Pcos
Reading File
Finding Sources
Searching PubMed
"polycystic ovary syndrome"[MeSH Terms] AND management
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content. Let me compile the full answer.
Polycystic Ovary Syndrome (PCOS)
Definition
PCOS is a heterogeneous endocrine disorder defined by the Rotterdam criteria: diagnosis requires any 2 of the following 3 features, after excluding other causes:
- Oligo-ovulation or anovulation
- Hyperandrogenism (clinical or biochemical)
- Polycystic ovaries on ultrasound (≥12 follicles per ovary, or increased ovarian volume >10 mL)
- Goldman-Cecil Medicine, p. 2560
Epidemiology
- Affects 6-12% of women of reproductive age - the most common endocrine abnormality in this group
- No clear geographic or ethnic predilection
- More than 50% of affected women develop type 2 diabetes by age 40
- Obesity amplifies the syndrome and is increasingly prevalent alongside it
Pathophysiology
The core defect involves inappropriate gonadal steroid feedback on the hypothalamic-pituitary axis:
- The hypothalamic-pituitary unit is structurally intact but functionally deranged
- Insulin-like growth factors within the ovary contribute to abnormal gonadotropin secretion
- LH is typically elevated relative to FSH (LH:FSH ratio >3), driving excess androgen production from theca cells
- Insulin resistance and compensatory hyperinsulinemia are present across all racial/ethnic groups
- Hyperinsulinemia directly stimulates ovarian androgen production and reduces hepatic SHBG synthesis, raising free testosterone
- Genetic factors include alterations in CYP17 (17α-hydroxylase) and CYP19 (aromatase)
A severely affected subset has ovarian hyperthecosis - markedly increased androgen-producing stromal, hilar, and thecal cells - presenting with acanthosis nigricans, hyperuricemia, severe hirsutism, and glucose intolerance.
Clinical Features
| Feature | Details |
|---|---|
| Menstrual irregularity | Oligomenorrhea, amenorrhea, or dysfunctional uterine bleeding |
| Hirsutism | Androgen-driven terminal hair in male-pattern distribution |
| Acne | Androgen-driven sebaceous gland stimulation |
| Obesity | Central/visceral pattern; present in ~50-60% |
| Infertility | Anovulation is the predominant cause |
| Acanthosis nigricans | Marker of insulin resistance |
| Androgenic alopecia | Temporal hair thinning |
Symptoms usually begin at puberty and worsen over time, with some improvement near menopause.
Diagnostic Evaluation
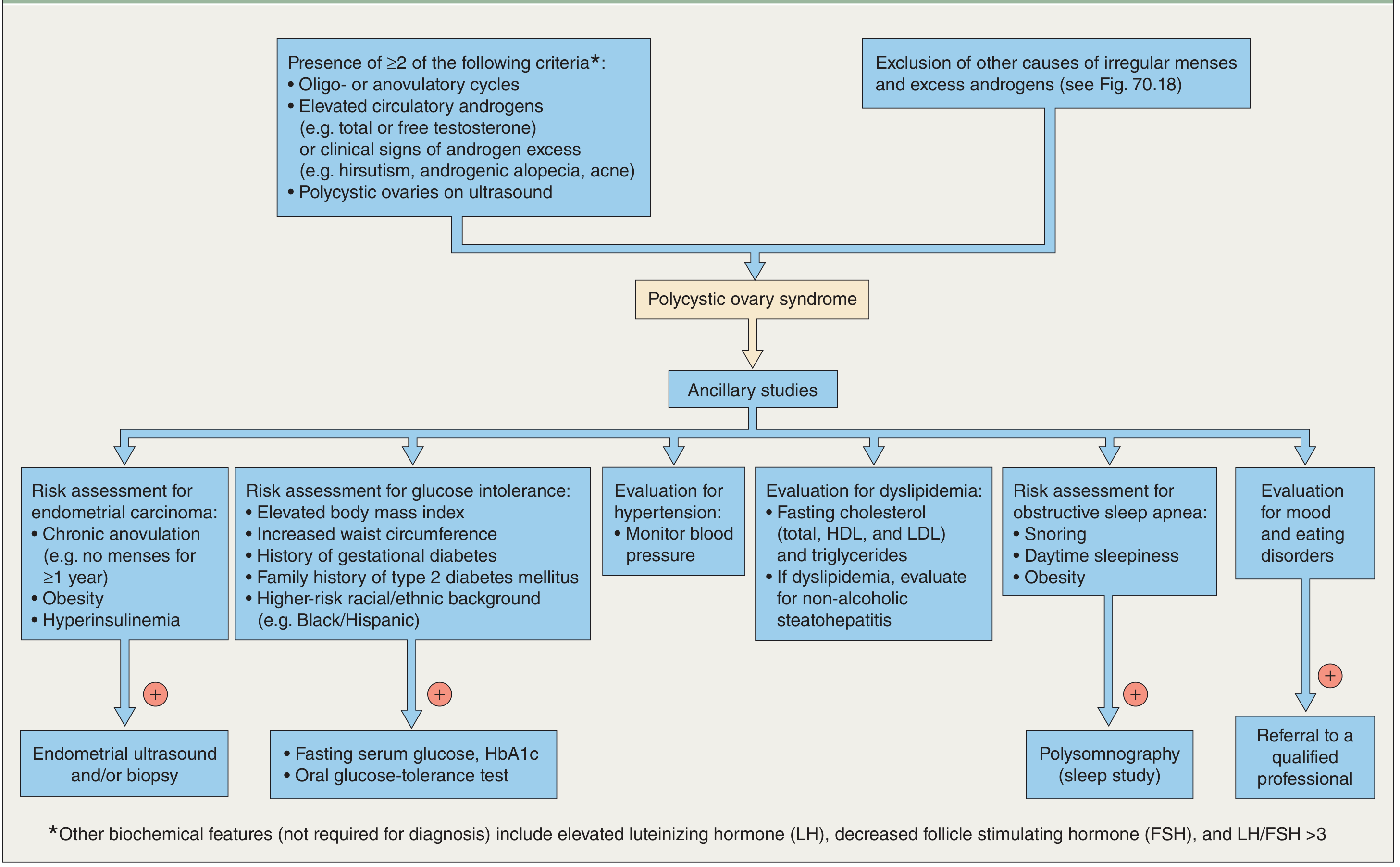
Key investigations:
- Testosterone (total and free) - typically mildly to moderately elevated
- LH/FSH ratio - often >3 (not required for diagnosis but supportive)
