Liver cirosis note
Reading File
Finding Sources
Searching PubMed
"liver cirrhosis"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I have all the information needed for a comprehensive note. Let me now compose the full liver cirrhosis clinical note.
Liver Cirrhosis - Clinical Notes
Definition
Cirrhosis refers to the diffuse transformation of the liver into regenerative parenchymal nodules surrounded by fibrous bands. It represents the end stage of any chronic liver disease. It is not a specific diagnosis - it is a morphologic endpoint with variable causes, courses, and prognoses. Notably, not all chronic liver disease terminates in cirrhosis, and not all cirrhosis leads to end-stage liver failure (e.g., patients with cured hepatitis C or treated autoimmune hepatitis may have adequate function despite cirrhosis).
- Robbins & Kumar Basic Pathology, p. 598
- Goldman-Cecil Medicine, p. 1614
Etiology
Main causes (>90% of cases):
| Cause | Notes |
|---|---|
| Alcoholic liver disease | Most common in Western countries |
| Non-alcoholic fatty liver disease (NAFLD/MASLD) | Increasingly common worldwide |
| Chronic hepatitis B | Leading cause globally |
| Chronic hepatitis C | Previously major cause; now curable |
Less common causes (each <2%):
- Cholestatic/autoimmune: Primary biliary cirrhosis, primary sclerosing cholangitis, autoimmune hepatitis
- Mechanical obstruction: Biliary atresia, cystic fibrosis
- Metabolic: Hemochromatosis, Wilson disease, alpha-1 antitrypsin deficiency, glycogen storage diseases, porphyria
- Hepatic venous outflow obstruction: Budd-Chiari syndrome, veno-occlusive disease, right heart failure
- Drugs and toxins, intestinal bypass
- Cryptogenic cirrhosis - no identifiable cause found
Pathogenesis
Hepatic Stellate Cell Activation
The key pathogenic event is activation of hepatic stellate cells (Ito cells / perisinusoidal cells):
- Normally located in the space of Disse between hepatocytes and sinusoidal endothelium
- In the quiescent state, serve as the main hepatic storage site for retinoids (vitamin A)
- Upon injury: they become activated, lose vitamin A, proliferate, develop prominent rough ER, and secrete extracellular matrix (collagen types I and III, sulfated proteoglycans, glycoproteins)
