Serous retinal detachment 10 marks
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive information from both Kanski's Clinical Ophthalmology and the Wills Eye Manual. Here is a complete 10-mark answer on serous (exudative) retinal detachment:
Serous (Exudative) Retinal Detachment
Definition
Serous or exudative retinal detachment (RD) is the separation of the neurosensory retina from the retinal pigment epithelium (RPE) due to the accumulation of subretinal fluid (SRF) in the absence of any retinal break or vitreoretinal traction. Fluid accumulates because of a breakdown of the normal blood-retinal barrier.
Pathogenesis
Under normal conditions, even when fluid leaks from diseased choroidal vessels, the RPE actively pumps the excess fluid back into the choroidal circulation. Exudative RD occurs when this compensatory mechanism is overwhelmed:
- Vascular, inflammatory, or neoplastic disease involving the retina, RPE, or choroid causes fluid to leak outside vessels.
- The subretinal space accumulates protein-rich fluid.
- There is no retinal break — fluid is purely exudative/transudative in origin.
Key TIP: An exudative RD (often caused by a choroidal tumour) is characterized by 'shifting' subretinal fluid — Kanski's Clinical Ophthalmology
Causes (Etiology)
| Category | Examples |
|---|---|
| Neoplastic | Choroidal malignant melanoma, metastases (most common intraocular tumour cause), choroidal haemangioma, multiple myeloma, retinal capillary haemangioblastoma |
| Inflammatory | Vogt-Koyanagi-Harada (VKH) syndrome, posterior scleritis, sympathetic ophthalmia, other chronic inflammatory processes |
| Vascular | Choroidal neovascularization (CNV), Coats disease, malignant hypertension, pre-eclampsia/toxaemia of pregnancy, FEVR |
| Congenital | Optic pit, morning glory syndrome, choroidal coloboma |
| Idiopathic | Central serous chorioretinopathy (CSCR) — rare bullous form; uveal effusion syndrome (bilateral, especially nanophthalmic eyes) |
| Iatrogenic | Post-RD surgery, panretinal photocoagulation |
Rule of thumb: An intraocular tumour should be considered the cause of exudative RD until proved otherwise.
Symptoms
- Visual field defect with varying degrees of vision loss
- Visual changes may vary with changes in head position (pathognomonic)
