leucorrhea disease cash tracking of symptom
Reading File
Finding Sources
Searching the Web
leucorrhea symptoms classification causes treatment clinical
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information. Let me compile the full clinical answer on leucorrhea.
Leucorrhea — Clinical Overview & Symptom Tracking
Leucorrhea (also spelled leucorrhoea) refers to a white or yellowish vaginal discharge. It may be physiologic (normal) or pathologic (a sign of underlying disease). Tracking symptoms is key to identifying the cause and directing treatment.
1. Physiologic Leucorrhea
Normal vaginal discharge is white or transparent, thick, and mostly odorless. It increases in these states:
- Pregnancy
- Mid-cycle ovulation (estrogen surge)
- Use of estrogen-progestin oral contraceptives
- Neonates (first 2–3 weeks of life — thin, clear/white, self-limited)
Normal vaginal pH is 3.8–4.4, maintained by lactobacilli; this is hostile to pathogens.
2. Pathologic Leucorrhea — Causes & Symptom Tracking
Candidiasis, bacterial vaginosis (BV), and trichomoniasis account for 90% of vaginitis cases. Use the following symptom comparison for tracking:
Comparison Table (from Textbook of Family Medicine 9e)
| Type | Symptoms | Discharge Appearance | Vaginal pH | KOH Test | Wet Mount |
|---|---|---|---|---|---|
| Bacterial Vaginosis | Malodorous discharge | Thin, gray, adherent | >4.5 | Amine/fishy odor (positive) | Clue cells |
| Vulvovaginal Candidiasis | Itching, burning, pain | Curd-like, thick white | 3.8–4.5 | Pseudohyphae, budding yeast | Occasional hyphae/yeast |
| Trichomoniasis | Fish-odor discharge, purulent | Profuse, yellow, purulent | 6–7 | Negative | Motile trichomonads, many WBCs |
| Atrophic Vaginitis | Dryness, pain | Pale, scanty | >4.5 | Negative | RBCs, WBCs, many bacteria |
| Aerobic Vaginitis | Foul odor | Heavy, purulent | >4.5 | Negative | Cocci or coarse rods |
| Irritant/Allergic | Itching, swelling | Erythema | Any | Negative | Negative |
| Physiologic (Leukorrhea) | No odor, no pruritus | Clear/white, varies with cycle | Normal | Negative | Normal flora |
— Textbook of Family Medicine 9e, p. 619
3. Full Differential Diagnosis of Vaginal Discharge
- Bacterial vaginosis (BV) — most common cause, ~50% of infections
- Candida albicans / C. glabrata — most common cause of vulvar pruritus
- Trichomonas vaginalis — STI, flagellated protozoan
- Chlamydial infection or gonorrhea (cervicitis) — often asymptomatic
- Allergic/contact vaginitis
- Erosive lichen planus
- Desquamative inflammatory vaginitis
- Atrophic vaginitis (post-menopausal)
- Vaginal foreign body (especially in children — toilet paper is most common)
