Calcanuem fractures and management
Reading File
Finding Sources
Searching PubMed
"calcaneus fracture" AND management
Finding Sources
Searching PubMed
"calcaneal fracture" AND surgery
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive material to write a complete, well-structured answer. Here it is:
Calcaneum (Calcaneus) Fractures
Epidemiology
The calcaneus is the most commonly fractured tarsal bone, accounting for 65% of tarsal injuries and 2% of all skeletal fractures, with an incidence of approximately 11.5 per 100,000 population per year. Fractures occur most commonly in young, active working males aged 20-29. In older women (>50), the incidence rises due to low-energy falls on osteoporotic bone. Up to 75% are intra-articular, and 3-7.9% are bilateral. Associated injuries are seen in 25-50% of cases, including lumbar spine fractures (6-20%), pilon fractures, ankle fractures, and femoral fractures. Alcohol use is associated with 20% of cases.
- Rockwood and Green's Fractures in Adults, 10th ed. 2025, p. 3412
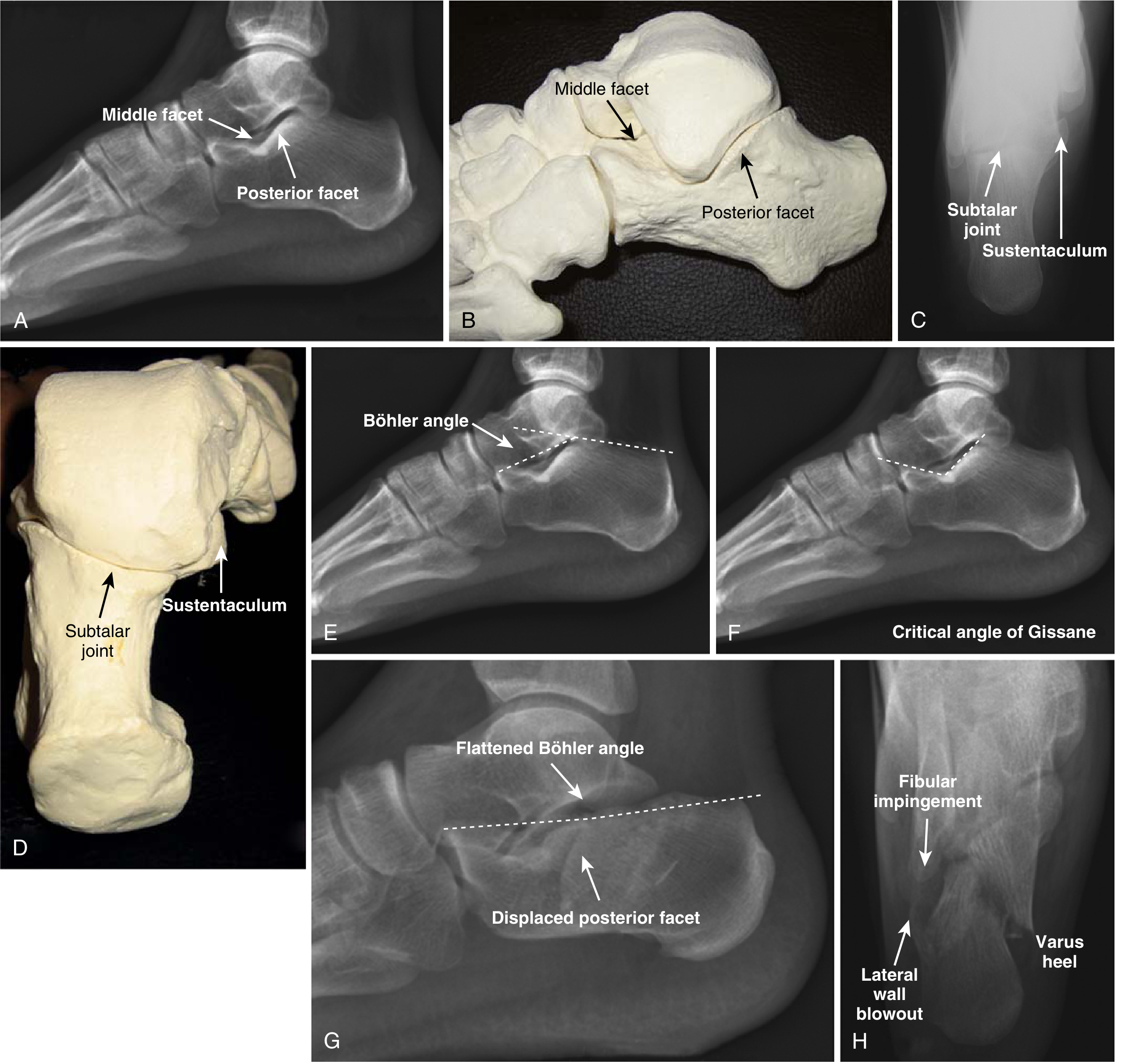
Anatomy
The calcaneus is the largest tarsal bone with four articulating facets:
- Three superior facets (posterior, middle, anterior) articulating with the talus
- One anterior facet articulating with the cuboid (calcaneocuboid/CC joint)
Key landmarks:
- Sustentaculum tali - located 2.5 cm below the medial malleolus; contains the FHL tendon groove inferiorly; remains attached to the talus by the deltoid and interosseous talocalcaneal ligaments (this is the "constant fragment" in fractures)
- Critical angle of Gissane - the lateral cortical strut from the anterior process to the posterior facet; normal 120-145 degrees
- Bohler's angle - formed on lateral radiograph; normal 25-40 degrees; reduction indicates posterior facet collapse
