पता दें।
Asking for Preferences
आपका प्रश्न बहुत संक्षिप्त है और इससे यह स्पष्ट नहीं हो रहा कि आप किसका या किस चीज़ का "पता" जानना चाहते हैं।
कृपया थोड़ा और विवरण दें, जैसे:
- किसी स्थान का पता - जैसे "AIIMS दिल्ली का पता बताएं"
- किसी विषय की जानकारी - जैसे "डायबिटीज़ के बारे में पता दें"
- किसी व्यक्ति या संस्था की जानकारी - जैसे "नवकार इंस्टिट्यूट का पता दें"
- कोई और विषय - अपने शब्दों में लिखें
आपका पूरा प्रश्न लिखें, मैं तुरंत सहायता करूंगा।
Regenerative medicine. Aiiii! Tô uuuurra!
Reading File
Searching the Web
regenerative medicine 2026 latest advances stem cells tissue engineering
Searching PubMed
regenerative medicine stem cells tissue engineering
Finding Sources
Reading File
Reading File
Reading File
Reading File
Here is a thorough overview of Regenerative Medicine:
What is Regenerative Medicine?
Regenerative medicine seeks to harness methods for the replacement or repair of dysfunctional cells, tissues, or organs to restore normal function. It draws upon:
- Pharmaceuticals & biologics
- Medical devices
- Cell therapy
- Tissue engineering
- Molecular/gene therapies
The long-term goal is to develop curative strategies for unmet needs like diabetes, heart failure, chronic kidney disease, traumatic tissue loss, and neurodegenerative disorders. (Goldman-Cecil Medicine, p. 331)
The Three Pillars
1. Stem Cells - The Raw Material
| Cell Type | Source | Key Feature |
|---|---|---|
| Embryonic Stem Cells (ESCs) | Fertilized blastocyst | Totipotent; risk of teratoma, ethical issues |
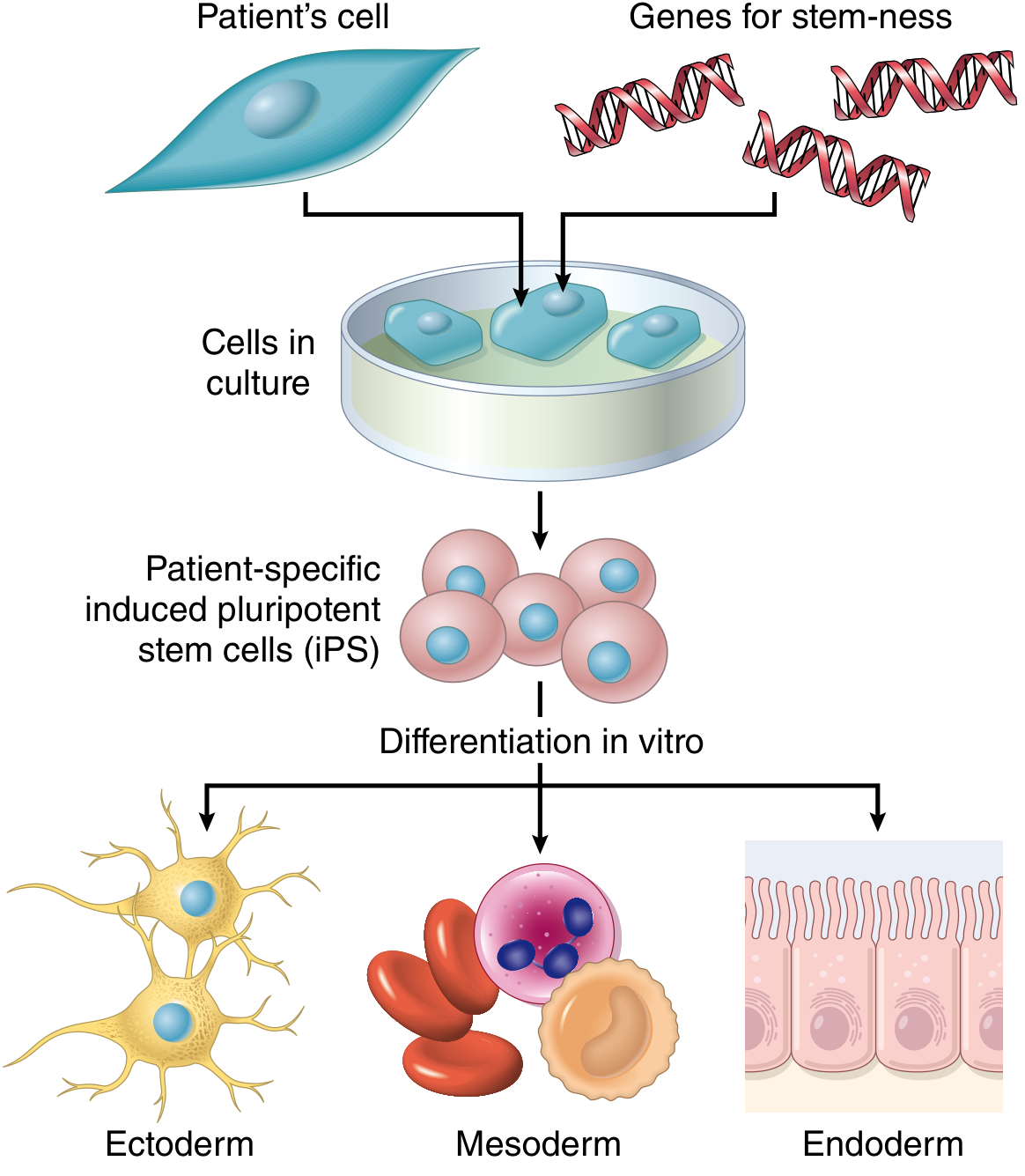
