How to approach a unconscious patient
Reading File
Finding Sources
Finding Sources
Searching the Web
approach to unconscious patient clinical assessment ABCDE
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
I now have comprehensive content from authoritative sources. Here is the full, structured response:
Approach to the Unconscious Patient
Coma is a state of pathologic unresponsiveness from which the patient cannot be aroused by any form of stimulation. The goal is simultaneous stabilization, diagnosis, and treatment - these should not happen sequentially.
Step 1 - Safety & Scene Assessment
Before touching the patient, ensure the scene is safe. Don gloves. Call for help immediately - this is a team effort.
Step 2 - Check for Response (AVPU/GCS)
Quickly determine responsiveness:
- Call the patient's name loudly
- Apply a painful stimulus (trapezius pinch, sternal rub)
- If no response, the patient is unconscious - activate emergency services if not already done
AVPU scale (quick field tool):
| A | Alert |
|---|---|
| V | Responds to Voice |
| P | Responds to Pain |
| U | Unresponsive |
The Glasgow Coma Scale (GCS) is the standard clinical tool (range 3-15):
| Component | Best Response | Score |
|---|---|---|
| Eye Opening | Spontaneous | 4 |
| To voice | 3 | |
| To pain | 2 | |
| None | 1 | |
| Verbal | Oriented | 5 |
| Confused | 4 | |
| Words only | 3 | |
| Sounds | 2 | |
| None | 1 | |
| Motor | Obeys commands | 6 |
| Localizes pain | 5 | |
| Withdrawal | 4 | |
| Flexion (decorticate) | 3 | |
| Extension (decerebrate) | 2 | |
| None | 1 |
GCS ≤8 = coma; necessitates airway protection.
Step 3 - ABCDE Primary Survey
A - Airway
- Is it patent? Look for vomit, secretions, foreign bodies, tongue falling back
- Head-tilt chin-lift (if no C-spine injury) or jaw thrust (if trauma suspected)
- Insert oropharyngeal airway (Guedel) if tolerated (no gag reflex)
- Plan for early intubation if GCS ≤8 or airway at risk
B - Breathing
- Look, listen, feel - is the patient breathing?
- If apneic: start rescue breathing / bag-valve-mask ventilation
- Check SpO2 - give high-flow O2 (15 L/min via non-rebreather mask)
- Assess respiratory pattern - it localizes the lesion:
| Pattern | Significance |
|---|---|
| Cheyne-Stokes | Diencephalic dysfunction, metabolic encephalopathy |
| Central neurogenic hyperventilation | Midbrain/pontine tegmentum lesion |
| Kussmaul (rapid, deep) | Severe metabolic acidosis |
| Ataxic/Biot | Lower brainstem - agonal pattern |
C - Circulation
- Check pulse - if absent, start CPR
- Get IV access (two large-bore IV lines), connect to cardiac monitor
- Check blood pressure and heart rate
- Send bloods immediately (see investigations below)
- Consider hypovolaemia as primary cause of shock until proven otherwise
D - Disability (Neurological)
- GCS (scored above)
- Pupils: size, symmetry, and reactivity to light
| Pupil Finding | Significance |
|---|---|
| Small, reactive (bilateral) | Metabolic, drugs (opioids), high diencephalic |
| Midposition, fixed (bilateral) | Midbrain lesion |
| Pinpoint | Opioids, pontine hemorrhage |
- Eye movements: gaze deviation (towards lesion in hemispheric, away in pontine)
- Oculocephalic reflex (doll's eye): intact = brainstem intact
- Motor responses: decorticate posturing (flexion) vs. decerebrate (extension)
- Blood glucose: bedside glucometry - this is mandatory at this step
E - Exposure
- Fully undress the patient
- Look for: rashes, needle tracks, medic-alert bracelets, trauma, transdermal drug patches, signs of head injury, Battle's sign, raccoon eyes, CSF rhinorrhea/otorrhea
Step 4 - Immediate Investigations
Run simultaneously with ABCDE:
Bedside:
- Blood glucose (always first)
- ECG
- SpO2
Blood tests:
- FBC, U&E, creatinine, LFTs
- Blood glucose, HbA1c
- Serum osmolality
- Coagulation (PT, APTT)
- Blood cultures (if fever)
- ABG (assess oxygenation, ventilation, acid-base)
- Toxicology screen (urine + serum)
- Ammonia, lactate
- Thyroid function, cortisol
Urine: Dipstick + toxicology
Neuroimaging:
- CT head (non-contrast) - first-line to rule out hemorrhage, mass, herniation
- CT angiography or MRI if indicated
LP (lumbar puncture): After CT, if meningitis/encephalitis suspected (fever + neck stiffness)
