Treatment of summer diarrhoea
Reading File
Finding Sources
Finding Sources
Searching PubMed
"acute diarrhea" AND treatment
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed. Here is a comprehensive treatment guide for summer diarrhoea:
Treatment of Summer Diarrhoea (Acute Infectious Diarrhoea)
"Summer diarrhoea" refers to acute gastroenteritis caused by ingestion of contaminated food or water during warm months, when bacterial proliferation and outdoor eating risks peak. Pathogens include Salmonella, Shigella, Campylobacter, enterotoxigenic E. coli, Vibrio, and viral agents (norovirus, rotavirus), along with protozoal causes in travellers.
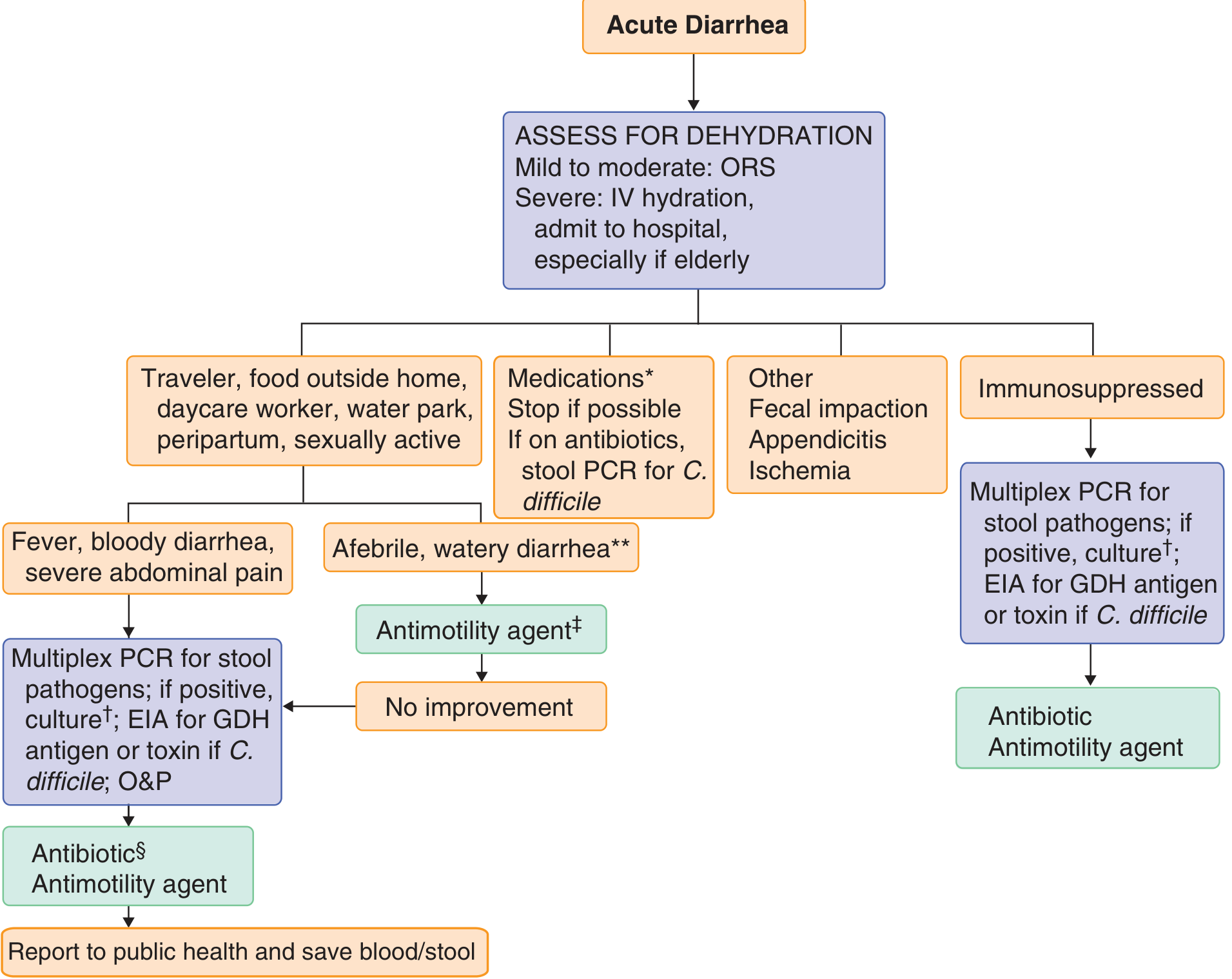
Step 1: Assess Severity and Dehydration
First priority is estimating volume depletion. Deaths from acute diarrhoea are caused by dehydration, not infection itself.
| Severity | Features | Action |
|---|---|---|
| Mild | <3 loose stools/day, no systemic signs | Oral fluids, symptomatic care |
| Moderate | 3–6 stools/day, mild dehydration, no blood/fever | ORS, consider antimotility agent |
| Severe | ≥6 stools/day, fever, bloody stools, dehydration | IV fluids, stool culture/PCR, antibiotics |
Step 2: Fluid Replacement (Most Critical Measure)
Oral Rehydration Solution (ORS)
The cornerstone of treatment. Works via intact sodium-glucose cotransporter in gut epithelium regardless of ongoing secretion.
