
91f560c4-8241-4d97-9d19-210d0fc721a9.jpeg
Explain this
analyse_media
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
These are notes on the Etiopathology of Neonatal Respiratory Distress Syndrome (RDS) / Hyaline Membrane Disease. Here is a full breakdown of everything on the page.
What Is This Condition?
Neonatal Respiratory Distress Syndrome (RDS), also called Hyaline Membrane Disease (HMD), is the most common cause of respiratory failure in newborns. The core problem is a deficiency of surfactant - the substance that keeps alveoli (air sacs in the lungs) from collapsing after each breath.
Section 1: Etiopathology (Top Flowchart) - The Vicious Cycle
This is the key diagram showing how surfactant deficiency creates a self-worsening (vicious) cycle:
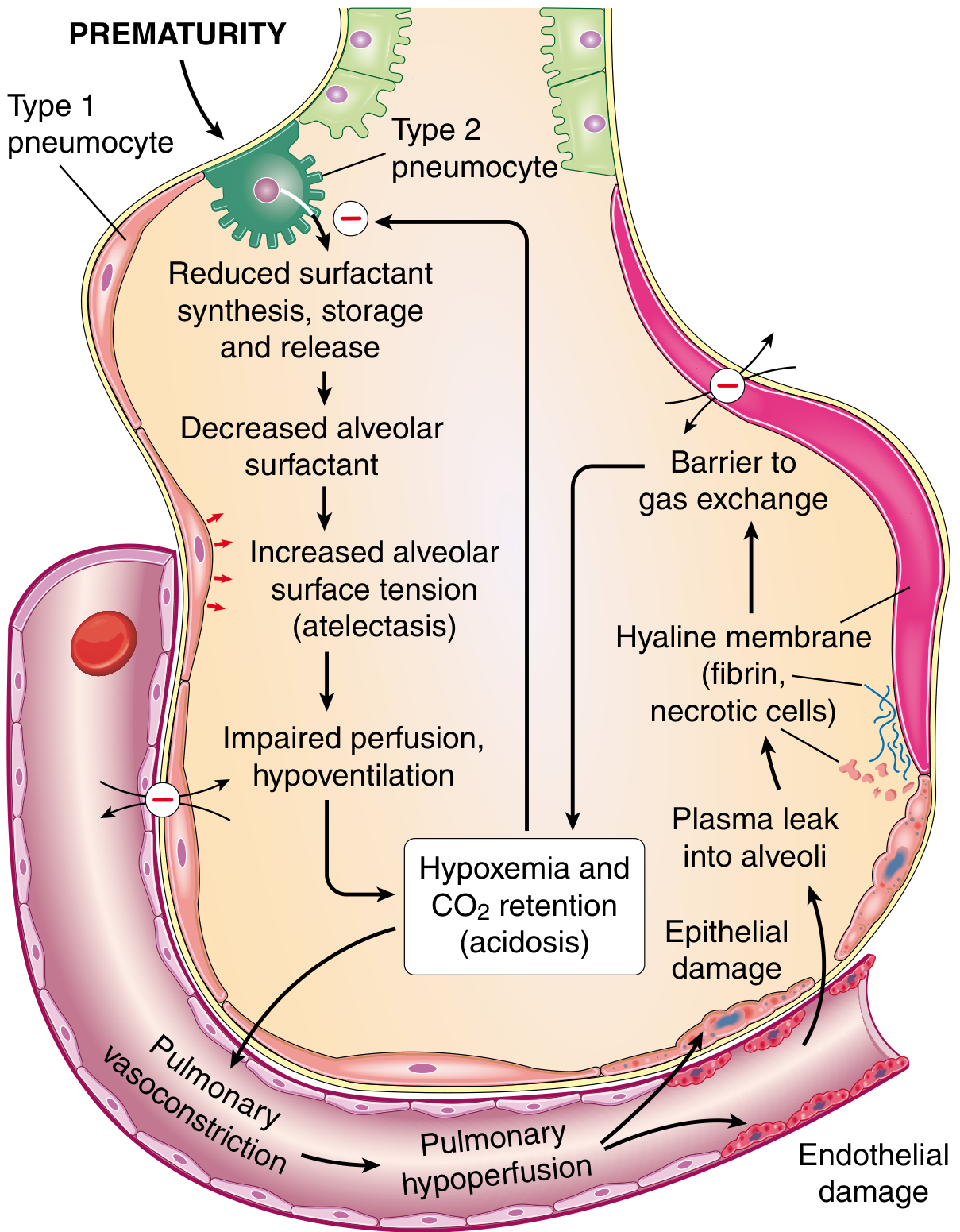
Here is the step-by-step cycle from your notes:
-
Diminished Surfactant
- Surfactant is produced by Type II pneumocytes. Without enough surfactant, alveolar surface tension increases.