EEG: If non-convulsive status epilepticus suspected
Step 5 - Targeted History (Collateral)
From witnesses, family, emergency services, medical records:
- Time/onset and circumstances (sudden vs. gradual, trauma, witnessed seizure)
- Past medical history: diabetes, epilepsy, hypertension, heart disease, liver/renal disease, psychiatric history
- Medications: prescribed, OTC, any recent changes
- Drug/alcohol use
- Recent headache, fever, vomiting, neck pain
- Preceding confusion, focal weakness, or visual disturbance
- Atrial fibrillation or prior stroke/TIA
Step 6 - Differential Diagnosis (Causes of Coma)
Use the mnemonic AEIOU TIPS or this structured framework:
Structural / Vascular:
- Traumatic brain injury (contusion, EDH, SDH, SAH, DAI)
- Intracerebral hemorrhage, large hemispheric infarction
- Brainstem/cerebellar stroke
- Raised ICP, herniation
Metabolic / Toxic:
- Hypoglycemia or hyperglycemia (most common reversible cause)
- Hyponatremia, hypernatremia, hypercalcemia
- Hepatic encephalopathy, uremic encephalopathy
- Hypoxia / anoxia (post-cardiac arrest)
- Drug intoxication: opioids, benzodiazepines, barbiturates, alcohol, TCAs, anticholinergics
- Carbon monoxide poisoning
Infectious:
- Bacterial meningitis
- Viral encephalitis (HSV most important)
- Brain abscess
Epileptic:
- Post-ictal state
- Non-convulsive status epilepticus
Endocrine:
- Hypoadrenalism, hypothyroidism (myxoedema coma), pituitary apoplexy
- Hypertensive encephalopathy
Other:
- Locked-in syndrome (mimics coma - patient is aware; communicate via eye blinks)
- Functional/psychogenic unresponsiveness
Step 7 - Empirical Treatment ("Coma Cocktail")
While awaiting results, if no obvious cause is found:
| Drug | Dose | Indication |
|---|---|---|
| 50% Dextrose | 25 g IV | Hypoglycemia |
| Thiamine (B1) | 100 mg IV | Before glucose, to prevent Wernicke's |
| Naloxone | 0.4-2 mg IV | Opioid overdose |
| Flumazenil | 0.2 mg IV | Benzodiazepine overdose (caution: seizure risk) |
If fever + neck stiffness: start empirical antibiotics + aciclovir for bacterial meningitis/HSV encephalitis before LP results.
Step 8 - Raised ICP Management
If raised ICP is suspected (papilloedema, Cushing's triad: hypertension + bradycardia + irregular breathing):
- Head elevation 30 degrees
- Hyperventilation to PaCO2 ~30 mmHg (transient effect)
- Mannitol 0.5-1.5 g/kg IV or hypertonic saline
- Dexamethasone (for vasogenic oedema around tumour or abscess; not for trauma or ischaemia)
- Neurosurgery referral for mass lesion, hydrocephalus, or refractory ICP
Step 9 - Ongoing Monitoring & Documentation
- Continuous monitoring: SpO2, ECG, BP, temperature, urine output
- Hourly GCS documentation
- Reassess pupils and neurological status regularly
- Call for senior/specialist review early (neurology, ICU, neurosurgery as needed)
- Prevent secondary brain injury: maintain normoglycaemia, normothermia, MAP >70 mmHg, SpO2 >94%
Key Neurological Localisation Summary
| Level of Dysfunction | Pupils | Motor Response | Breathing |
|---|---|---|---|
| High diencephalic | Small, reactive | Paratonia, grasp | Eupnea / post-hyperventilation apnea |
| Low diencephalic | Small, reactive | Decorticate (flexion) | Cheyne-Stokes |
| Midbrain | Midposition, fixed | Decerebrate (extension) | Central neurogenic hyperventilation |
| Pontine | Pinpoint | Flaccid / minimal | Apneustic |
| Medullary | Variable | Flaccid | Ataxic / agonal |
Sources: Goldman-Cecil Medicine, 26th Ed. (Greer & Bernat, Ch. 373) | Bradley and Daroff's Neurology in Clinical Practice | Resuscitation Council UK - ABCDE Approach
What are factors that affect pulmonary circulation. Give answer from Morgan book
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I now have everything needed for a complete, well-structured answer directly from Morgan & Mikhail. Here it is:
Factors Affecting Pulmonary Circulation
Source: Morgan and Mikhail's Clinical Anesthesiology, 7th Edition
Overview
The pulmonary circulation normally receives the total output of the right heart via the pulmonary artery. Pulmonary arteries and veins have thinner walls with less smooth muscle than systemic vessels. Despite equal flow through both circulations, pulmonary vascular resistance (PVR) is much lower, resulting in far lower pulmonary pressures.