- WHO/UNICEF standard low-osmolarity ORS (preferred for non-cholera diarrhoea): Na⁺ 75 mmol/L, glucose 75 mmol/L, K⁺ 20 mmol/L, osmolarity 245 mOsm/L
- Home preparation: ½ teaspoon salt + 6 level teaspoons sugar in 1 litre of clean water
- Children: 50–100 mL/kg over 4–6 hours; Adults: up to 1000 mL/hour
- Zinc sulfate adjunct in children: 10 mg/day (<6 months) or 20 mg/day (>6 months) — reduces severity, duration, and recurrence
- Rice-based ORS decreases stool output in cholera but not in non-cholera diarrhoea, though it still rehydrates effectively
- Reduced-osmolarity solutions are better tolerated but may cause hyponatraemia with high-volume losses — use cautiously in cholera
Intravenous Hydration
Reserved for:
- Severe dehydration with volume depletion
- Inability to tolerate oral intake
- Cholera/ETEC-type massive diarrhoea
Use Ringer's lactate or normal saline; supplement with KCl and bicarbonate as needed, transitioning to ORS once stable.
Step 3: Symptomatic (Antidiarrhoeal) Therapy
Loperamide
- Adults: 4 mg initially, then 2 mg after each unformed stool; maximum 16 mg/day
- Safe in watery, afebrile, non-bloody diarrhoea; effective in traveller's diarrhoea when combined with antibiotics
- Contraindicated in dysentery (fever + blood/pus in stool), suspected EHEC O157:H7 (risk of haemolytic uraemic syndrome), and C. difficile colitis — paralysed motility worsens invasion and toxin retention
Bismuth Subsalicylate (Pepto-Bismol)
- Adults: 524 mg every 30–60 min as needed, up to 8 doses/day (max ~4200 mg/day)
- Children (by age, every 30–60 min, max 8 doses/day):
- 3–5 yr: 87.3 mg | 6–8 yr: 175 mg | 9–11 yr: 262 mg | ≥12 yr: 524 mg
- Safe and efficacious in bacterial infectious diarrhoea; has antisecretory, antimicrobial, and anti-inflammatory effects
- Avoid in children <16 yr with chickenpox/influenza-like illness (Reye syndrome risk), in renal failure, and with anticoagulants
Racecadotril (Acetorphan)
- Adults: 100 mg three times daily; Children: 1.5 mg/kg three times daily
- Intestinal enkephalinase inhibitor — antisecretory but does NOT paralyse motility, making it safer in invasive/febrile diarrhoea
- Use if available, especially in paediatric watery diarrhoea
Adjuncts
- Antiemetics: Promethazine 12.5–25 mg orally once or twice daily
- Anxiolytics (if cramping severe): Diazepam 2 mg orally two to four times daily
- Dietary: Green bananas, pectin (amylase-resistant starch), and zinc lessen diarrhoea volume/duration in children
Step 4: Early Refeeding and Nutrition
Do not withhold food. Early refeeding is safe, well tolerated, and clinically beneficial. Malnutrition is the primary risk factor for diarrhoea-related death in developing countries. Breastfeeding should be maintained in infants (reduces diarrhoeal losses and ORS requirement).
Step 5: Antibiotics — When and Which
Most acute summer diarrhoea is viral or self-limited bacterial — antibiotics are not routinely needed. Reserve for:
| Indication | Antibiotic Choice |
|---|---|
| Moderate-severe diarrhoea with fever, bloody stools, ≥6 stools/24h, or dehydration | Empiric: Azithromycin 1 g single dose PO or 500 mg/day × 3 days (first-line, covers Campylobacter) |
| Traveller's diarrhoea | Rifaximin 200 mg PO TID × 3 days (non-invasive); Azithromycin 1 g single dose PO (invasive/febrile); Ciprofloxacin 500 mg PO BD × 3 days (resistance common in Asia) |
| Shigellosis | Ciprofloxacin 500 mg BD × 3 days PO (first-line); Azithromycin 6–20 mg/kg/day × 1–5 days (paediatric) |
| Cholera | Doxycycline 300 mg single dose (adult); Azithromycin 1 g single dose |
| Campylobacter | Azithromycin 500 mg/day × 3 days |
| C. difficile | Fidaxomicin 200 mg BD × 10 days (first-line; superior to vancomycin for preventing recurrence); Vancomycin 125 mg QID × 10 days |
| Giardia/parasites | Metronidazole or tinidazole |
| Immunocompromised patients | Always treat empirically regardless of stool appearance |
Fluoroquinolone alternatives (for resistant organisms): Azithromycin 500 mg day 1, then 250 mg/day × 4 days for resistant Shigella, Campylobacter, and traveller's diarrhoea from Mexico.
NEVER give antibiotics for EHEC O157:H7 — increases risk of haemolytic uraemic syndrome. Antimotility drugs are also contraindicated.
Step 6: Specific Pathogens — Special Considerations
- Salmonella (non-typhoidal): Antibiotics NOT indicated in immunocompetent adults (prolongs carrier state); treat only in infants, elderly, immunosuppressed, or those with vascular/orthopaedic prostheses or haemolytic anaemia
- EHEC O157:H7: Supportive care only; avoid antibiotics and antimotility agents
- C. difficile: Stop offending antibiotics; fidaxomicin preferred; fecal microbiota transplant (FMT) for recurrent cases (90% resolution vs 30% with vancomycin)
- Cryptosporidiosis: Nitazoxanide in immunocompetent patients; no effective treatment in HIV (ART is key)
Step 7: Prevention
- Judicious avoidance of contaminated food and drink; observe food expiration dates
- Strict hand hygiene — handwashing after defecation and before food handling
- Safe water and food preparation (cook to appropriate temperatures)
- Cholera vaccine for travel to endemic areas
- Zinc supplementation in malnourished children reduces diarrhoea recurrence
Sources: Goldman-Cecil Medicine (2-vol. set); Harrison's Principles of Internal Medicine, 22nd ed. (2025); ROSEN's Emergency Medicine; Sleisenger & Fordtran's GI and Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.