- Rockwood and Green's, p. 3424 | Miller's Review of Orthopaedics 9th ed., p. 621
Mechanism of Injury
- Intra-articular (75%): High-energy axial loading - falls from height, motor vehicle collisions. The lateral process of the talus acts as a wedge, driving into the calcaneus and splitting it into primary and secondary fracture lines.
- Extra-articular (25%): Include tuberosity avulsions (forceful Achilles contraction), anterior process avulsions (forced inversion/plantarflexion at the bifurcate ligament), and sustentaculum fractures.
Resulting deformity: The calcaneus becomes shortened, widened, and varus. The lateral wall "blows out" causing subfibular and peroneal tendon impingement. Posterior facet collapses with loss of Bohler's angle.
Classification
Essex-Lopresti (plain radiograph based)
- Joint depression type - secondary fracture line exits posteriorly above the Achilles insertion
- Tongue type - secondary fracture exits below the Achilles insertion, producing a large tongue fragment attached to the tuberosity
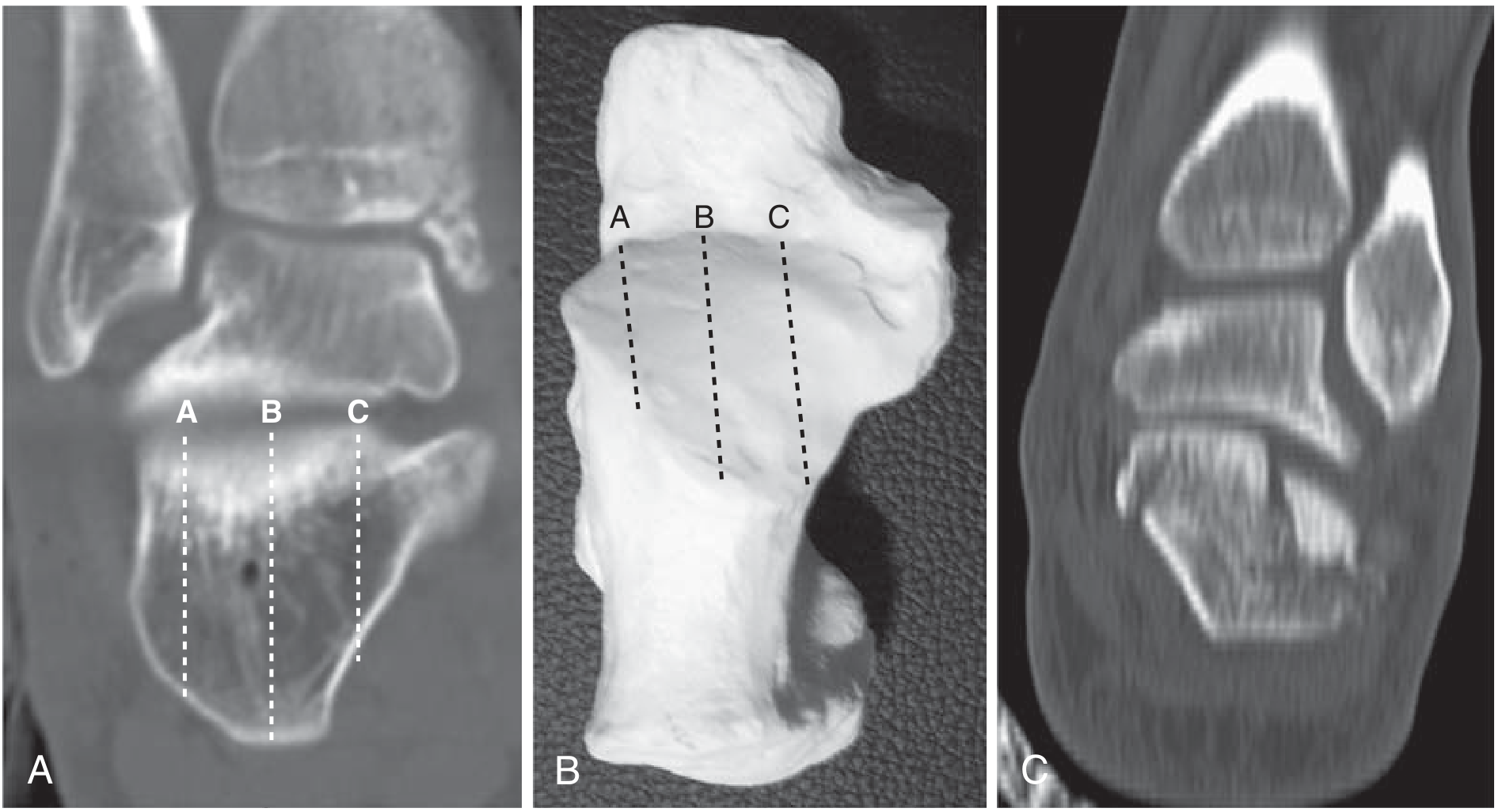
Sanders Classification (CT-based, most widely used)
Based on the number of fracture lines through the posterior facet on coronal CT:
| Type | Description | Treatment |
|---|---|---|
| I | Non-displaced (any number of lines) | Non-operative |
| II | 2-part posterior facet fracture (IIA, IIB, IIC) | ORIF generally recommended |
| III | 3-part fracture (IIIAB, IIIAC, IIIBC) | ORIF; consider primary subtalar fusion |
| IV | Highly comminuted (4+ fragments) | ORIF + primary subtalar arthrodesis |
- Miller's Review of Orthopaedics 9th ed., p. 622
Imaging Evaluation
Plain Radiographs