- Result: Progressive atelectasis (widespread alveolar collapse)
-
Progressive Atelectasis → Hyperventilation
- The baby tries to compensate by breathing faster and harder. This quickly exhausts the infant.
-
Hyperventilation → ↑PCO₂, ↓PO₂, ↓pH
- Gas exchange fails. CO₂ builds up (hypercapnia), oxygen drops (hypoxia), and blood becomes acidic (respiratory acidosis).
-
Acidosis & Hypoxia → Impaired cellular metabolism
- The acid environment and low oxygen directly impair the Type II pneumocytes that make surfactant - worsening the original deficiency. This is the vicious cycle closing back on itself.
-
↑PCO₂, ↓PO₂, ↓pH → Pulmonary vasoconstriction + Hypotension/Shock
- Hypoxia causes the pulmonary blood vessels to constrict reflexively (hypoxic pulmonary vasoconstriction).
- This leads to alveolar hypoperfusion (poor blood flow to alveoli).
-
Alveolar Hypoperfusion → Impaired cellular metabolism → Less surfactant
- The loop is complete. Less blood flow = less metabolic support for surfactant-producing cells = even less surfactant.
Section 2: Causes (Hub-and-Spoke Diagram)
Five causes of diminished surfactant are listed:
| Cause | Explanation |
|---|---|
| Prematurity | The most important cause. Surfactant production only accelerates after 35 weeks of gestation. Premature infants have underdeveloped Type II pneumocytes. |
| C-section (Cesarean section) | Normal labor stimulates surfactant synthesis; C-section before labor onset bypasses this stimulus. |
| Acidosis | Low pH directly inhibits surfactant production. |
| Intra-partum asphyxia | Oxygen deprivation during delivery damages Type II pneumocytes. |
| Familial predisposition | Genetic mutations in surfactant protein genes (e.g., SFTPB, SFTPC) can cause congenital surfactant deficiency. |
Section 3: Clinical Consequences (Lower Diagram)
The box shows ↑PCO₂, ↓PO₂, ↓pH (the blood gas picture of RDS), and the diagram maps the clinical states that contribute to or result from it:
| Finding | Meaning |
|---|---|
| Apnea | Breathing pauses; the exhausted infant stops making respiratory effort. |
| Hypothermia | Metabolic failure and poor perfusion lead to inability to maintain body temperature. |
| Hypercapnia (↑CO₂ in blood) | Carbon dioxide cannot be exhaled due to collapsed alveoli. |
| Asphyxia neonatorum | Combined hypoxia and hypercapnia causing systemic suffocation. |
| Transient tachypnea of the newborn (TTN) | Rapid breathing, sometimes seen as an overlapping or preceding condition. |
Section 4: Final Paragraph - How the Hyaline Membrane Forms
"Progressive epithelial and endothelial cell injury due to atelectasis. Ischemic injury results in effusion of proteinous fluid into alveolar space, forming membrane leading to condition i.e. Hyaline Membrane Disease."
This is the microscopic mechanism:
- Atelectasis causes ischemic injury to the alveolar epithelium (Type I & II pneumocytes) and the capillary endothelium.
- This damage lets protein-rich fluid (plasma) leak into the alveolar spaces.
- The proteins, mainly fibrin mixed with necrotic cell debris, coat the alveolar walls as a glassy, eosinophilic layer - the hyaline membrane (hyaline = glass-like in Greek).
- These membranes further block gas exchange, deepening hypoxia and completing the destructive cycle.
Summary in One Sentence
Surfactant deficiency (mainly from prematurity) causes progressive alveolar collapse → hypoxia and acidosis → pulmonary vasoconstriction and cellular damage → even less surfactant → hyaline membrane formation from leaked plasma proteins → a life-threatening vicious cycle. - Robbins & Kumar Basic Pathology, p. 137; Robbins Pathologic Basis of Disease, p. 433
This is a shared conversation. Sign in to Orris to start your own chat.