Of the ~5 L/min flowing through the lungs, only 70-100 mL at any one time is within the pulmonary capillaries undergoing gas exchange.
1. Pulmonary Blood Volume
Total pulmonary blood volume can vary between 500 and 1000 mL. Several factors shift this:
| Factor | Effect on Pulmonary Blood Volume |
|---|---|
| Cardiac systole | Small increase |
| Spontaneous inspiration | Small increase |
| Supine to erect posture | Decreases by up to 27% |
| Trendelenburg position | Increases |
| Systemic venoconstriction | Shifts blood from systemic to pulmonary |
| Systemic vasodilation | Shifts blood from pulmonary to systemic |
Large increases in cardiac output or blood volume are tolerated with little change in pressure due to passive dilation of open vessels and recruitment of collapsed pulmonary vessels. In this way, the lung acts as a reservoir for the systemic circulation.
2. Local Chemical & Gaseous Factors
Local factors are more important than the autonomic nervous system in influencing pulmonary vascular tone.
Hypoxia (Most Important)
- Hypoxia is a powerful stimulus for pulmonary vasoconstriction - the opposite of its effect on systemic vessels
- Both pulmonary arterial (mixed venous) hypoxia and alveolar hypoxia cause vasoconstriction, but alveolar hypoxia is the more powerful stimulus
- Mechanisms:
- Direct effect of hypoxia on pulmonary vasculature
- Increased production of leukotrienes relative to vasodilatory prostaglandins
- Inhibition of nitric oxide production
- Hypoxic pulmonary vasoconstriction (HPV) is a key physiological mechanism to reduce intrapulmonary shunting and prevent hypoxemia
- Hyperoxia has little effect on the pulmonary circulation in normal individuals
CO2 and Acid-Base
| Condition | Effect on Pulmonary Circulation |
|---|---|
| Hypercapnia | Vasoconstriction |
| Acidosis | Vasoconstriction |
| Hypocapnia | Vasodilation |
Note: These effects are the opposite of what occurs in the systemic circulation.
3. Gravity and Posture (Distribution of Pulmonary Perfusion)
Pulmonary blood flow is not uniform. Dependent areas receive greater blood flow than non-dependent areas due to a gravitational gradient of 1 cmH₂O per cm of lung height.
The normally low pulmonary pressures allow gravity to exert a significant influence on flow. Additionally, in vivo perfusion scanning shows an "onion-like" layering with reduced flow at the periphery and increased flow toward the hilum.
West Zones of Pulmonary Blood Flow
The interplay between pulmonary arterial pressure (Pa), alveolar pressure (PA), and pulmonary venous pressure (Pv) defines four distinct zones:
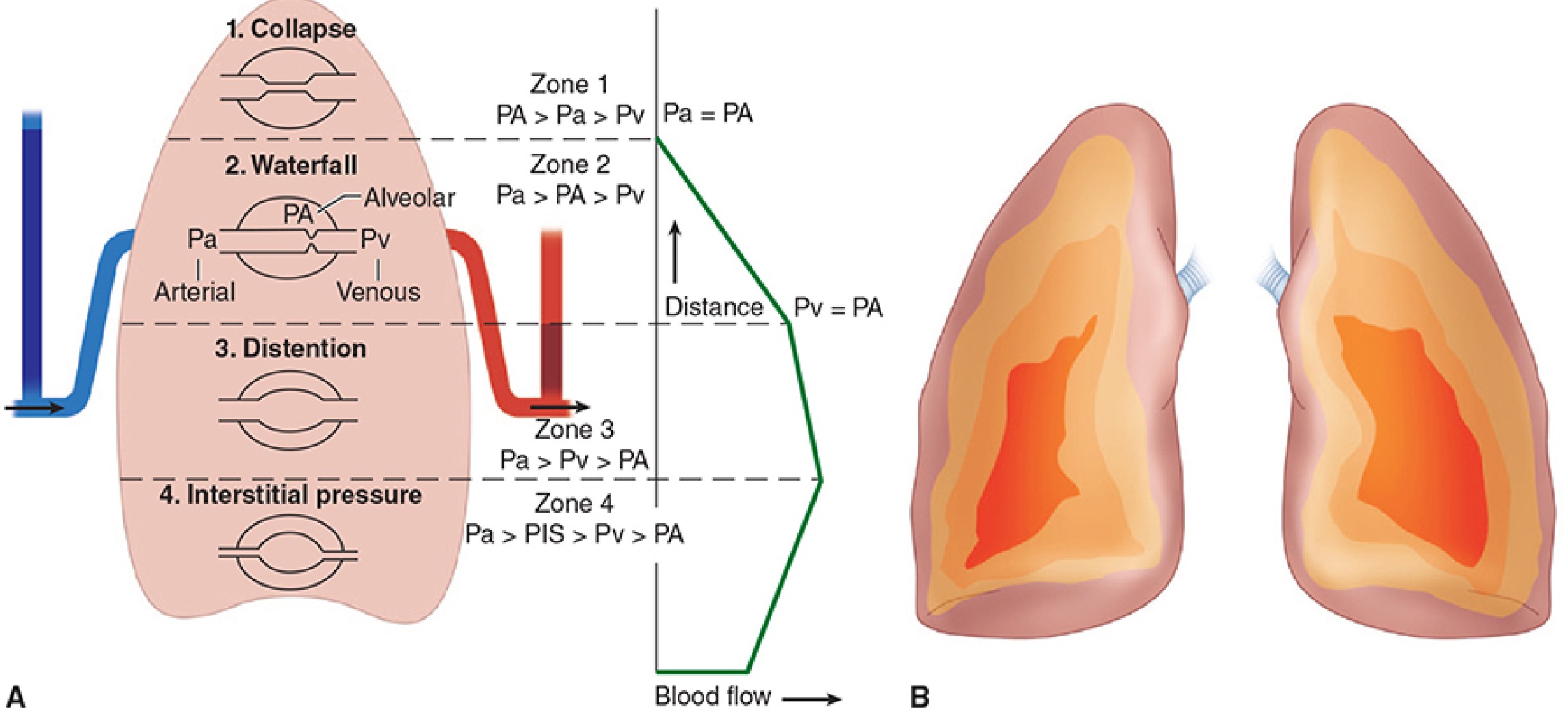
| Zone | Pressure Relationship | Blood Flow | Mechanism |