- They also transform into contractile myofibroblasts, contributing to sinusoidal vasoconstriction
Capillarization of Sinusoids
Collagen deposition in the space of Disse leads to defenestration of sinusoidal endothelial cells ("capillarization"), reducing the diameter of sinusoids and impairing exchange between plasma and hepatocytes.
- Goldman-Cecil Medicine, p. 1615
Morphology
Gross appearance:
- Entire liver transformed into regenerative parenchymal nodules surrounded by fibrous bands
- Orange-tawny color, irregular surface, nodular texture
- Contrast with normal liver: smooth surface, homogeneous texture
Microscopically:
- Disorganized architecture with regenerative nodules surrounded by fibrous tissue
- Ductular reactions (stem cell-derived duct-like structures) become increasingly prominent
- Pattern of scarring varies: portal-to-portal bridging vs. portal-to-central vein bridging

Gross specimen of cirrhotic liver from chronic viral hepatitis (Robbins & Kumar Basic Pathology)
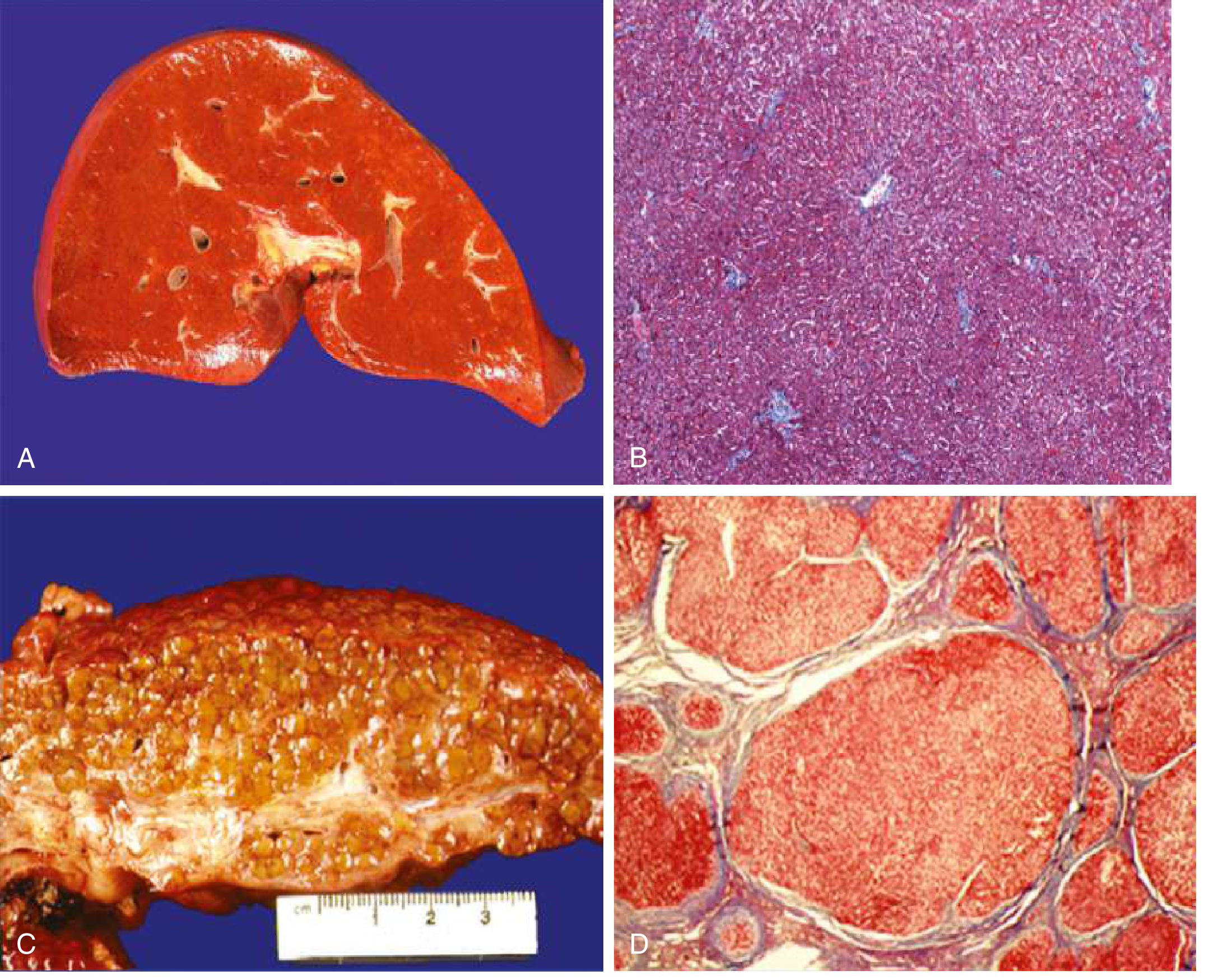
A: Normal liver gross - smooth, homogeneous. B: Normal microscopically - organized sinusoids. C: Cirrhotic liver gross - orange-tawny, nodular. D: Cirrhotic microscopically - disorganized architecture, regenerative nodules in fibrous septa (Goldman-Cecil Medicine)
Reversibility
Regression of fibrosis - and even of established cirrhosis - can occur after disease remission or cure. Scars become thinner, more compacted, fragment, and adjacent nodules coalesce. All cirrhotic livers show both progression and regression, with the balance dictated by the severity and persistence of the underlying disease.
Clinical Staging: Compensated vs. Decompensated
| Stage | Definition | Dominant Mechanism |
|---|---|---|
| Compensated | No major complications; may be asymptomatic | Sinusoidal hypertension |
| Decompensated | Development of ascites, variceal hemorrhage, encephalopathy, or jaundice | Portal hypertension + liver insufficiency |
About 40% of patients with cirrhosis are asymptomatic until the most advanced stages, presenting with nonspecific features: anorexia, weight loss, weakness.