| Induced Pluripotent Stem Cells (iPSCs) | Adult somatic cells (e.g. fibroblasts) reprogrammed via transcription factors (Oct-3/4, Sox2, Klf4, c-Myc) | Patient-specific; no rejection |
| Mesenchymal Stem Cells (MSCs) | Bone marrow, adipose tissue | Relatively immune-privileged |
| Hematopoietic Stem Cells | Bone marrow / blood | Proven in transplantation |
iPSCs were discovered in 2006 in mice and 2007 in humans by Yamanaka & Takahashi - a Nobel Prize-winning breakthrough. Patient-derived iPSCs can also serve as "avatars" to study disease and screen drugs in vitro. (Sabiston Surgery, p. 1026)
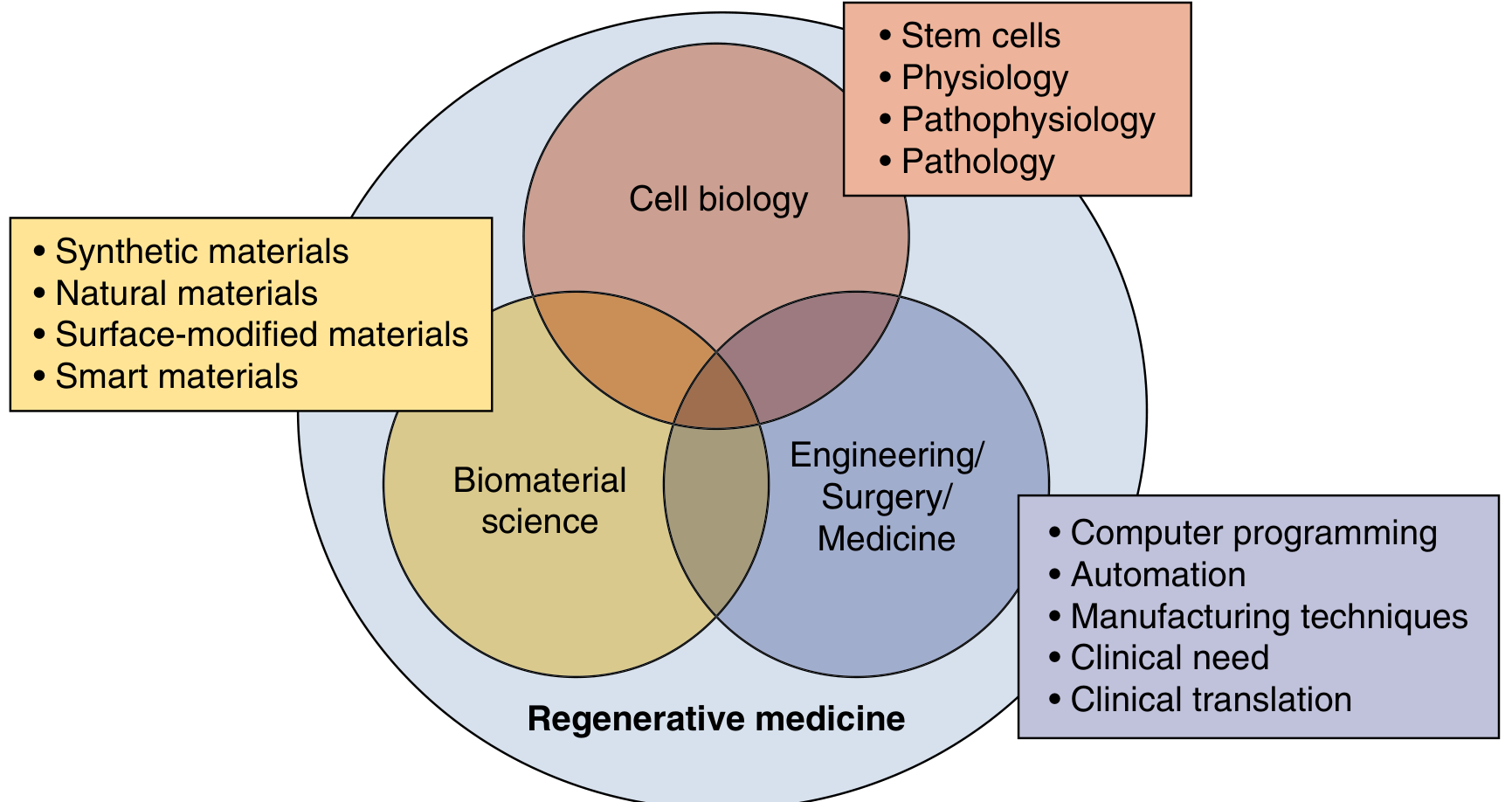
2. Tissue Engineering
Combines cell biology, biomaterial science, and engineering to build functional tissues. Key steps:
- Harvest cells from the patient (autologous) or donor (allogeneic)
- Seed cells onto a scaffold (natural or synthetic biomaterial)
- Culture and condition the construct
- Implant into the patient
Decellularization is a major approach: strip a donor organ of all cells, leaving a collagen scaffold, then repopulate with the patient's own cells. This dramatically reduces rejection risk.
3. Gene Therapy & Gene Editing
- Transfer of DNA, siRNA, or modified RNA into cells to correct inherited disorders or alter cellular function
- CRISPR-Cas9 system now allows direct correction of mutations at the DNA level (rather than just overexpressing missing proteins)
- Recent clinical trials show encouraging benefits and an excellent safety record (Goldman-Cecil Medicine, p. 332)
Clinical Applications (What's Already in Use)
| Application | Product/Example | Status |
|---|---|---|
