Can you tell me or show me some granuloma images and, like, types, like caseating, non-caseating, examples of them, like tuberculosis, sarcoidosis? I need to know, uh, about the, like... 哎哟。 Uh, I need to get practiced by seeing the images and finding what type of granuloma it is。 Give me like some practice or examples。
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Loading Image
Loading Image
I now have a rich set of images and textbook content. Let me now compile the complete educational response with all the images.
Granulomas: Types, Images, and Practice Guide
What is a Granuloma?
A granuloma is a compact aggregate of activated macrophages (called epithelioid cells on H&E because of their pink granular cytoplasm) that forms when the immune system tries to wall off something it cannot destroy. The core of epithelioid macrophages is surrounded by a collar of lymphocytes, and older granulomas may have a rim of fibroblasts/connective tissue.
A key feature: multinucleated giant cells (Langhans giant cells) - formed by fusion of multiple activated macrophages, 40-50 μm in diameter with peripheral or horseshoe-shaped nuclei.
The driving mechanism: TH1 cells activate macrophages via IFN-γ, CD40L, and TNF-α. When macrophages can't kill the pathogen, they fuse and wall it off chronically.
The Two Big Categories
| Feature | Caseating (Necrotizing) | Non-caseating (Nonnecrotizing) |
|---|---|---|
| Central necrosis | Yes - cheesy, granular, eosinophilic debris | No - clean epithelioid core |
| Cell outlines in center | Lost (amorphous) | N/A (no necrosis) |
| Prototype disease | Tuberculosis | Sarcoidosis |
| Other examples | Histoplasmosis, coccidioidomycosis | Crohn disease, leprosy, foreign body reaction, drug reactions, berylliosis |