- Lateral hindfoot view - confirms fracture, assesses Bohler's angle, classifies tongue vs. joint depression type; identifies anterior process fractures
- Harris axial heel view - shows tuberosity displacement, varus angulation, fibular abutment, lateral wall blowout
- Broden views (ankle internal rotation 15-40 degrees with X-ray beam centered 35 degrees cephalad) - evaluates posterior facet displacement
CT Scan (mandatory for intra-articular fractures)
- Semicoronal (30-degree) plane - posterior and middle facet displacement
- Axial plane - CC joint involvement
- Sagittal plane - tuberosity displacement
CT is essential for Sanders classification, pre-operative planning, and detection of sustentaculum fractures.
- Rockwood and Green's, p. 3420
Management
Extra-articular Fractures
Tuberosity avulsion fractures:
- Non-displaced: immobilization
- Displaced (tenting skin): emergent percutaneous fixation with lag screws from posterior superior tuberosity directed inferior and distal - skin compromise risk is a surgical emergency
Anterior process fractures:
- Often misdiagnosed as ankle sprains
- Most: immobilization in boot/brace
-
25% CC joint involvement or significant displacement: ORIF
- Symptomatic nonunion: fragment excision
Sustentaculum fractures:
- Rarely isolated; usually with posterior facet involvement
- Displaced: ORIF via lag screws through a medial approach
Intra-articular Fractures (Displaced)
Non-operative Treatment
Indications: non-displaced fractures (Sanders I), medically unfit patients, elderly low-demand patients with minimal deformity, patients with severe peripheral vascular disease/diabetes where wound risk is prohibitive.
Protocol: Non-weight-bearing for 6-8 weeks, early ROM of ankle/subtalar joint (to prevent stiffness), gradual return to weight-bearing.
