Pituitary and thyroid diseases
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive medical student-level overview of both pituitary and thyroid diseases, drawn from Robbins & Kumar Basic Pathology and Textbook of Family Medicine.
Pituitary and Thyroid Diseases - Medical Student Overview
PART 1: THE PITUITARY GLAND
Anatomy & Physiology
The pituitary is a small, bean-shaped gland at the base of the brain within the sella turcica. It has two lobes:
- Anterior lobe (adenohypophysis) - epithelial cells derived from the oral cavity; produces trophic hormones
- Posterior lobe (neurohypophysis) - modified glial cells (pituicytes) and axonal processes from the hypothalamus
The hypothalamic-pituitary axis controls hormone release through stimulatory and inhibitory factors:
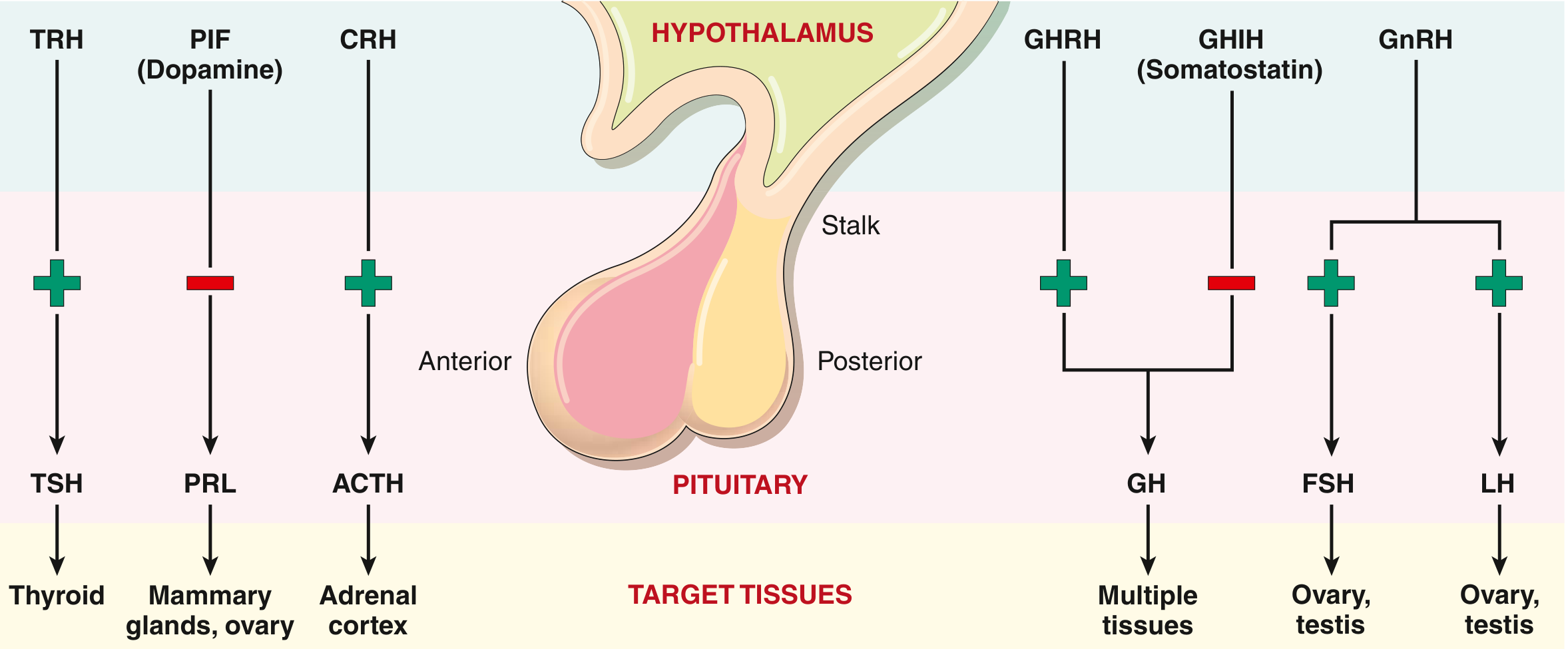
Anterior pituitary cell types and hormones:
| Cell Type | Hormone(s) |
|---|---|
| Somatotrophs | GH (growth hormone) |
| Lactotrophs | PRL (prolactin) |
| Mammosomatotrophs | GH + PRL |
| Corticotrophs | ACTH, POMC, MSH |
| Thyrotrophs | TSH |
| Gonadotrophs | FSH, LH |
Posterior pituitary stores and releases ADH (antidiuretic hormone) and oxytocin - both synthesized in the hypothalamus.