🔬 CASEATING GRANULOMA - Tuberculosis
How TB granuloma forms: Mycobacteria resist macrophage killing → TH1 cells chronically activate macrophages → granuloma (tubercle) forms → center becomes hypoxic + free radical damage → caseous necrosis (looks like cheese grossly; amorphous pink granular debris microscopically).
What to look for on H&E:
- Central pink, amorphous, structureless debris = caseous necrosis (no cell outlines)
- Surrounding epithelioid macrophages
- Langhans giant cells at the periphery (nuclei arranged in horseshoe or peripheral ring)
- Outer rim of lymphocytes and fibroblasts
- Acid-fast bacilli on ZN stain
Image 1: TB Necrotizing Granuloma - H&E (Quick Compendium of Clinical Pathology)
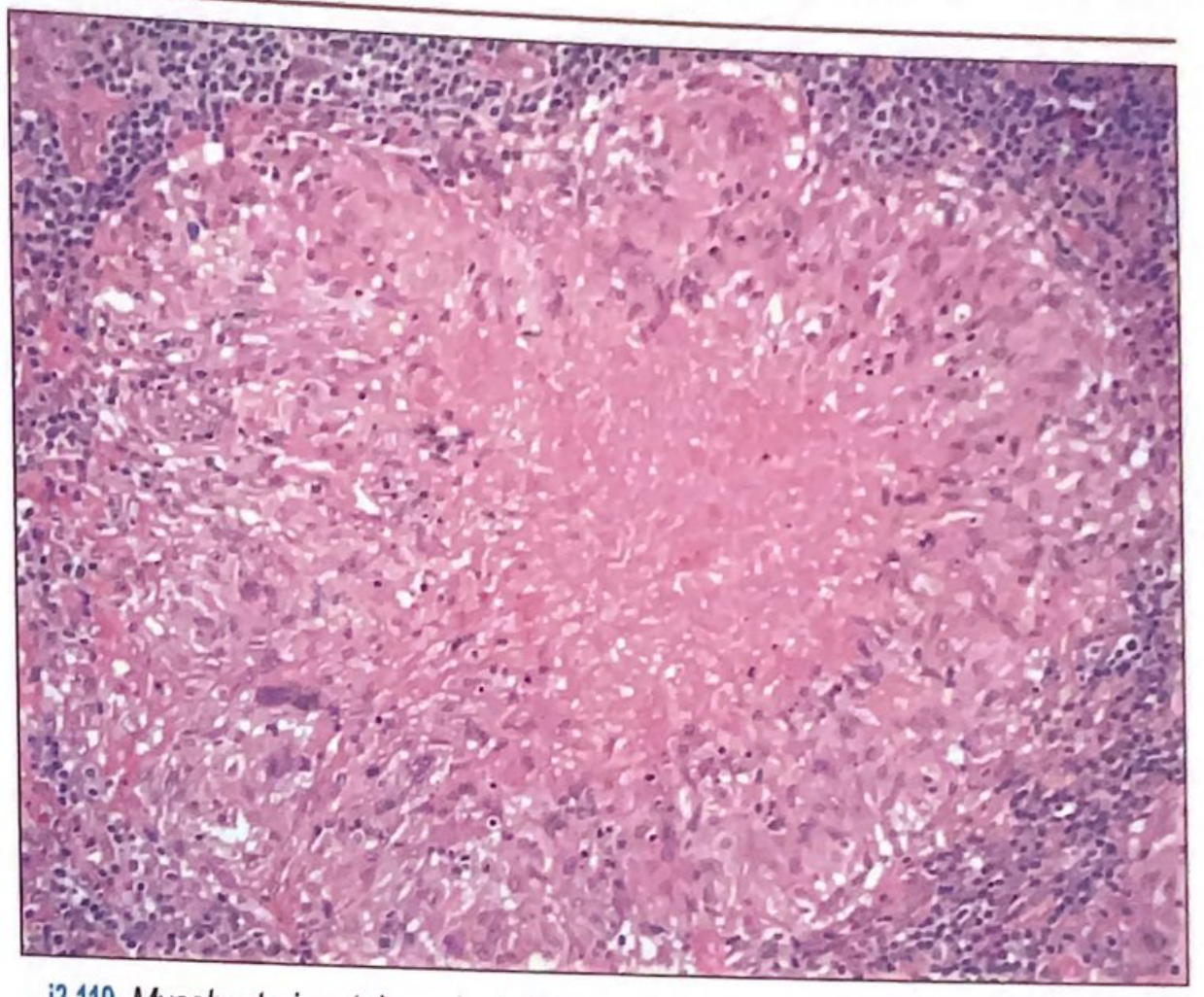
