fever, confusion, photophobia, neck stiffness, headaches, fatigue, somnolent, diarrhea, slurred speech, difficulty walking, intermittent incontinence of urine and stool, chills, diffuse hyperreflexia, myoclonic jerks, immunocompromised,
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
meningoencephalitis immunocompromised fever myoclonus hyperreflexia
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
viral encephalitis immunocompromised diagnosis treatment
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Searching the Web
immunocompromised patient fever confusion neck stiffness myoclonic jerks hyperreflexia differential diagnosis encephalitis 2024
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Now I have sufficient information for a comprehensive analysis. Let me synthesize.
Clinical Analysis: Meningoencephalitis in an Immunocompromised Host
This constellation of symptoms constitutes a medical emergency. The combination of meningeal signs + encephalopathy + upper motor neuron signs + incontinence in an immunocompromised patient demands urgent workup and empiric treatment.
Syndromic Localization
| Finding | Implication |
|---|---|
| Fever + neck stiffness + photophobia + headache | Meningeal irritation |
| Confusion + somnolence + slurred speech + difficulty walking | Diffuse cortical + cerebellar/brainstem involvement |
| Diffuse hyperreflexia + myoclonic jerks | Upper motor neuron / corticospinal tract involvement |
| Intermittent incontinence (urine + stool) | Myelopathic or frontal lobe dysfunction |
| Diarrhea + chills | Systemic/prodromal infectious illness |
Syndrome: Meningoencephalomyelitis — inflammation spanning meninges, cortex, and spinal cord.
Differential Diagnosis (Prioritized by Likelihood in Immunocompromised)
🔴 MOST URGENT — Must Rule Out Immediately
1. Herpes Simplex Encephalitis (HSV-1 or HSV-2)
The top priority to treat empirically regardless of immune status. HSV-1 has a predilection for the temporal lobe and limbic system. In immunocompromised patients, presentation can be more diffuse and fulminant.
- Classic signs: Acute fever, focal neurologic deficits, temporal lobe involvement on MRI
- CSF: Lymphocytic pleocytosis, elevated protein, RBCs (hemorrhagic necrosis), HSV PCR positive
- Treatment: IV acyclovir 30 mg/kg/day in 3 divided doses × 14–21 days — start empirically without waiting for confirmatory results (Harrison's 22e)
2. Bacterial Meningitis / Meningoencephalitis
- Key organisms in immunocompromised: Listeria monocytogenes, Streptococcus pneumoniae, gram-negative bacilli, Staphylococcus aureus
- Listeria specifically causes rhombencephalitis (brainstem encephalitis): cranial nerve palsy, cerebellar ataxia, altered mental status — highly relevant given the slurred speech and gait difficulty
- Treatment: Empiric ampicillin + ceftriaxone + dexamethasone — do NOT delay for imaging if clinical suspicion is high
