40 years male working at a construction site on investigation showed Lung nodularity in chest X-ray. This condition belongs to which group of lung disease? What is the morphology?
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a thorough answer. Here it is:
Clinical Diagnosis: Silicosis
A 40-year-old male construction worker with lung nodularity on chest X-ray fits the classic presentation of silicosis - inhalation of crystalline silicon dioxide (silica) dust from concrete cutting, sandblasting, and demolition work.
Disease Group: Pneumoconiosis
Pneumoconiosis is the group this condition belongs to. It is defined as lung disease caused by inhalation of mineral dusts, chemical fumes, or vapors encountered in the workplace. Silicosis is classified under the mineral dust pneumoconioses, alongside coal workers' pneumoconiosis and asbestosis.
The key factors that determine the severity of pneumoconiosis include:
- Dust concentration in ambient air
- Duration of exposure
- Particle size - the most dangerous particles are 1 to 5 µm in diameter, as they reach terminal airways and air sacs
- Solubility of the particle (more soluble = more toxic acutely)
- Particle shape (irregular/jagged particles are more harmful)
(Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 647)
Pathogenesis
Phagocytosis of inhaled silica crystals by macrophages activates the inflammasome, triggering release of IL-1 and IL-18. This recruits additional inflammatory cells and activates interstitial fibroblasts, leading to progressive collagen deposition and fibrosis. Crystalline silica forms (quartz, cristobalite, tridymite) are far more fibrogenic than amorphous forms - quartz is the most commonly implicated.
Morphology of Silicosis
Gross Pathology
- Early stage: Tiny, barely palpable, discrete pale to blackened nodules in the hilar lymph nodes and upper zones of the lungs
- Progressive stage: Nodules coalesce into hard, collagenous scars
- Advanced disease (Progressive Massive Fibrosis - PMF): Large confluent masses, typically in the posterior upper lobes, with architectural distortion and traction emphysema at the periphery
- Eggshell calcification in hilar lymph nodes - a pathognomonic radiological sign (calcium rimming a lucent center)
- Some nodules may undergo central softening/cavitation due to superimposed tuberculosis or ischemia
Histopathology (Hallmark Lesion)
The diagnostic lesion of silicosis is the silicotic nodule, which has two distinct zones:
- Central zone: Whorled (concentric layers of) collagen fibers - the defining feature