- Photopsia is typically absent (no vitreoretinal traction)
- Floaters may be present if associated vitritis exists
- Bilateral involvement possible depending on cause (e.g., VKH, toxaemia of pregnancy)
Signs
Critical features:
- Serous elevation of the retina with shifting SRF on positional change
- Sitting upright → SRF accumulates inferiorly, detaching inferior retina
- Supine position → SRF shifts posteriorly, detaching the macula
- No retinal break identified
- Detachment typically does not extend to the ora serrata
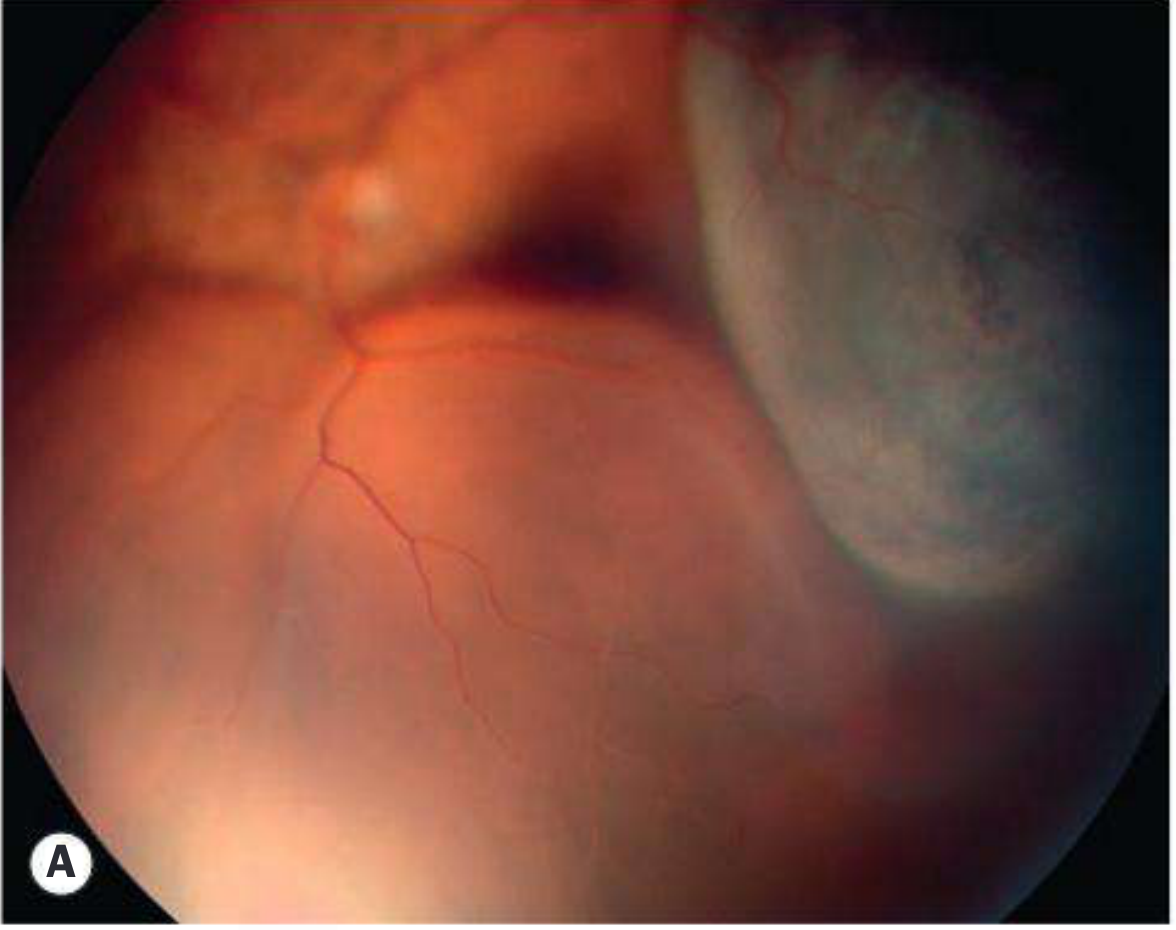
- Retina surface is smooth (not corrugated as in rhegmatogenous RD) and may become bullous
- The detached retina is highly mobile
- Mild relative afferent pupillary defect (RAPD) may be present in large detachments
- 'Leopard spots' — scattered subretinal pigment clumping — may appear after the detachment resolves
- The underlying cause (e.g., choroidal tumour) may be visible on fundoscopy or B-scan
Differentiating Exudative from Other Types of RD
| Feature | Exudative/Serous | Rhegmatogenous | Tractional |
|---|---|---|---|
| Retinal break | Absent | Present | Absent |
| Traction | Absent | Absent | Present |
| Shifting fluid | Present (pathognomonic) | Absent | Absent |
| Surface | Smooth, bullous | Corrugated | Concave, immobile |
| Photopsia | Absent | Common | Absent |
| Ora serrata | Does not reach | Extends to | Does not reach |
Investigations (Workup)
- Fundoscopy — assess character of detachment, identify underlying lesion
- Intravenous Fluorescein Angiography (IVFA) — demonstrates leakage or pooling and identifies the SRF source
- OCT (Optical Coherence Tomography) — identifies the source of SRF (e.g., CNV); shows smooth subretinal fluid dome
- B-scan Ultrasonography — helps delineate the underlying cause (tumour, posterior scleritis); shows mobile retina
- Systemic workup — to rule out inflammatory, neoplastic, or vascular causes (BP, autoimmune screen, chest X-ray, oncology)
- Fundus Autofluorescence (FAF) — demonstrates hyperautofluorescence in areas of serous detachment
Treatment
Treatment is directed at the underlying cause:
- Neoplastic causes — treat the primary tumour (photocoagulation, PDT, radiotherapy, enucleation for melanoma)