- Actinomyces / Behçet syndrome (IUD-associated)
- Vulvar vestibulitis
- Cervical malignancy
4. Diagnosis Algorithm
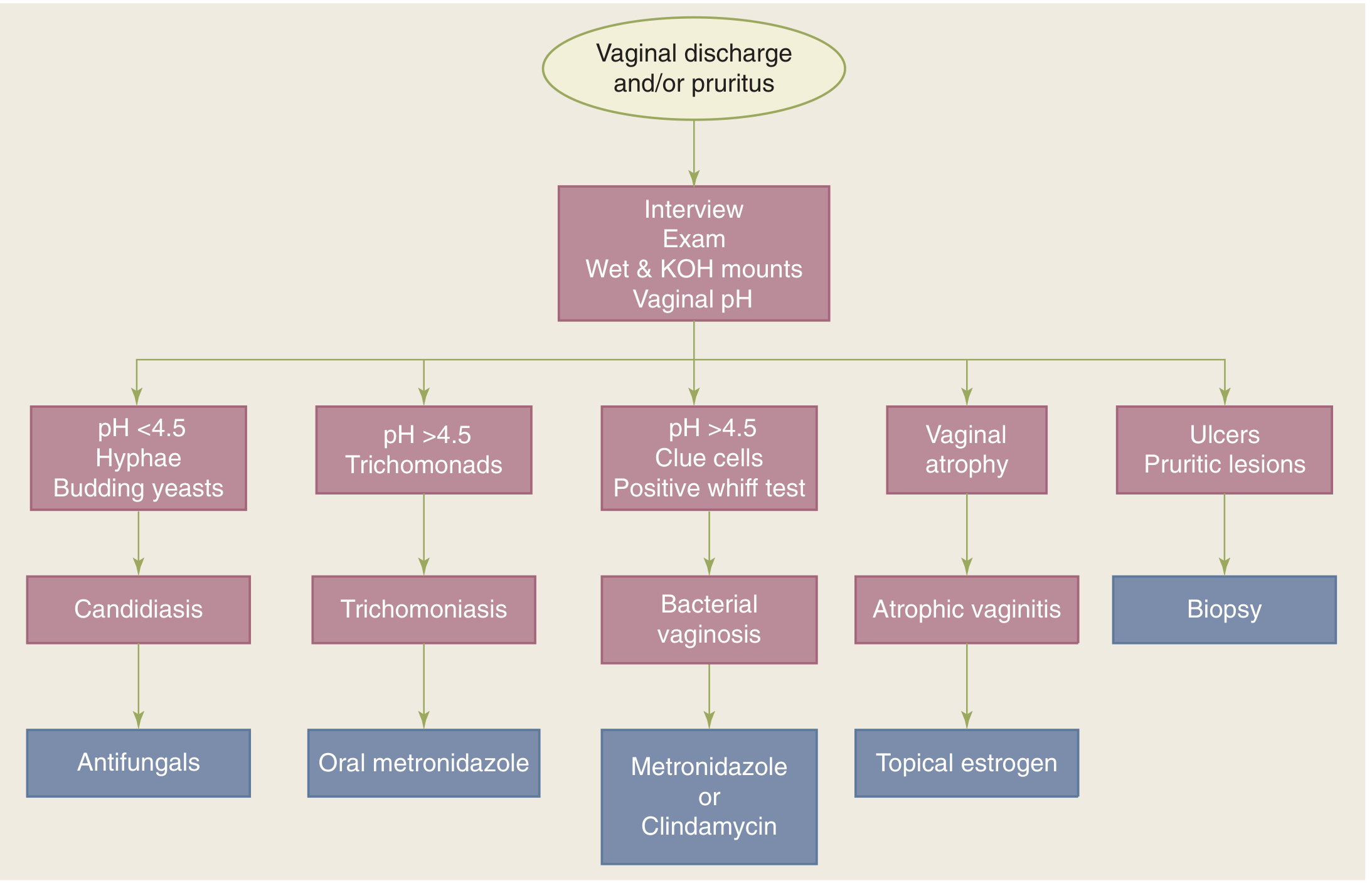
— Schwartz's Principles of Surgery, 11th Ed.
Workup steps:
- History + pelvic examination
- Vaginal pH testing
- Wet mount (saline) and KOH microscopy
- Whiff test (amine odor with KOH → BV)
- NAAT for Chlamydia trachomatis and N. gonorrhoeae
- Culture if microscopy is negative
Amsel Criteria for BV (3 of 4 required):
- Vaginal pH >4.5
- Clue cells >20% on wet mount
- Homogeneous gray adherent discharge
- Positive whiff test
5. Treatment Summary
| Condition | First-Line Treatment |
|---|---|
| Bacterial Vaginosis | Metronidazole 500 mg PO twice daily × 7 days, OR metronidazole gel/clindamycin 2% cream intravaginally |
| Trichomoniasis | Metronidazole 2 g single oral dose (7-day preferred) or tinidazole; treat partners |
| Vulvovaginal Candidiasis | Topical antifungals (azoles); single-dose oral fluconazole also effective |
| Atrophic Vaginitis | Topical estrogen cream |
| Physiologic Leucorrhea | Reassurance; no treatment needed |
| Prepubertal vulvovaginitis | Hygiene measures; short-course topical estrogen + broad-spectrum antibiotics if needed |
Key notes:
- pH ≥4.9 indicates bacterial or protozoal infection
- Douching is not helpful for prevention or treatment
- Treating T. vaginalis partners is standard of care to prevent reinfection
- In developing-country syndromic management: 7-day metronidazole covers BV + trichomoniasis
- Most chlamydial/gonococcal cervical infections are asymptomatic — do not rely on discharge alone
6. Symptom Tracking Checklist (Clinical Use)
To track leucorrhea systematically, document:
| Parameter | Details to Record |
|---|---|
| Onset | When did discharge start? Acute vs. chronic |
| Color | White, gray, yellow, green, brown, bloody |
| Consistency | Thin/watery, thick/curdy, homogeneous, frothy |
| Odor | None, fishy/amine, foul |
| Volume | Increased vs. baseline |
| Associated symptoms | Pruritus, burning, dysuria, pelvic pain, dyspareunia |
| Menstrual cycle relation | Mid-cycle, premenstrual, post-coital |
| Sexual history | New partner, STI exposure, condom use |
| Medications/hygiene | Antibiotics, douching, soaps, IUD use |
| Pregnancy status | LMP, contraception |
| Age group | Prepubertal, reproductive, postmenopausal |
Sources: Textbook of Family Medicine 9e, pp. 619–620 | Schwartz's Principles of Surgery 11e | Harrison's Principles of Internal Medicine 22e | Tintinalli's Emergency Medicine | Berek & Novak's Gynecology
This is a shared conversation. Sign in to Orris to start your own chat.