|---|---|---|---|
| Zone 1 (apex) | PA > Pa > Pv | None / Dead space | Alveolar pressure exceeds arterial pressure; capillaries collapse |
| Zone 2 (middle) | Pa > PA > Pv | Depends on Pa - PA | "Waterfall" effect; flow determined by arterial-alveolar pressure difference |
| Zone 3 (base) | Pa > Pv > PA | Continuous; highest | Both Pa and Pv exceed PA; flow determined by arterio-venous difference |
| Zone 4 (dependent base) | Pa > PIS > Pv > PA | Reduced | High interstitial pressure (PIS) compresses extra-alveolar vessels |
Clinical notes:
- Zone 1 is normally small in spontaneous breathing but enlarges during positive pressure ventilation (raises PA)
- Zone 4 is most prominent at low lung volumes when interstitial pressure is highest
4. Ventilation/Perfusion (V/Q) Ratio Effects
- Overall V/Q ratio = ~0.8 (ventilation 4 L/min; perfusion 5 L/min)
- Because perfusion increases at a greater rate than ventilation in dependent areas:
- Apical (non-dependent) areas: high V/Q (relative dead space)
- Basal (dependent) areas: low V/Q (relative shunt)
- Units with low V/Q ratios have low O2 tension and high CO2 tension in their effluent - this depresses arterial PaO2 significantly more than it elevates PaCO2
5. Cardiac Output & Intravascular Pressures
Pulmonary blood flow is directly dependent on right ventricular output. Increased cardiac output recruits collapsed vessels and distends patent ones - both mechanisms reduce PVR, keeping pulmonary pressures relatively stable even with high flows.
6. Lung Volume
Pulmonary vascular resistance is affected by lung volume through two competing vessel types:
| Vessel Type | Effect of Lung Volume |
|---|---|
| Alveolar vessels (in alveolar walls) | Compressed at high lung volumes → increased resistance |
| Extra-alveolar vessels (in lung parenchyma) | Compressed at low lung volumes (Zone 4) → increased resistance |
PVR is therefore lowest at functional residual capacity (FRC) and increases at both high and low lung volumes.
Summary Table
| Factor | Effect |
|---|---|
| Hypoxia | Vasoconstriction (HPV) |
| Hypercapnia / acidosis | Vasoconstriction |
| Hypocapnia | Vasodilation |
| Gravity / dependent position | Increased perfusion |
| Positive pressure ventilation | Enlarges Zone 1 (dead space) |
| Systemic venoconstriction | Increases pulmonary blood volume |
| High lung volumes | Compress alveolar vessels, increase PVR |
| Low lung volumes | Compress extra-alveolar vessels, increase PVR |
| Increased cardiac output | Vessel recruitment/distension, reduces PVR |
Morgan and Mikhail's Clinical Anesthesiology, 7th Ed. - Chapter 23 (Pulmonary Physiology), pp. 942-945
This is a shared conversation. Sign in to Orris to start your own chat.