🟠 HIGH PRIORITY — Immunocompromised-Specific
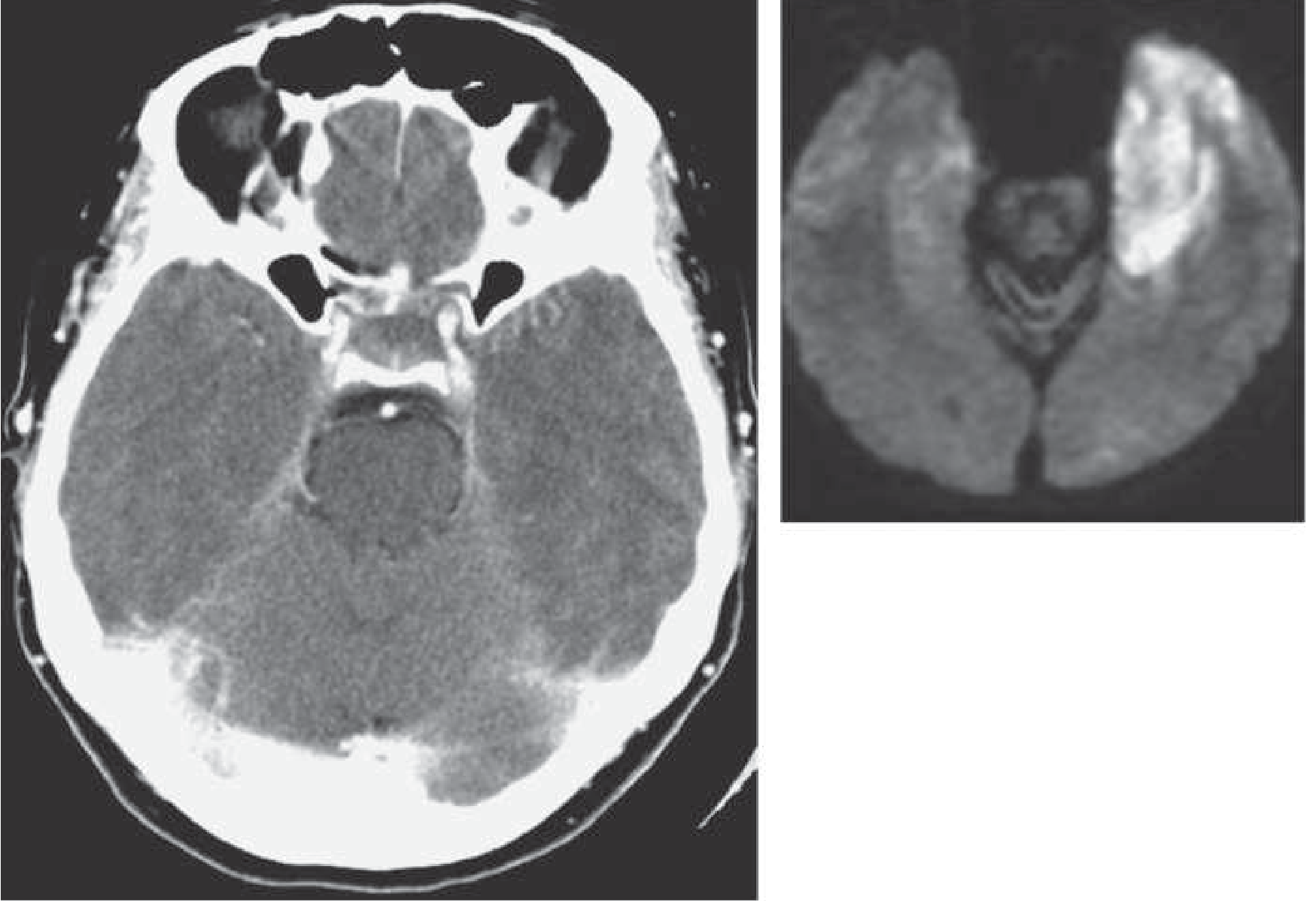
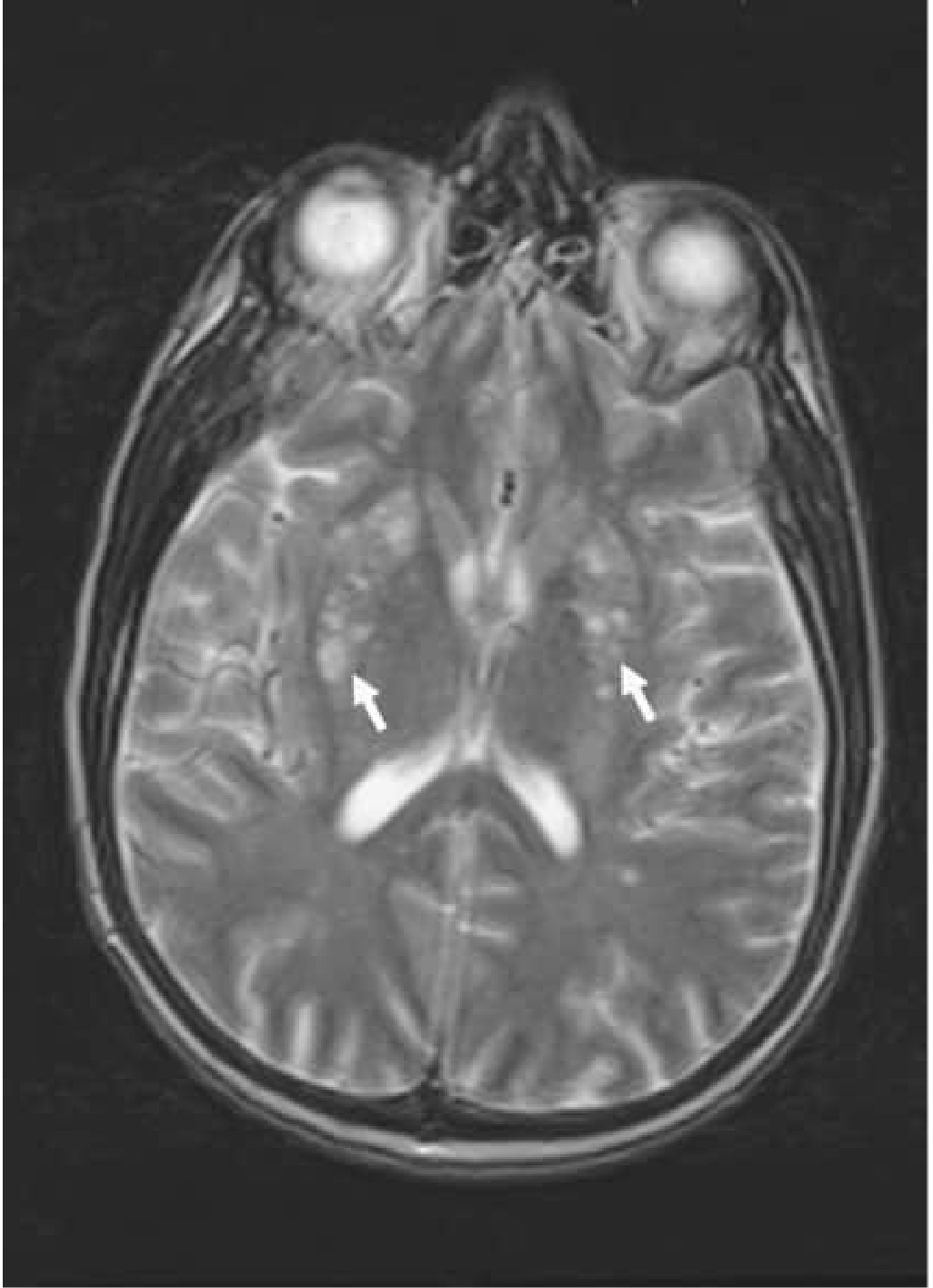
3. Cryptococcal Meningoencephalitis
The most common cause of adult meningitis in AIDS patients, occurring when CD4+ count < 100/μL. Classic triad of headache + fever + stiff neck + photophobia is present here.
- Often presents with subacute onset, personality change, cognitive impairment, elevated ICP
- Meningeal signs may be minimal or absent in >50% of cases
- Complications: hydrocephalus, gelatinous pseudocysts (basal ganglia on T2 MRI — see image), cryptococcoma
- CSF: CrAg (>90% sensitivity), India ink, fungal culture
- Treatment: Induction with amphotericin B (0.5–0.7 mg/kg/day) ± flucytosine (75–150 mg/kg/day) × 2–3 weeks, then fluconazole 200 mg BID × 8–10 weeks, then maintenance 200 mg/day (Bradley & Daroff)
4. CMV Encephalitis
Cytomegalovirus causes severe CNS disease in immunocompromised patients (HIV/AIDS CD4 <50, transplant recipients).
- Features: Subacute encephalitis, myeloradiculopathy (explains incontinence + hyperreflexia progression), ventriculoencephalitis
- Treatment: Ganciclovir/valganciclovir — induction followed by maintenance (Harrison's 22e)
5. Toxoplasma Gondii Encephalitis
Classic ring-enhancing lesions in AIDS (CD4 <100). More focal signs expected (hemiparesis, seizures), but diffuse encephalopathy possible.