- Inflammatory causes (VKH, posterior scleritis) — systemic corticosteroids
- CSCR with bullous detachment — the leaking RPE site may be sealed by laser photocoagulation or PDT
- Choroidal haemangioma — PDT; laser photocoagulation (low success rate)
- Some cases resolve spontaneously after treatment of the underlying cause
- Anti-VEGF injections for CNV-driven exudative detachment
Complications (if untreated)
- Chronic macular damage with permanent visual loss
- 'Leopard spot' RPE atrophy after resolution
- Choroidal neovascularization as a secondary complication
- Phthisis bulbi (end-stage)
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Ed., pp. 706–707 | The Wills Eye Manual, pp. 768–769
Diagnosis and management foe 10 marks
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive material. Here is a detailed 10-mark answer on the diagnosis and management of serous/exudative retinal detachment:
Diagnosis and Management of Serous (Exudative) Retinal Detachment
A. DIAGNOSIS
1. Clinical Diagnosis
History
- Painless visual field defect with variable vision loss
- Visual changes that shift with head position — the hallmark of exudative RD
- No flashing lights (photopsia) — absence distinguishes it from rhegmatogenous RD
- Possible bilateral involvement (VKH, toxaemia of pregnancy)
- History of systemic disease: hypertension, malignancy, autoimmune disease, steroid use
Fundoscopic Findings (Ophthalmoscopy)
- Smooth, bullous, convex elevation of the detached retina (not corrugated)
- Shifting subretinal fluid (SRF) — classic and pathognomonic
- Sitting: SRF collects inferiorly → inferior retinal detachment
- Supine: SRF shifts to posterior pole → macular detachment
- No retinal break identifiable
- Does not extend to the ora serrata
- Highly mobile retina
- Underlying lesion (tumour, haemangioma) may be visible
- 'Leopard spots' — scattered subretinal pigment clumping after resolution
2. Investigations
A. Optical Coherence Tomography (OCT)
- First-line investigation
- Shows optically empty subretinal space (neurosensory elevation)
- Identifies RPE detachments, precipitates on posterior retinal surface
- Quantifies SRF height — correlates with disease activity (especially in VKH)
- Detects subretinal septae (VKH), CNV membranes, RPE tears