What you're seeing: The large pink central zone is the caseous necrosis - structureless, no cell outlines visible. The dark-staining cells around the periphery are the lymphocytic collar and epithelioid macrophages. This is the hallmark of TB.
Image 2: Granuloma Formation Diagram + Histology (Janeway's Immunobiology)
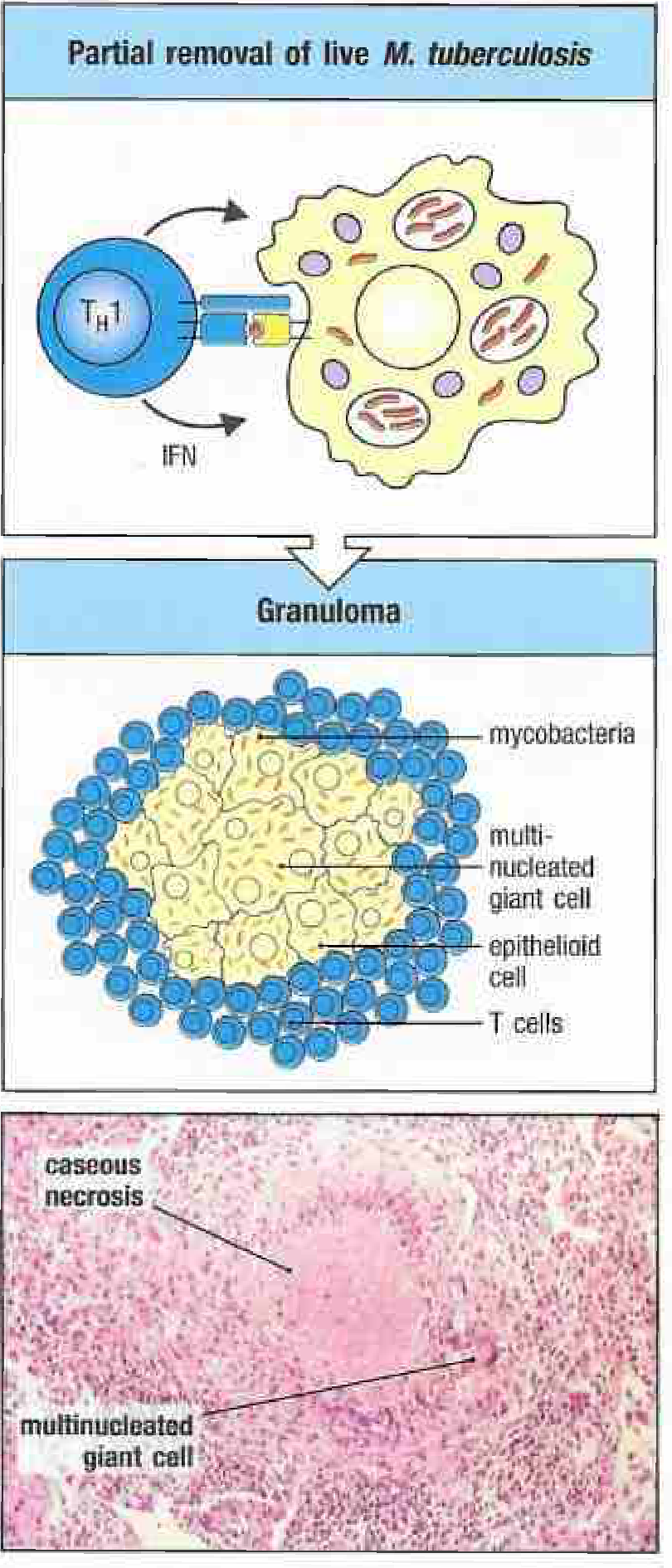
What you're seeing: Top panel shows TH1 cell activating a mycobacterium-infected macrophage via IFN-γ. Middle is the diagram with labels - note the central mycobacteria, surrounding epithelioid cells, multinucleated giant cells, and outer T cells. Bottom panel is the actual H&E - notice the labeled "caseous necrosis" center (pale, structureless) and the "multinucleated giant cell" at the edge.
Image 3: Tuberculous Granuloma - Robbins (Robbins & Cotran Pathologic Basis of Disease)
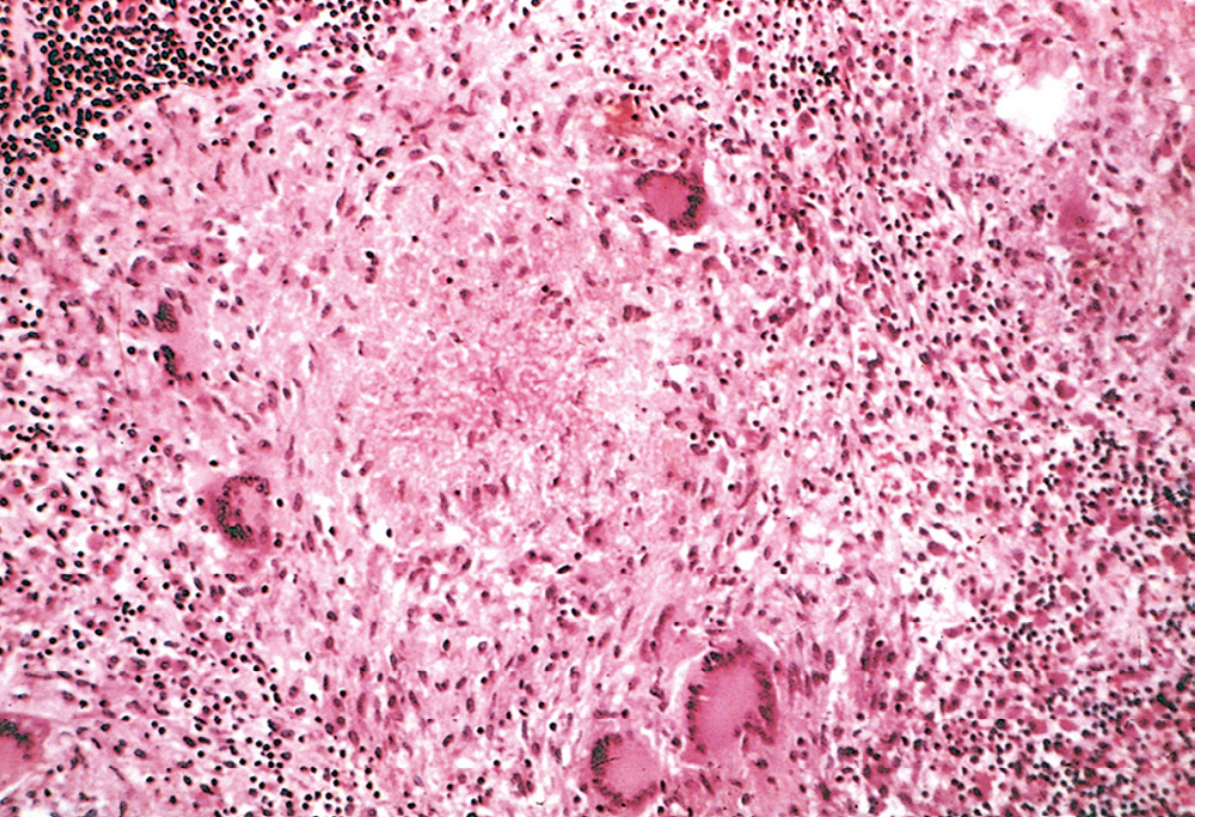