Operative Treatment
Timing: Surgery should be delayed 10-21 days until soft tissue swelling subsides. The "wrinkle sign" (skin wrinkles present over lateral hindfoot) confirms readiness. Operating through swollen tissue dramatically increases wound complications.
Contraindications to surgery: Uncontrolled diabetes, smoking (relative), severe peripheral vascular disease, open wounds, medical instability.
Surgical Approaches
1. Extensile Lateral Approach (ELA)
- Full-thickness L-shaped flap over lateral hindfoot
- Excellent visualization of subtalar and CC joints, allows plate fixation
- Wound complication rate: 25-30% (delayed healing); deep infection 1-4%
- Complications increase in smokers, diabetics, open fractures
2. Sinus Tarsi Approach (STA) - increasingly preferred
- Smaller incision over the sinus tarsi
- Lower wound complication rate
- Requires good understanding of fracture anatomy; malreduction risk if technique is not mastered
- Can be used within 0-2 weeks of injury (before callus formation makes fragment mobilization difficult)
- Recent meta-analyses confirm significantly lower wound complication rates vs. ELA
3. Percutaneous techniques
- For tongue-type fractures and some simpler Sanders II fractures
- Minimal soft tissue disruption
Treatment by Sanders Type
- Type I: Non-weight-bearing 6 weeks, early ROM, no surgery
- Type II & III: ORIF (ELA or STA); primary subtalar arthrodesis if articular cartilage is destroyed or fracture is highly comminuted
- Type IV: ORIF + primary subtalar arthrodesis is the treatment of choice
Operative fixation typically uses lateral-to-medial 3.5 or 4.0 mm cortical screws targeting the sustentacular fragment (constant fragment). Low-profile locking plates are used with the ELA.
Open Calcaneus Fractures
- Standard open fracture protocol: IV antibiotics, tetanus prophylaxis, urgent washout and debridement
- Bony stabilization with external fixator, K-wires, or Schanz pins
- Definitive fixation deferred until clean wound bed achieved (reassess every 48-72 hours)
- Plastic surgery early involvement - 5-8% eventual below-knee amputation rate
- Average 2.8 procedures per open calcaneal fracture
Postoperative Protocol (ORIF)
- Splint for 1 week → wound check → cast
- Non-weight-bearing with limb elevation
- Sutures removed ~2 weeks
- CAM boot and gentle ROM at 6 weeks
- Progressive weight-bearing from 10-12 weeks
Complications
| Complication | Notes |
|---|---|
| Wound dehiscence/infection | Most common after ELA; 25-30% wound issues, 1-4% deep infection |
| Calcaneal osteomyelitis | Serious; may require debridement, flap coverage |
| Posttraumatic subtalar arthritis | Most common long-term complication; 50% decreased subtalar ROM regardless of treatment |
| Peroneal tendon impingement/dislocation | From lateral wall blowout; 20% have peroneal dislocation |
| Calcaneal malunion | Shortened, widened, varus calcaneus; may need corrective osteotomy or subtalar arthrodesis |
| Subfibular impingement | From persistent lateral wall expansion |
| Nerve entrapment/cutaneous nerve injury | Sural nerve most at risk with lateral approaches |
| Heel pad pain | From fat pad crush injury |
| Anterior ankle pain | From horizontal talus and reduced declination; may need bone-block distraction arthrodesis |
Prognosis
- Patients can be totally incapacitated up to 3 years and partially impaired up to 5 years
- Outcomes improve with operative management in: significant intra-articular displacement, flattened Bohler's angle, female sex, age <29, non-workers' compensation cases
- Secondary subtalar arthrodesis after primary ORIF has better outcomes than fusion after failed non-operative management (due to better preserved calcaneal height and width)
- Bone-block distraction arthrodesis of the subtalar joint is needed when significant calcaneal height loss has produced a horizontal talus with anterior ankle impingement
- Rockwood and Green's Fractures in Adults, 10th ed. 2025 | Miller's Review of Orthopaedics 9th ed.
Recent Evidence Note
A 2026 systematic review (PMID: 40375052) supports primary subtalar arthrodesis in severely displaced intra-articular calcaneal fractures. A 2024 meta-analysis (PMID: 38729077) confirms the sinus tarsi approach has significantly lower wound complication rates than the extensile lateral approach, reinforcing its growing adoption as the preferred technique.
This is a shared conversation. Sign in to Orris to start your own chat.