- Peripheral zone: Dust-laden macrophages surrounding the collagen core
Under polarized microscopy, weakly birefringent silicate particles are visible within the nodules.
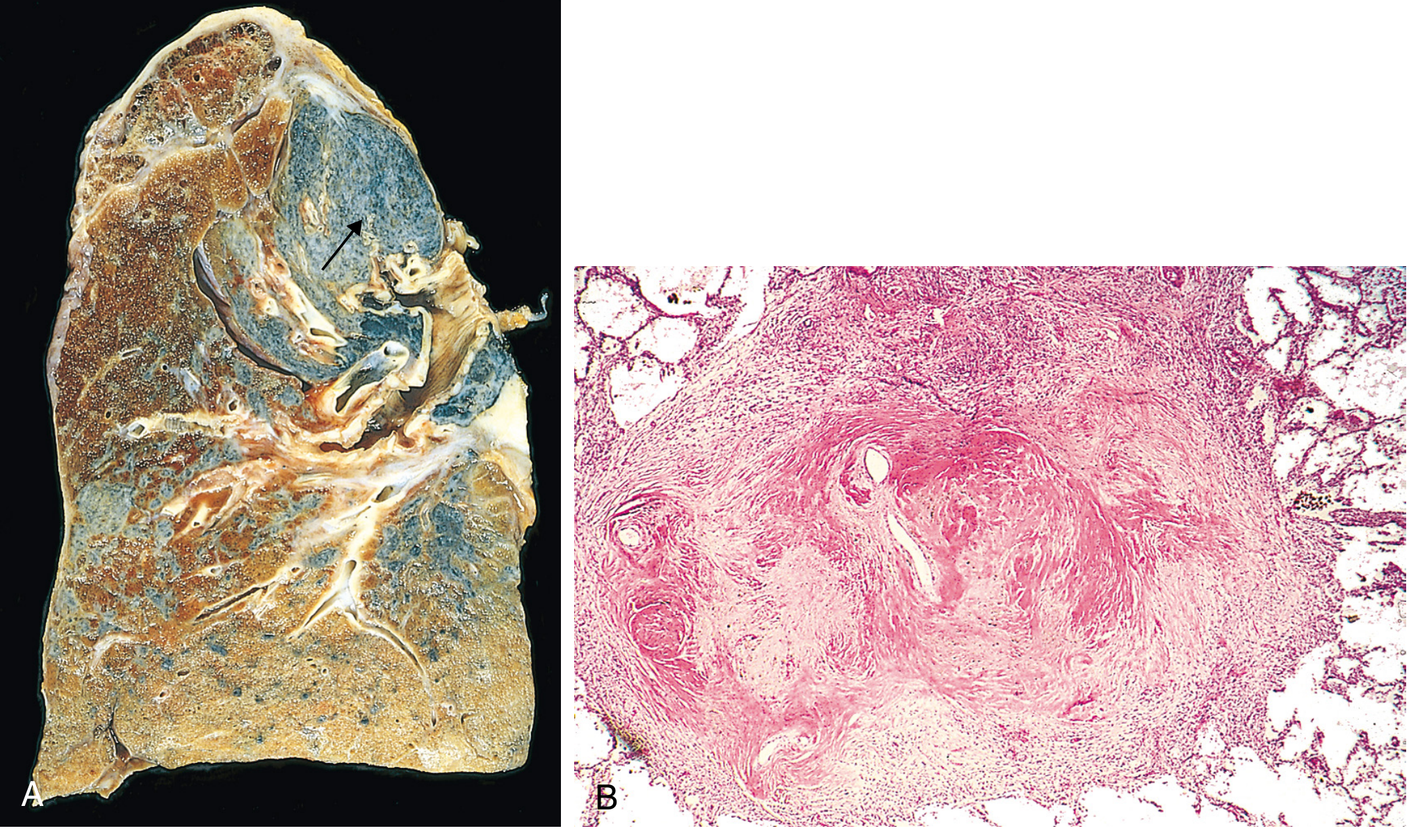
Fig. 15.17 Advanced silicosis. (A) Scarring has contracted the upper lobe into a small dark mass. Note the dense pleural thickening. (B) A silicotic nodule showing the classic whorled pattern of collagen fibers. - Robbins, Cotran & Kumar Pathologic Basis of Disease
Chest X-Ray Findings (Correlation)
- Simple silicosis: Profusion of small (1-3 mm) round nodules predominantly in the upper two-thirds of the lung, posterior predominance
- Nodules may be calcified
- Hilar and mediastinal lymph node enlargement with eggshell calcification
- PMF: Mass-like opacities in the posterior upper lobes with hilar elevation and peripheral emphysema
(Grainger & Allison's Diagnostic Radiology, p. 245)
Summary Table
| Feature | Detail |
|---|---|
| Disease group | Pneumoconiosis (mineral dust type) |
| Causative agent | Crystalline silica (SiO2) - quartz |
| Occupation at risk | Construction, sandblasting, stone cutting, mining |
| Key gross finding | Hard collagenous nodules, upper lobe predominance |
| Key histological finding | Whorled collagen nodule with peripheral macrophages |
| Polarized microscopy | Weakly birefringent silicate particles |
| Radiological sign | Eggshell calcification of hilar nodes |
| Complications | PMF, tuberculosis (2-4x risk), lung cancer (2x risk) |
(Robbins, Cotran & Kumar Pathologic Basis of Disease, pp. 647-649)
50 years old male presents with cough, dyspnea, intermittent hemoptysis for two months along with loss of weight and appetite. He is a chronic smoker for the past three decades. CT chest revealed mass lesion in the right lobe of lung. What is your probable diagnosis? Discuss in detail the classification, morphological features and the paraneoplastic syndromes associated with it
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive data from multiple authoritative textbooks. Let me compile the complete answer.
Probable Diagnosis: Primary Bronchogenic Carcinoma (Lung Cancer)
A 50-year-old male with a 30-pack-year smoking history, presenting with a 2-month history of:
- Productive cough
- Dyspnea
- Intermittent hemoptysis (highly suggestive of endobronchial involvement)
- Constitutional symptoms - weight loss and anorexia (B symptoms)
- CT chest mass lesion in the right lobe
This is the classic triad of a centrally located bronchogenic carcinoma, most likely squamous cell carcinoma (central, cavitating, strongly linked to heavy smoking in a male patient).