| Burn wound coverage | Integra (dermal matrix), Epicel (keratinocyte sheets), Apligraf | Approved & widely used |
| Autologous burn repair | ReCell (Avita Medical) - epithelial cell suspension | FDA approved |
| Tissue-engineered bladder | First bench-to-bedside organ implant | Clinical |
| Urethras and vaginas | Tissue-engineered constructs | Clinical |
| Bone marrow transplant | Hematopoietic stem cells | Gold standard for decades |
| CAR-T cell therapy | Gene-modified immune cells for cancer | FDA approved |
| Endometrial disorders | Stem cell-based therapies | Clinical trials (PMID 38796750) |
Key Challenges
- Integration - Introducing cells and functionally connecting them at the damage site
- Immunologic rejection - Most stem cells express HLA antigens; iPSCs solve this for autologous use
- Teratoma risk - ESCs and incompletely differentiated iPSCs can form tumors
- Scale & manufacturing - Moving from lab to mass production
- Ethics - ESC derivation from human embryos remains controversial
Why It Matters Economically
The healthcare cost burden of the diseases regenerative medicine targets is enormous:
- Heart failure: ~$81 billion/year in the US
- Kidney failure: ~$215 billion/year in the US
The global regenerative medicine market was valued at ~$43.77 billion in 2025 and is projected to reach $234 billion by 2035 (CAGR ~18%), driven by iPSC advances, gene editing, and 3D bioprinting. (Sabiston Surgery, p. 1026; BioSpace 2025)
Sources: Robbins Pathologic Basis of Disease (p. 44); Goldman-Cecil Medicine (pp. 331-332); Sabiston Textbook of Surgery (pp. 1025-1030)
This is a shared conversation. Sign in to Orris to start your own chat.