6. Progressive Multifocal Leukoencephalopathy (PML)
JC virus reactivation in immunocompromised patients — causes demyelination, cognitive decline, ataxia, slurred speech, weakness. Myoclonic jerks can occur. Subacute course.
7. EBV / HHV-6 Encephalitis
Common in post-transplant patients; HHV-6 in particular causes limbic encephalitis with confusion, seizures, memory disturbance.
🟡 CONSIDER ALSO
8. West Nile Virus Encephalitis
Myoclonic jerks + flaccid paralysis/hyperreflexia + fever + encephalopathy is a characteristic constellation. Predilection for deep gray matter.
- Acute flaccid paralysis from anterior horn involvement
- Diagnosis: WNV IgM in CSF/serum
9. Autoimmune/Paraneoplastic Encephalitis
Anti-NMDA receptor encephalitis and other autoimmune encephalitides can mimic infectious CNS disease.
- Myoclonus, confusion, autonomic instability
- Must be excluded especially if workup is CSF-negative for infection
10. Prion Disease (CJD)
Rapidly progressive dementia + myoclonus + hyperreflexia is the classic triad of Creutzfeldt-Jakob disease. Less likely in acute febrile illness but must be in differential for myoclonus + hyperreflexia.
Immediate Workup
| Test | Target |
|---|---|
| Emergent brain MRI with gadolinium (FLAIR/DWI) | HSV temporal, ring lesions (toxo), PML white matter, WNV deep gray |
| LP with CSF analysis | Cell count, glucose, protein, opening pressure |
| CSF PCR panel | HSV-1/2, CMV, EBV, VZV, HHV-6, JC virus, enterovirus |
| CSF CrAg | Cryptococcus |
| India ink + fungal culture | Cryptococcus |
| Serum CrAg | Cryptococcus (screen) |
| HIV viral load + CD4 count | Defines immune status, guides OI risk |
| Toxoplasma IgG serology | Establishes prior infection risk |
| CMV PCR (blood + CSF) | CMV encephalitis |
| EEG | Seizure activity, CJD pattern (periodic sharp waves) |
| Blood cultures × 2 | Bacterial meningitis/sepsis |
| CBC, CMP, LFTs, ammonia | Metabolic encephalopathy |
| CSF 14-3-3 protein / RT-QuIC | Prion disease if indicated |
Empiric Treatment (Start IMMEDIATELY)
Do not wait for full results if LP is not immediately available.
| Drug | Indication | Dose |
|---|---|---|
| IV Acyclovir | HSV encephalitis (empiric) | 10 mg/kg q8h (30 mg/kg/day) |
| Ampicillin | Listeria (immunocompromised) | 2 g IV q4h |
| Ceftriaxone | Bacterial meningitis | 2 g IV q12h |
| Dexamethasone | Adjunct for bacterial meningitis | 0.15 mg/kg q6h × 4 days (give 15–20 min before or with first antibiotic) |
| Amphotericin B | If CrAg positive / high suspicion Cryptococcus | 0.5–0.7 mg/kg/day |
Note: Dexamethasone should be used cautiously if Cryptococcus is suspected (may worsen fungal disease).
Red Flags in This Case
- Myoclonic jerks + diffuse hyperreflexia: Strongly suggests cortical/subcortical irritation — seen in HSV encephalitis, WNV, CJD, and toxic-metabolic states
- Incontinence: Suggests either frontal lobe involvement (loss of inhibition) or myelopathy (CMV polyradiculomyelitis)
- Immunocompromised status: Dramatically expands the differential and increases urgency — opportunistic infections must be covered empirically
- Somnolence + confusion: Risk of airway compromise — consider ICU-level monitoring
Sources: Harrison's Principles of Internal Medicine 22e (Ch. 197); Bradley & Daroff's Neurology in Clinical Practice (Chs. 17, 77); Goldman-Cecil Medicine (Ch. 309); recent DGHO CNS infection guideline 2024 (PMID context); BMJ Practical Neurology 2026 encephalitis review.
This is a shared conversation. Sign in to Orris to start your own chat.