What you're seeing: Classic Robbins image. The pale amorphous center = caseous necrosis. Around it: large epithelioid macrophages with abundant pink cytoplasm and indistinct cell borders. You can spot the large multinucleated giant cells (big cells, multiple dark nuclei). Outer rim of small dark lymphocytes.
Robbins & Cotran Pathologic Basis of Disease describes this as: "Caseating granulomas (tubercles): foci of activated macrophages (epithelioid cells), rimmed by fibroblasts, lymphocytes, histiocytes, occasional Langhans giant cells; central necrosis with amorphous granular debris; acid-fast bacilli."
🔬 NON-CASEATING GRANULOMA - Sarcoidosis
Sarcoidosis key facts:
- Unknown etiology (no infectious cause found)
- Diagnosis requires: clinical + imaging + histology showing non-caseating granulomas + exclusion of other causes
- Serum ACE elevated in ~85% of active disease
- Bilateral hilar lymphadenopathy on CXR is classic
What to look for on H&E:
- Tight, well-defined clusters of epithelioid macrophages
- NO central necrosis - the center is full of pink epithelioid cells, not debris
- Multinucleated giant cells often present (may contain Schaumann bodies or asteroid bodies)
- Thin rim of lymphocytes
- "Naked granuloma" appearance - less lymphocytic cuffing than TB
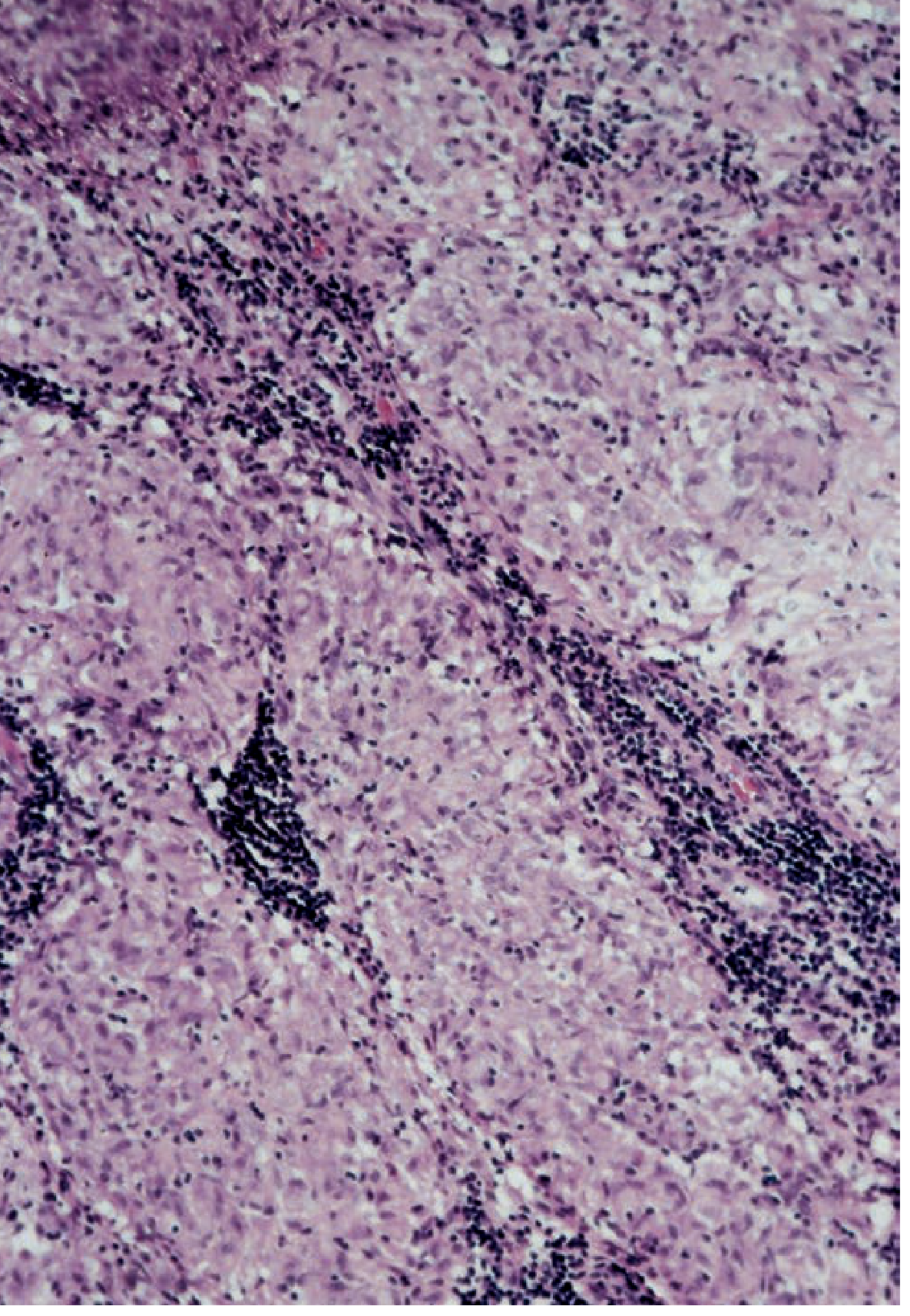
Image 4: Sarcoidosis - Lung Biopsy (Fishman's Pulmonary Diseases)
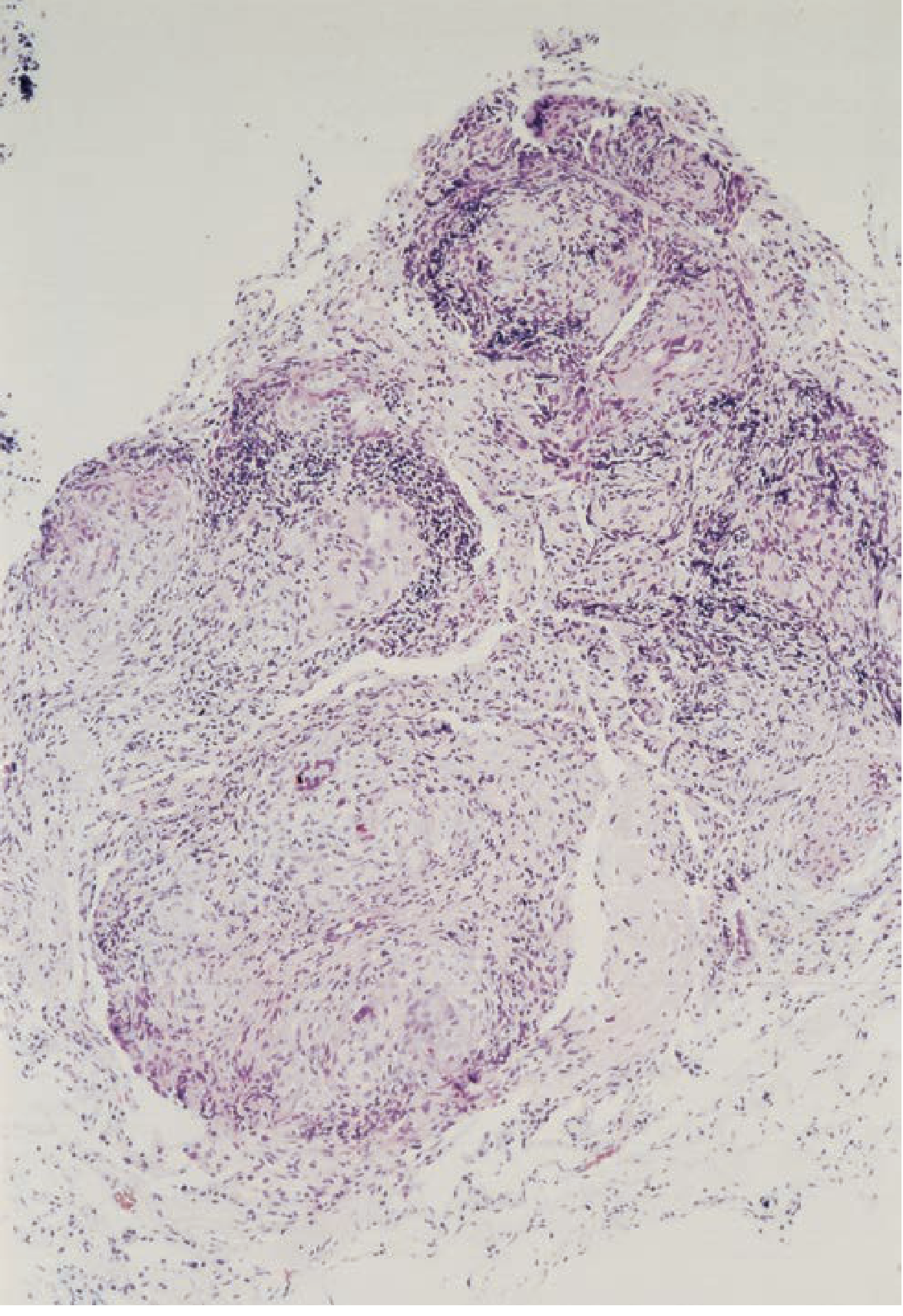
What you're seeing (x80): Multiple discrete granuloma nodules in the lung parenchyma. Notice there is NO pale cheesy center - the clusters are solid, cellular, pink-purple all the way through. This is the key difference from TB. Multiple coalescing granulomas fill the tissue.
