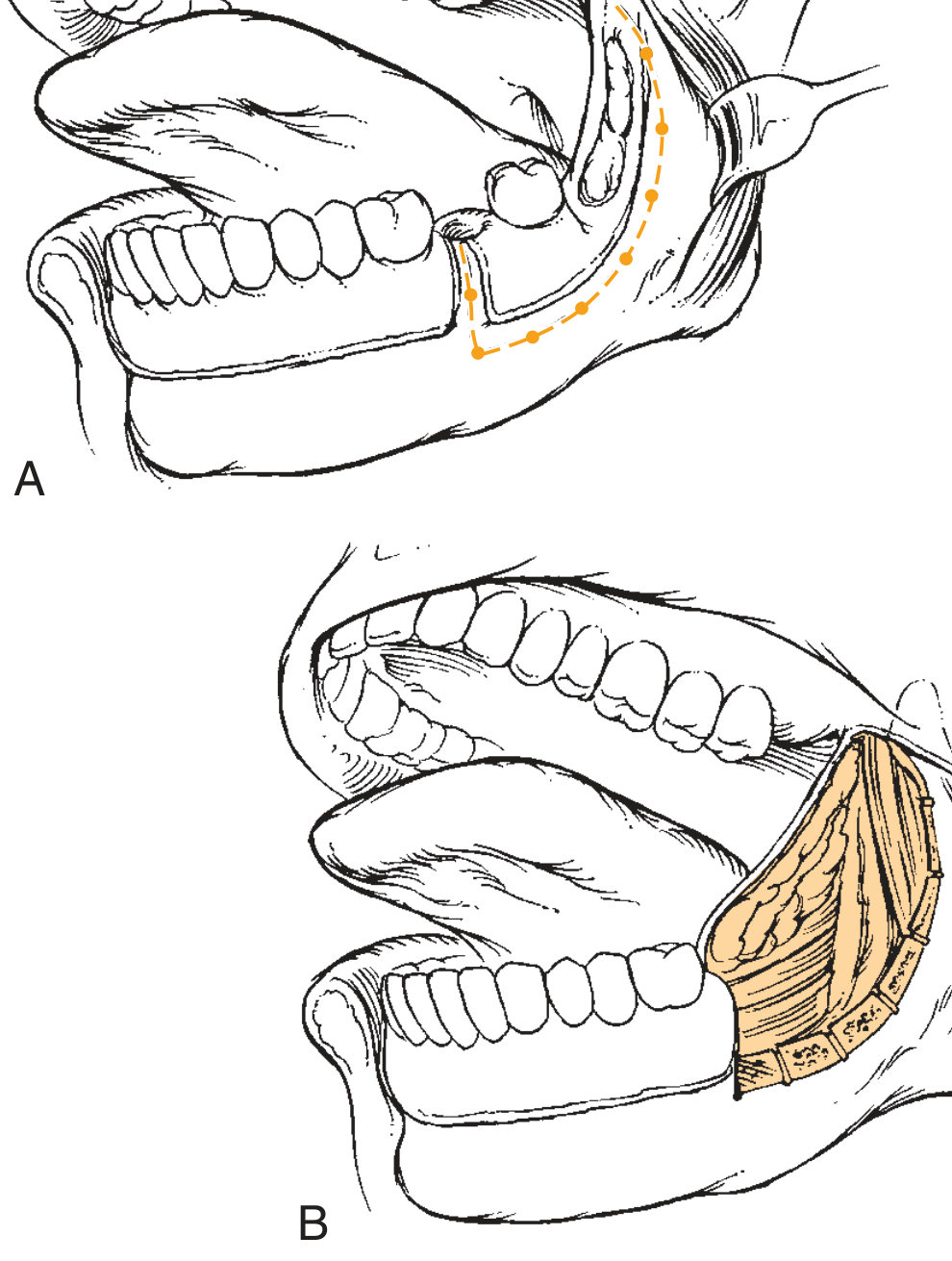
Fig. 91.20 — L-shaped marginal mandibulectomy for a retromolar trigone tumour. A generous portion of cortical bone remains at the posterior body–angle–ramus such that the defect requires only soft tissue reconstruction. (Cummings Otolaryngology)

Fig. 91.19 — Marginal mandibulectomy for a posterior alveolar ridge–retromolar trigone squamous carcinoma. (Cummings Otolaryngology)
Neck Dissection
- In patients with significant nodal risk, unilateral elective neck dissection (levels I–III) is performed even with a clinically N0 neck, given the 10–50% rate of occult metastasis
- Positive nodes require therapeutic dissection; bilateral dissection is indicated when the lesion approaches midline structures
Reconstruction
- Marginal defects: Local or regional flap (e.g., buccal fat pad, pectoralis major)
- Segmental mandibular defects: Fibula osteocutaneous free flap is the gold standard
- Mandibular bars alone are suboptimal due to high rates of hardware infection and extrusion
Radiation Therapy
- For early-stage disease (T1–T2): definitive RT is an alternative to surgery, though surgery is preferred due to ORN risk
- Postoperative RT is indicated for: positive or close margins, perineural invasion, lymphovascular invasion, multiple positive nodes, or extranodal extension
- Concurrent chemoradiation (cisplatin-based) is used for unresectable disease or as organ-preservation strategy
- Complications of RT: ORN, soft tissue necrosis, severe trismus, xerostomia
Outcomes
| Group | 5-Year Locoregional Control | 5-Year Disease-Specific Survival |
|---|---|---|
| Stages I–III (surgery + RT) | 87% | 83% |
| Stage IV (surgery + RT) | 62% | 61% |
| Overall (surgery + RT) | 71% | 69% |
Survival for T1 lesions is 76% at 5 years, declining to 54% for T4 disease. Nodal involvement dramatically worsens prognosis: N0 → 69%, N1 → 56%, N2 → 26% at 5 years. Combined surgery and postoperative radiotherapy achieves a recurrence rate of 23%, compared to 44% with radiation alone.
Summary Flowchart
RETROMOLAR TRIGONE CARCINOMA
│
Biopsy + Imaging
│
┌──────┴──────┐
▼ ▼
Resectable Unresectable
│ │
▼ ▼
Surgery Chemoradiation
± ND (Cisplatin)
│
▼
Pathology Review
│
├─ Clear margins, N0, no PNI → Observe
│
└─ +ve margins / N+ / PNI / ECE → Postop RT (± Chemo)
│
▼
Follow-up: Clinical exam
+ Imaging q3–6 months (Year 1–2)
then annually
Sources: Cummings Otolaryngology Head and Neck Surgery (pp. 1655–1666); K.J. Lee's Essential Otolaryngology (pp. 849–850)
Sialoendoscopy ENT essay answer under 1000 words with Diagrams- flowcharts
Finding Sources
Finding Sources
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.