- Thickened choroid seen in CSCR (pachychoroid)
B. Fundus Fluorescein Angiography (FFA/IVFA)
- Demonstrates leakage or pooling from the SRF source
- Choroidal tumour: irregular hyperfluorescence with late staining
- CSCR (Central Serous Chorioretinopathy):
- Early: hyperfluorescent spot at RPE leak site
- Expands as an "ink-blot" (most common) or "smokestack" pattern (less common)
- Late: pooling of dye within the detachment
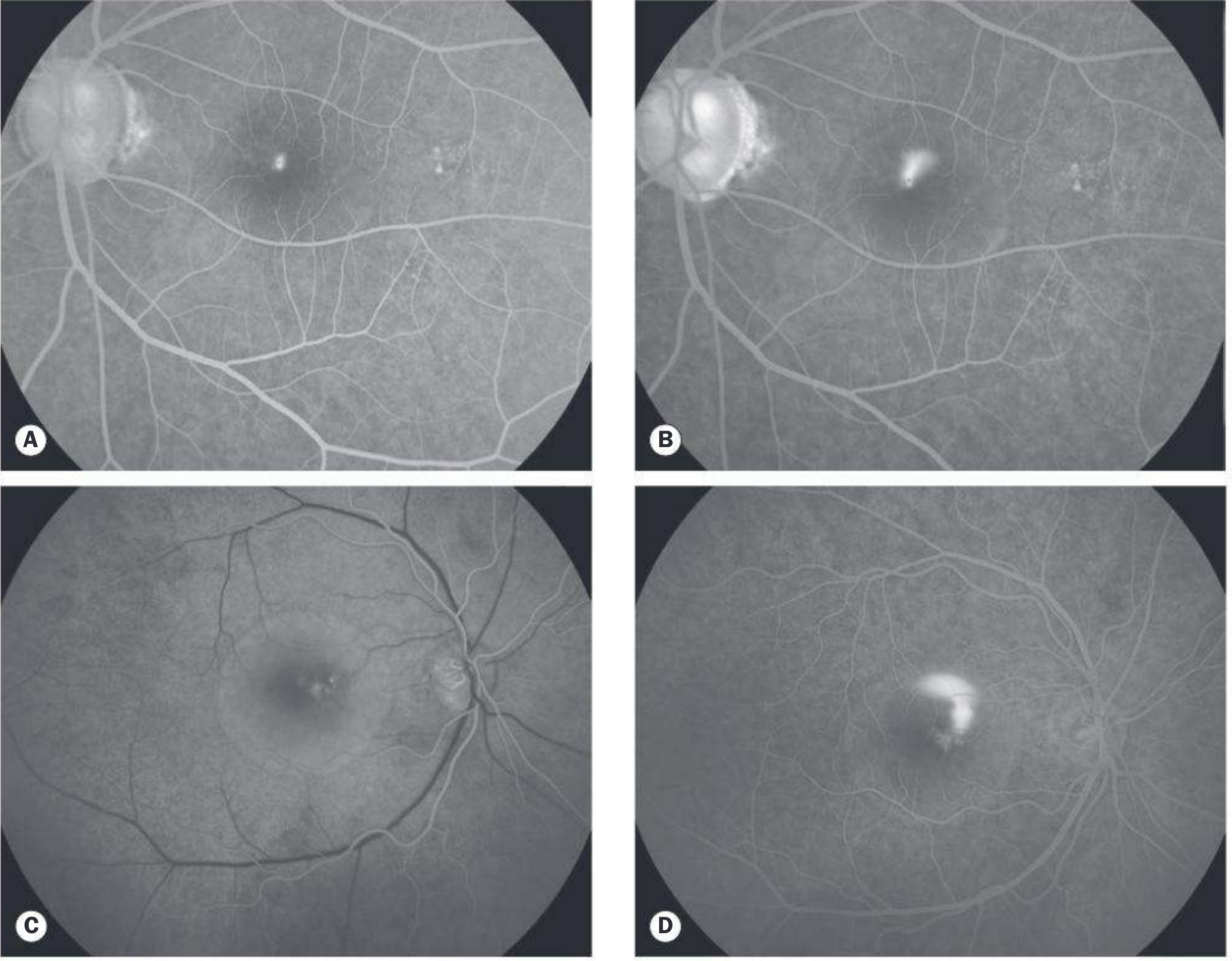
- VKH: Multifocal hyperfluorescent dots at RPE level → subretinal pooling in acute phase; RPE window defects in chronic phase
- Posterior scleritis: Associated disc swelling, choroidal folds
C. B-Scan Ultrasonography
- Identifies the underlying cause: choroidal tumour (elevated, acoustically solid), diffuse choroidal thickening (VKH, posterior scleritis)
- Demonstrates highly mobile retina on dynamic B-scan
- Excludes posterior scleritis (diffuse choroidal thickening + T-sign of posterior scleritis)
- Helpful when media opacities prevent fundal view
D. Fundus Autofluorescence (FAF)
- Hyperautofluorescence in areas of active serous detachment (VKH)
- Hypoautofluorescence at RPE leakage site and old lesion sites (CSCR)
- Gravitational tract (dependent SRF tracking) visible in chronic CSCR
E. Indocyanine Green Angiography (ICGA)
- In VKH: regularly distributed hypofluorescent spots in acute phase; diffuse posterior pole hyperfluorescence in late phase; useful for monitoring
- In CSCR: dilated choroidal vessels, choroidal hyperpermeability in mid-phase; identifies subclinical foci
F. Systemic Workup (to identify underlying cause)
- Blood pressure measurement (malignant hypertension)
- Urinalysis / obstetric review (pre-eclampsia/toxaemia)
- Oncology screen: chest X-ray, CT thorax/abdomen/pelvis, tumour markers (metastasis)
- Autoimmune screen: ANA, HLA-B27, ACE, chest X-ray (sarcoid, VKH)
- Lumbar puncture if VKH uncertain: CSF shows transient lymphocytic pleocytosis + melanin-containing macrophages
G. Amsler Grid
- Confirms metamorphopsia corresponding to the macular detachment (especially in CSCR)
B. MANAGEMENT
The principle is: treat the underlying cause. The exudative RD is a secondary phenomenon and resolves once the primary disease is controlled.