Clinical Presentations of Pituitary Disease
Pituitary disease produces symptoms in three ways:
-
Local mass effects - expanding lesions compress the optic chiasm -> bitemporal hemianopsia (most classic finding). Also cause headache, nausea, vomiting from raised intracranial pressure.
- Pituitary apoplexy: acute hemorrhage into a pituitary tumor -> sudden enlargement + loss of consciousness. This is a neurosurgical emergency.
-
Hyperpituitarism - excess secretion of trophic hormones, most often from an anterior pituitary adenoma.
-
Hypopituitarism - deficiency of trophic hormones from ischemic injury, surgery, radiation, inflammation, or nonfunctional adenomas.
Anterior Pituitary Adenomas (Key Exam Tumors)
Formerly called "pituitary adenomas," now officially termed pituitary neuroendocrine tumors (PitNETs) - though "adenoma" remains in common use.
Classification:
- Microadenoma: <1 cm
- Macroadenoma: >1 cm (more likely to cause mass effects)
| Adenoma Type | Hormone | Key Clinical Features |
|---|---|---|
| Prolactinoma | PRL | Most common. Women: amenorrhea, galactorrhea, infertility. Men: impotence, decreased libido. Tx: dopamine agonists (cabergoline, bromocriptine) |
| GH-secreting | GH | Gigantism (before epiphyseal fusion) / Acromegaly (after fusion) - enlarged hands, feet, jaw (prognathism) |
| ACTH-secreting | ACTH | Cushing disease - central obesity, moon face, buffalo hump, striae, hypertension, hyperglycemia |
| TSH-secreting | TSH | Rare; causes secondary hyperthyroidism |
| Null cell / nonfunctional | None | Causes mass effects and hypopituitarism |
Diagnosis: hormone assays + MRI of the sella turcica.
Hypopituitarism
Causes include:
- Nonfunctional adenoma compressing normal gland
- Sheehan syndrome (postpartum ischemic necrosis of pituitary)
- Craniopharyngioma (most common pituitary tumor in children)
- Radiation, surgery, inflammatory disease (sarcoidosis, TB)
Deficiencies appear in order: GH first, then FSH/LH, then TSH, then ACTH (ACTH last = most resilient).
Posterior Pituitary - Diabetes Insipidus
ADH deficiency (central DI) or renal resistance to ADH (nephrogenic DI) -> polyuria + polydipsia + dilute urine. Treated with desmopressin (DDAVP) in central DI.
PART 2: THE THYROID GLAND
Key Physiology
- Hypothalamus releases TRH -> Anterior pituitary releases TSH -> Thyroid produces T4 (thyroxine) and T3 (triiodothyronine)
- T3 is the active form (T4 is converted peripherally to T3)
- Classic negative feedback: high T3/T4 suppresses TSH
Hyperthyroidism (Thyrotoxicosis)
Diagnosis: suppressed TSH (<0.1 mIU/L) + elevated free T4 (and/or T3).
Common causes:
| Cause | Key Feature |
|---|---|
| Graves disease | Most common. TSH receptor-stimulating antibodies (TSH-RS Abs) mimic TSH. Diffuse goiter + ophthalmopathy (exophthalmos) + pretibial myxedema |
| Toxic multinodular goiter (Plummer disease) | Multiple autonomously functioning nodules |
| Toxic adenoma | Single autonomous nodule (gain-of-function mutation in TSH receptor or GNAS) |
| Subacute thyroiditis | Transient thyrotoxicosis followed by hypothyroidism |
| TSH-secreting pituitary adenoma | Rare secondary hyperthyroidism |
Symptoms of hyperthyroidism (hypermetabolic state):
- Tachycardia, wide pulse pressure, systolic hypertension
- Weight loss, diarrhea
- Anxiety, tremor, irritability
- Warm, moist skin
- Proximal muscle weakness (thyroid myopathy, ~50%)
- Exophthalmos (Graves-specific)
Thyroid storm: acute severe hyperthyroidism - triggered by infection, surgery, or stress. Medical emergency; significant mortality from cardiac arrhythmias.