Image 5: Sarcoidosis - Mediastinal Lymph Node Biopsy (Fishman's Pulmonary Diseases)
What you're seeing (x200): Higher power view. You can see the discrete collections of epithelioid cells (large, pale-pink, indistinct borders) forming nodules. Again, no central necrosis. The dark areas between granulomas are the lymphocytic background of the lymph node.
Practice Quiz - Can You Identify These?
Here's a quick self-test based on what you've seen:
Question 1: You see a biopsy with a tight cluster of pink macrophages, NO central necrosis, multinucleated giant cells with Schaumann bodies, from a patient with bilateral hilar lymphadenopathy and elevated ACE. → Answer: Non-caseating granuloma - Sarcoidosis
Question 2: You see a biopsy with a pale amorphous center (no cell outlines), surrounding epithelioid cells, Langhans giant cells with horseshoe nuclei, from a patient who is immunosuppressed with apical lung infiltrates. → Answer: Caseating granuloma - Tuberculosis
Question 3: Acid-fast bacilli in macrophages, noncaseating granulomas, from lepromatous skin nodules. → Answer: Non-caseating granuloma - Leprosy (M. leprae)
Question 4: Rounded/stellate granuloma with central neutrophils and granular debris, no giant cells, from a patient with regional lymphadenopathy after a cat scratch. → Answer: Cat-scratch disease (Bartonella henselae)
Question 5: Foreign body material visible inside a giant cell with nuclei randomly scattered (not peripheral), no necrosis. → Answer: Foreign body granuloma - non-caseating type, Foreign body giant cells (nuclei scattered throughout vs. Langhans = peripheral)
Diseases With Granulomatous Inflammation - Full Reference Table
(From Robbins & Cotran Pathologic Basis of Disease)
| Disease | Etiology | Type | Key Histology |
|---|---|---|---|
| Tuberculosis | M. tuberculosis | Caseating | Epithelioid cells, Langhans giant cells, central caseous necrosis, acid-fast bacilli |
| Leprosy | M. leprae | Non-caseating | Acid-fast bacilli in macrophages, noncaseating granulomas |
| Syphilis (tertiary) | Treponema pallidum | Gumma | Central necrosis WITH preserved cell outlines (not caseous), plasma cells, histiocyte wall |
| Cat-scratch disease | Bartonella henselae | Non-caseating | Rounded/stellate, central neutrophils + debris, giant cells uncommon |
| Sarcoidosis | Unknown | Non-caseating | Noncaseating granulomas, Schaumann bodies, abundant activated macrophages |
| Crohn disease | Immune-mediated | Non-caseating | Noncaseating granulomas in bowel wall |
| Foreign body reaction | Inert material | Non-caseating | Foreign body giant cells (randomly scattered nuclei), material visible |
| Histoplasmosis | Histoplasma capsulatum | Caseating | Similar to TB; yeast visible within macrophages |
| Berylliosis | Beryllium exposure | Non-caseating | Histologically identical to sarcoidosis, occupational history key |
| Drug reaction | Various drugs | Non-caseating | "Hypersensitivity granulomas," reactive epithelioid histiocytes |
Key Memory Tricks
- Caseating = Cheese (caseous = cheesy). TB makes cheese. Histoplasmosis also caseates.
- Non-caseating = Sarcoid, Crohn, Leprosy, Foreign body, Berylliosis, Drug - think "SCLFBD" - nothing cheesy about them.
- Langhans giant cell = nuclei at the periphery (horseshoe) = infectious/TB type. Foreign body giant cell = nuclei randomly scattered throughout.
- Sarcoid "naked granulomas" = tight, well-formed, minimal lymphocyte cuff, no necrosis. TB granulomas have a thicker lymphocyte/fibroblast rim around them.
- If you see caseating on a biopsy: always rule out TB first before assuming another cause.
Sources: Janeway's Immunobiology 10e, Robbins & Cotran Pathologic Basis of Disease, Fishman's Pulmonary Diseases and Disorders, Quick Compendium of Clinical Pathology 5th ed.
This is a shared conversation. Sign in to Orris to start your own chat.