Complications
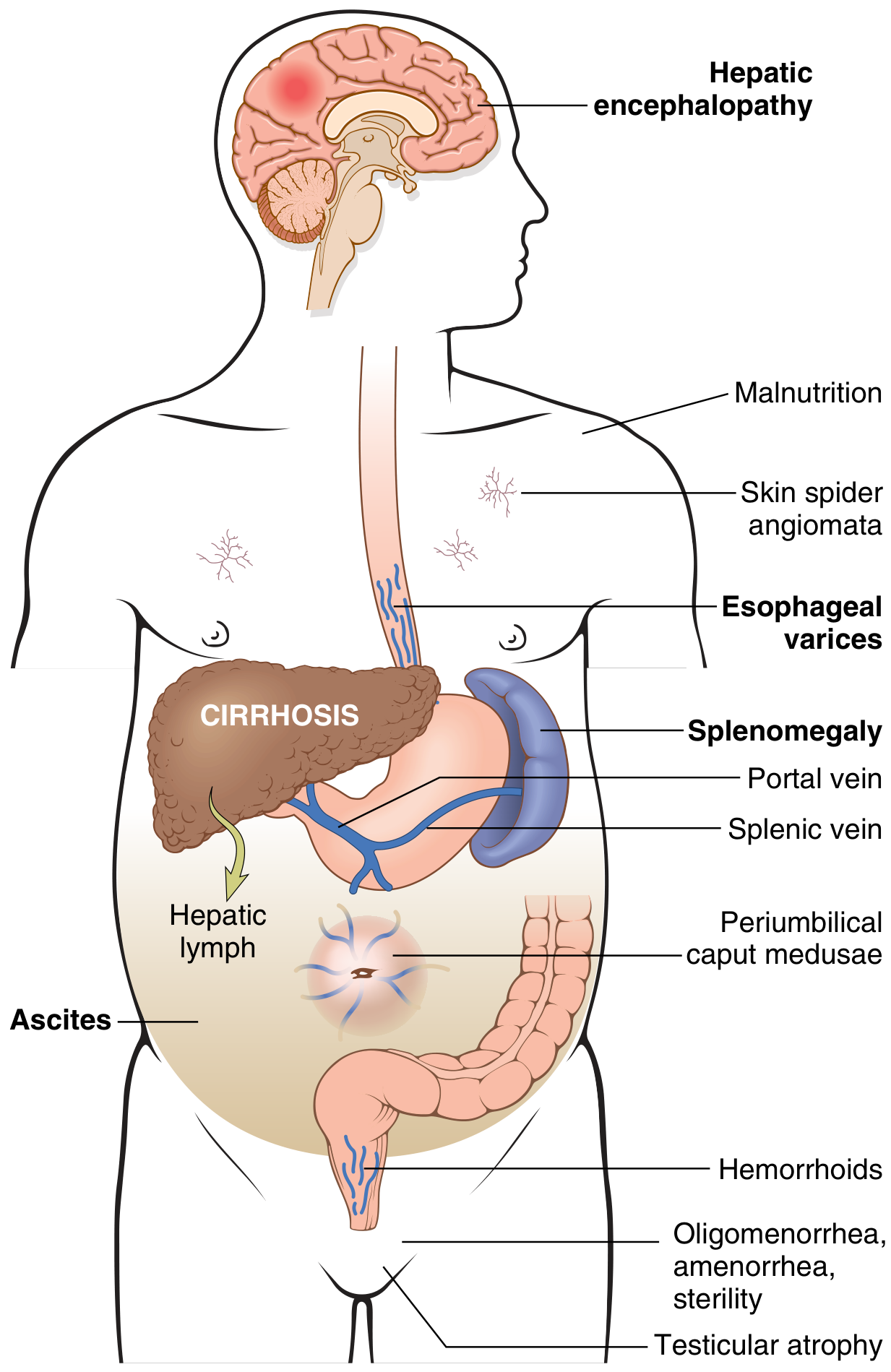
Systemic manifestations of portal hypertension and liver insufficiency in cirrhosis (Robbins & Kumar Basic Pathology)
The two main pathophysiologic consequences are portal hypertension (with hyperdynamic circulation) and liver insufficiency:
1. Portal Hypertension
Mechanism - dual component:
- Fixed component: Fibrosis and compression by regenerative nodules increase sinusoidal resistance
- Functional component: Active vasoconstriction from intrahepatic NO deficiency and enhanced vasoconstrictors; amenable to vasodilators
Consequences:
- Splenomegaly and hypersplenism - congestive enlargement (up to 1000g); thrombocytopenia, pancytopenia
- Portosystemic collaterals / varices - esophagogastric varices form in ~40% of advanced disease; risk of massive hematemesis. A 2025 systematic review (PMID 40597728) addressed optimal endoscopy timing in acute variceal bleeding
- Ascites - peritoneal fluid accumulation; transudate with <3 g/dL protein; serum-to-ascites albumin gradient ≥1.1 g/dL; ~85% of all ascites is due to cirrhosis
- Caput medusae - periumbilical venous distension
- Hemorrhoids - from inferior mesenteric vein collaterals
2. Liver Insufficiency
- Jaundice - inability to excrete bilirubin; chronic severe jaundice causes pruritus (from bile salt accumulation)
- Coagulopathy - reduced synthesis of clotting factors
- Hypoalbuminemia - contributing to edema and ascites
- Hyperestrogenemia (impaired estrogen catabolism in males) causing: spider angiomas, palmar erythema, gynecomastia, testicular atrophy, loss of axillary/chest hair
- Encephalopathy (result of both portal hypertension AND liver insufficiency - see below)
3. Spontaneous Bacterial Peritonitis (SBP)
- About 1/3 of hospitalized patients with cirrhosis have or develop bacterial infection
- SBP is the most common; key predictors: severity of liver disease, GI hemorrhage on admission
- Manifestations: fever, jaundice, abdominal pain/tenderness; up to 1/3 initially present without abdominal symptoms (encephalopathy, AKI, or shock instead)
4. Hepatic Encephalopathy (HE)
- Occurs at ~2-3% per year in cirrhosis
- Wide spectrum from subclinical to coma:
| Grade | Features |
|---|---|
| 1 | Sleep-wake inversion, forgetfulness, distal tremor |
| 2 | Confusion, bizarre behavior, disorientation |
| 3 | Lethargy, profound disorientation |
| 4 | Coma |
- Hallmark sign: asterixis (flapping tremor)
- Characteristic breath: fetor hepaticus (sweet-smelling)
5. Pulmonary Complications
- Hepatopulmonary syndrome (HPS): exertional dyspnea, clubbing, cyanosis, vascular spiders; present in 5-10% awaiting transplant