Apathetic hyperthyroidism: seen in elderly patients, where classic features are blunted - presents as unexplained weight loss or worsening heart disease.
Graves disease - long-term treatment options:
- Antithyroid drugs (PTU or methimazole/MMI)
- Radioactive iodine (¹³¹I) ablation
- Thyroidectomy
Radioactive iodine scan findings:
- Graves: diffuse uptake
- Toxic adenoma: focal uptake in nodule
- Thyroiditis: decreased uptake
Hypothyroidism
Diagnosis: elevated TSH (>10 mIU/L in overt hypothyroidism) + low free T4.
Causes:
| Category | Examples |
|---|---|
| Primary (most common) | Hashimoto thyroiditis, iodine deficiency, surgery/radiation, drugs (lithium, amiodarone) |
| Secondary | Pituitary failure (low TSH + low T4) |
| Congenital | Thyroid dysgenesis or dyshormonogenesis |
Hashimoto thyroiditis (Chronic Autoimmune Thyroiditis - CAT):
- Most common cause in the developed world
- Female:male ratio = 10-14:1, typically diagnosed in 5th decade
- Anti-TPO antibodies (primary) and anti-thyroglobulin antibodies attack thyroid stroma -> progressive fibrosis
- Treatment: L-thyroxine replacement (average dose 1.6 mcg/kg/day)
- TSH monitored annually
Congenital hypothyroidism: Iodine deficiency is the most common cause worldwide (affecting ~2 billion people). If untreated, causes cretinism (severe intellectual disability + growth retardation).
Symptoms of hypothyroidism (hypometabolic state):
- Fatigue, cold intolerance, weight gain
- Constipation, bradycardia
- Dry skin, coarse hair, hair loss
- Myxedema (non-pitting edema)
- Delayed deep tendon reflexes
- In children: growth retardation, intellectual disability
Treatment: L-thyroxine replacement alone. Some patients may need combined T4+T3 if symptoms persist despite TSH in range.
Thyroid Nodules and Neoplasms
Multinodular goiter (MNG):
- Enlarged thyroid with multiple nodules due to iodine deficiency or other factors
- Follicles filled with stored colloid, lined by flattened epithelium
- May become "toxic" (hyperthyroid) - called Plummer disease
Follicular adenoma:
- Benign, solitary, encapsulated tumor derived from follicular epithelium
- Most are nonfunctional (cold nodule on scan); a few are toxic (hot nodule)
- Key hallmark: intact capsule - distinguishes it from follicular carcinoma
- Mutations: TSH-receptor or GNAS gain-of-function in toxic adenomas; RAS or PTEN mutations in nonfunctioning adenomas
Thyroid Cancers (exam high-yield summary):
| Type | Key Feature | Prognosis |
|---|---|---|
| Papillary (most common, ~85%) | Orphan Annie eye nuclei, psammoma bodies, nuclear grooves; RET/PTC and BRAF mutations | Excellent |
| Follicular | Capsular/vascular invasion (must check capsule); hematogenous spread | Good |
| Medullary | Calcitonin-secreting C-cells; amyloid stroma; associated with MEN2 | Moderate |
| Anaplastic | Undifferentiated; most aggressive; local invasion rapid | Poor (weeks-months) |
Quick Lab Reference
| Condition | TSH | Free T4 |
|---|---|---|
| Primary hyperthyroidism | Low | High |
| Secondary hyperthyroidism (pituitary TSHoma) | High/normal | High |
| Primary hypothyroidism | High | Low |
| Secondary hypothyroidism (pituitary failure) | Low/normal | Low |
| Subclinical hyperthyroidism | Low | Normal |
| Subclinical hypothyroidism | High | Normal |
Sources: Robbins & Kumar Basic Pathology, Chapter 18 (Endocrine System); Textbook of Family Medicine 9e, Chapter 35 (Thyroid and Pituitary Diseases)
This is a shared conversation. Sign in to Orris to start your own chat.