1. Inflammatory Causes
Vogt-Koyanagi-Harada (VKH) Syndrome
- High-dose oral prednisolone 1–2 mg/kg/day, tapered over 3–6 months
- May be preceded by IV methylprednisolone pulse (500–1000 mg/day for 3 days)
- Topical steroids + cycloplegics for anterior uveitis
- Steroid-resistant: immunosuppressives (azathioprine, mycophenolate)
- Biological agents (infliximab) if no response to steroids — use early
Posterior Scleritis
- NSAIDs or systemic corticosteroids
- Immunosuppressives for recurrent/chronic cases
2. Central Serous Chorioretinopathy (CSCR)
| Step | Action |
|---|---|
| 1. Observation | Most acute CSCR resolves spontaneously within 3–6 months (~80% cases) |
| 2. Stop steroids | Discontinue all corticosteroid use (including topical/inhaled) — mandatory in chronic/recurrent disease |
| 3. Oral spironolactone | 40 mg twice daily — faster resorption of SRF in acute CSCR |
| 4. Micropulse (subthreshold) diode laser | To RPE leakage site — good results; avoids RPE scarring of conventional laser |
| 5. Photodynamic therapy (PDT) | Half-dose verteporfin PDT (30–50% dose + 50% light) — treatment of choice in chronic/severe CSCR; leads to complete resolution |
| 6. Anti-VEGF | Intravitreal bevacizumab/ranibizumab — mainly if coexisting macular neovascularization (CNV) |
Key TIP: All corticosteroid treatment must be discontinued if possible in chronic or recurrent CSCR — Kanski's Clinical Ophthalmology
3. Neoplastic Causes
| Tumour | Treatment |
|---|---|
| Choroidal melanoma | Brachytherapy (plaque radiotherapy), proton beam radiotherapy, transpupillary thermotherapy, enucleation (large tumours) |
| Choroidal metastasis | Treat primary malignancy; supplemental external beam radiotherapy to eye |
| Choroidal haemangioma | PDT (most effective); laser photocoagulation (low success rate); low-dose external radiotherapy for large lesions |
4. Vascular Causes
| Condition | Treatment |
|---|---|
| Malignant hypertension / pre-eclampsia | Urgent blood pressure control; SRF resolves after delivery / BP normalisation |
| Choroidal neovascularization (CNV) | Intravitreal anti-VEGF agents (ranibizumab, bevacizumab, aflibercept) |
| Coats disease | Laser photocoagulation to telangiectatic vessels; anti-VEGF; vitreoretinal surgery for advanced detachment |
5. Idiopathic / Structural Causes
- Uveal effusion syndrome: sclerotomy / partial-thickness sclerectomy to improve transscleral fluid outflow
- Optic pit with serous detachment: vitrectomy + gas tamponade ± laser photocoagulation around the pit
- Bullous CSCR: PDT ± laser photocoagulation to seal RPE leak
Summary Algorithm
Exudative RD confirmed (smooth, shifting SRF, no break)
↓
Identify underlying cause (FFA, OCT, B-scan, systemic workup)
↓
┌────────────────┬──────────────────┬────────────────────┬──────────────┐
│ Inflammatory │ Neoplastic │ Vascular │ Idiopathic │
│ VKH / scleritis│ Melanoma/mets/ │ HTN/preeclampsia/ │ CSCR / UES │
│ → Systemic │ haemangioma │ CNV/Coats │ → Observe / │
│ steroids / │ → Tumour- │ → Anti-VEGF / │ stop │
│ immuno- │ specific Rx │ BP control │ steroids / │
│ suppressives │ │ │ PDT/laser │
└────────────────┴──────────────────┴────────────────────┴──────────────┘
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Ed., pp. 466–468, 617–620, 706–707 | The Wills Eye Manual, pp. 768–769
Sick
Hope you feel better soon! 🙏
When you're ready to continue studying, just send the next topic and I'll have it ready for you.
This is a shared conversation. Sign in to Orris to start your own chat.