- Portopulmonary hypertension: exertional dyspnea, syncope, chest pain; accentuated P2, right ventricular heave
Physical Examination Findings
Signs of liver insufficiency / hyperdynamic state:
- Muscle atrophy (bitemporal, thenar, hypothenar)
- Spider angiomas (trunk, face, upper limbs)
- Palmar erythema (thenar, hypothenar, fingertips)
- Gynecomastia, testicular atrophy, loss of body hair (males)
- Petechiae, ecchymoses (thrombocytopenia / coagulopathy)
- Jaundice, scleral icterus
Signs of portal hypertension:
- Splenomegaly
- Ascites (shifting dullness, fluid wave)
- Caput medusae
- Fetor hepaticus
Diagnosis
Gold standard: liver biopsy - but invasive and subject to sampling error.
Non-invasive assessment (increasingly preferred):
- Serum biomarkers (e.g., FIB-4 index, APRI score, FibroTest)
- Imaging: ultrasound (nodular surface, caudate lobe hypertrophy, splenomegaly, ascites), CT, MRI
- Liver stiffness measurement (transient elastography / FibroScan) - now the preferred non-invasive tool
Laboratory findings in cirrhosis:
- Elevated AST, ALT (may be near-normal in end-stage)
- Elevated bilirubin
- Elevated INR / prolonged PT
- Low albumin
- Thrombocytopenia (hypersplenism)
- Low sodium (dilutional hyponatremia)
Prognosis / Scoring Systems
| Score | Components | Use |
|---|---|---|
| Child-Pugh | Bilirubin, albumin, PT/INR, ascites, encephalopathy | Overall liver reserve; transplant listing |
| MELD (Model for End-stage Liver Disease) | Creatinine, bilirubin, INR, Na | Organ allocation; predicts 90-day mortality |
Key Principles of Management
Management targets the underlying etiology and its complications:
| Complication | Management |
|---|---|
| Ascites | Salt restriction, diuretics (spironolactone ± furosemide), large-volume paracentesis ± albumin, TIPS for refractory ascites |
| Variceal hemorrhage | Beta-blockers (propranolol/carvedilol) for prophylaxis; acute: vasoactive drugs (terlipressin/octreotide) + endoscopic band ligation; TIPS for refractory cases |
| SBP | IV cefotaxime (or alternatives); norfloxacin prophylaxis in high-risk patients |
| Hepatic encephalopathy | Lactulose (first-line); rifaximin (second-line / maintenance); identify and treat precipitants |
| Hepatorenal syndrome | Vasoconstrictors (terlipressin + albumin); bridge to transplant |
| Definitive treatment | Liver transplantation |
Sources
- Robbins & Kumar Basic Pathology (9780323790185), pp. 598-602
- Goldman-Cecil Medicine International Edition (9780323930345), Chapter 139, pp. 1614-1620
- Luo S et al. "Timing of endoscopy in patients with acute variceal bleeding in cirrhosis: updated systematic review and meta-analysis." BMC Gastroenterol 2025 PMID: 40597728
This is a shared conversation. Sign in to Orris to start your own chat.