Classification of Lung Carcinoma
WHO / Histologic Classification (2021)
The two major divisions are:
1. Non-Small Cell Lung Carcinoma (NSCLC) - ~84% of all lung cancers
| Subtype | Frequency | Key Features |
|---|---|---|
| Adenocarcinoma | Most common overall (~40%) | Peripheral, women/nonsmokers, EGFR/KRAS/ALK mutations |
| Squamous Cell Carcinoma | ~25-30% | Central/hilar, heavy smokers, cavitation, men |
| Large Cell Carcinoma | ~10-15% | Peripheral, undifferentiated, diagnosis of exclusion |
2. Small Cell Lung Carcinoma (SCLC) - ~13-15%
- Highly aggressive neuroendocrine tumor
- Almost exclusively in smokers
- Virtually always metastatic at presentation
- Sensitive to chemo/radiation but invariably recurs
3. Neuroendocrine Tumors (NETs) - ~1-2%
- Typical carcinoid (low grade)
- Atypical carcinoid (intermediate grade)
- Large cell neuroendocrine carcinoma (high grade)
(Robbins & Kumar Basic Pathology, p. 497; Murray & Nadel's Textbook of Respiratory Medicine)
Morphological Features
A. Squamous Cell Carcinoma (Most likely in this patient)
Gross:
- Arises from the central bronchi (main/lobar/segmental)
- Appears as a gray-white, irregular, hilar mass that may obstruct the bronchial lumen
- Frequently shows central cavitation due to necrosis (since squamous cells are prone to ischemia)
- Associated with surrounding pneumonitis/obstructive pneumonia distally
- May show pleural involvement and direct chest wall invasion
Histology:
- Arises from squamous metaplasia -> squamous dysplasia -> carcinoma in situ -> invasive carcinoma
- Well-differentiated: Sheets and nests of polygonal cells with abundant pink cytoplasm, intercellular bridges (desmosomes), and keratin pearls (whorls of squamous cells with central keratinization)
- Moderately differentiated: Some keratinization without well-formed pearls
- Poorly differentiated: Individual cell keratinization only, prominent pleomorphism
- IHC markers: CK5/6+, p40+, p63+ (nuclear), TTF-1 negative
B. Adenocarcinoma
Gross:
- Most often peripheral, frequently subpleural
- Grayish-white, lobulated, may show pleural puckering (retraction)
- Less likely to cavitate than squamous cell carcinoma
- Can arise from atypical adenomatous hyperplasia (AAH) -> adenocarcinoma in situ -> minimally invasive -> invasive
Histology (2021 WHO Growth Patterns):
- Lepidic: Tumor cells grow along pre-existing alveolar walls without destroying architecture (best prognosis)
- Acinar: Gland-forming pattern with round to oval malignant glands
- Papillary: Tumor cells on fibrovascular cores
- Micropapillary: Tumor cells in small papillary tufts without fibrovascular cores
- Solid: Sheets of cells with intracellular mucin (worst prognosis)
- IHC markers: TTF-1+, Napsin A+, CK7+; mucin positive
C. Small Cell Carcinoma (Oat Cell Carcinoma)
Gross:
- Central/perihilar soft, friable, white-gray masses
- Extensive mediastinal and hilar lymph node involvement early
- Widely metastatic at presentation
Histology (the hallmark features):
- Small cells (slightly larger than lymphocytes) with:
- Scant cytoplasm
- Hyperchromatic, "salt-and-pepper" nuclei (fine chromatin - neuroendocrine pattern)
- Indistinct nucleoli
- High mitotic rate
- Azzopardi effect: DNA encrustation of blood vessel walls (due to rapid cell death)
- Crush artifact on biopsy specimens
- Diffuse sheets of cells, no gland formation, no squamous differentiation
- IHC markers: Synaptophysin+, Chromogranin+, CD56+, TTF-1+ (~90%), CK (dot-like), RB negative
(Robbins & Kumar Basic Pathology, Table 11.6, p. 488)
D. Large Cell Carcinoma
Gross: Large peripheral mass, often with necrosis and hemorrhage
Histology:
- Sheets of large, pleomorphic cells with prominent nucleoli
- No squamous, glandular, or neuroendocrine differentiation
- Diagnosis of exclusion after IHC panel is negative
- Poor prognosis
Paraneoplastic Syndromes
Paraneoplastic syndromes occur in about 10% of cancer patients and may be the earliest manifestation of an occult tumor. They cannot be explained by direct invasion or metastasis. They are critical to recognize because they may confound treatment planning or mimic metastatic disease.
(Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 311)
I. Endocrinopathies (Ectopic Hormone Production)
| Syndrome | Tumor Type | Mechanism |
|---|---|---|
| Cushing Syndrome | SCLC (#1 cause - ~50% of ectopic Cushing) | Ectopic ACTH / pro-opiomelanocortin (POMC) secretion |
| SIADH (hyponatremia) | SCLC | Ectopic ADH (vasopressin) secretion |
| Hypercalcemia | Squamous cell carcinoma (#1 association) | Parathyroid hormone-related protein (PTHrP) secretion; also TGF-α, TNF, IL-1 |
| Carcinoid Syndrome | Pulmonary carcinoid | Serotonin, VIP |
| Acromegaly | Various lung tumors | Ectopic growth hormone |
| Gynecomastia | SCLC, large cell carcinoma | Ectopic gonadotropins/prolactin |
| Hypoglycemia | Rare lung tumors | Insulin-like substance |
Key point: Cushing syndrome from lung cancer shows elevated pro-opiomelanocortin (POMC) in serum - a marker NOT found in pituitary-driven Cushing disease.
PTHrP from squamous cell carcinoma - "like PTH, it increases bone resorption and renal calcium uptake while inhibiting renal phosphate transport, raising serum calcium." (Robbins, Cotran & Kumar, p. 312)
II. Neuromuscular / Neurological Syndromes
| Syndrome | Tumor | Mechanism |
|---|---|---|
| Lambert-Eaton Myasthenic Syndrome (LEMS) | SCLC | Anti-VGCC antibodies; proximal muscle weakness that improves with repeated stimulation |
| Peripheral neuropathy | Bronchogenic carcinoma | Immune-mediated (anti-Hu antibodies in SCLC) |
| Cortical cerebellar degeneration | Bronchogenic carcinoma | Anti-Yo, anti-Hu antibodies |
| Encephalomyelitis | SCLC | Autoimmune |
| Myasthenia gravis | Thymoma/bronchogenic carcinoma | Immune - anti-AChR antibodies |
III. Dermatological Syndromes
| Syndrome | Description |
|---|---|
| Acanthosis nigricans | Gray-black, velvety, hyperkeratotic skin patches (axillae, neck); associated with lung and gastric carcinoma; mediated by EGF secretion |
| Dermatomyositis | Proximal muscle weakness + heliotrope rash/Gottron's papules; immunologic mechanism |
IV. Osseous / Articular Syndromes
| Syndrome | Description |
|---|---|
| Hypertrophic pulmonary osteoarthropathy (HPO) | Periosteal new bone formation at distal long bones; painful swelling of wrists, ankles, knees; mechanism unknown |
| Clubbing of fingers | Almost pathognomonic for bronchogenic carcinoma; may resolve after tumor resection |
V. Vascular / Hematologic Syndromes
| Syndrome | Tumor | Mechanism |
|---|---|---|
| Migratory thrombophlebitis (Trousseau sign) | Pancreatic + bronchogenic carcinoma | Tumor mucins activate clotting cascade |
| Non-bacterial thrombotic endocarditis (NBTE) | Advanced cancers | Hypercoagulable state |
| DIC | Various | Tumor procoagulants |
Summary: Paraneoplastic Syndromes by Tumor Type
| Tumor Type | Most Associated Paraneoplastic Syndromes |
|---|---|
| Small Cell Carcinoma | Cushing (ectopic ACTH), SIADH, LEMS, peripheral neuropathy |
| Squamous Cell Carcinoma | Hypercalcemia (PTHrP) |
| Adenocarcinoma | HPO, clubbing, thrombophlebitis |
| Large Cell Carcinoma | Gynecomastia (hCG), HPO |
| Carcinoid | Carcinoid syndrome (serotonin), Cushing |
(Murray & Nadel's Textbook of Respiratory Medicine, p. 403; Robbins, Cotran & Kumar Pathologic Basis of Disease, Tables 7.11, pp. 310-313)
Clinical note: In this specific patient (50-year-old, male, 30-year smoker, central mass), squamous cell carcinoma is the most likely histologic type. If hypercalcemia is found on workup, it strongly supports this diagnosis via PTHrP secretion - a classic paraneoplastic association.
This is a shared conversation. Sign in to Orris to start your own chat.