- SHBG - reduced in insulin resistance
- DHEAS - elevated if adrenal androgen contribution
- Fasting glucose, HbA1c, OGTT - screen for insulin resistance/T2DM
- Fasting lipid panel - metabolic syndrome assessment
- Pelvic ultrasound - polycystic ovarian morphology
- Thyroid function, prolactin, 17-OHP - to exclude mimics
Conditions to exclude before diagnosing PCOS:
- Cushing syndrome
- Congenital adrenal hyperplasia (non-classical)
- Androgen-secreting tumors (ovarian or adrenal)
- Hyperprolactinemia
- Thyroid dysfunction
Long-term Complications
| System | Risk |
|---|---|
| Metabolic | Type 2 diabetes (>50% by age 40), metabolic syndrome |
| Cardiovascular | Hypertension, dyslipidemia, atherosclerosis |
| Endometrial | Endometrial hyperplasia and carcinoma (from chronic unopposed estrogen) |
| Reproductive | Infertility, pregnancy complications (GDM, preeclampsia) |
| Psychological | Depression, anxiety, eating disorders |
| Hepatic | Non-alcoholic fatty liver disease |
| Sleep | Obstructive sleep apnea (especially in obese patients) |
Management
Management is goal-directed and individualized based on the patient's primary concerns.
1. Lifestyle Modification (First Line for All)
-
Weight loss of just 5-7% over 6 months can significantly reduce free testosterone, restore ovulation in >75% of women, and improve insulin sensitivity
-
Exercise targeting large muscle groups (e.g., thighs) reduces insulin resistance
-
Relevant for all phenotypes regardless of BMI
-
Berek & Novak's Gynecology, p. 1935
2. Menstrual Regulation / Endometrial Protection
- Combined oral contraceptives (COCs): First-line for women not desiring pregnancy
- Suppress LH → ↓ ovarian androgen production
- ↑ hepatic SHBG → ↓ free testosterone
- ↓ DHEAS levels
- Protect endometrium from hyperplasia
- Cyclic progestins: (e.g., medroxyprogesterone acetate 5-10 mg for 10-14 days/month) for endometrial protection in women who cannot use estrogen; does NOT reliably suppress ovulation
3. Hirsutism / Hyperandrogenism
| Category | Agents |
|---|---|
| Hormonal suppression | COCs, medroxyprogesterone, GnRH analogues, glucocorticoids |
| 5α-reductase inhibitors | Finasteride |
| Antiandrogens | Spironolactone, cyproterone acetate, flutamide |
| Insulin sensitizer | Metformin |
| Steroidogenic enzyme inhibitors | Ketoconazole |
| Mechanical | Electrolysis, laser (permanent); threading, waxing (temporary) |
COCs reduce hair growth in nearly two-thirds of hirsute patients. Note: antiandrogens require effective contraception due to teratogenicity (feminization of male fetus).
4. Ovulation Induction (Women Desiring Pregnancy)
- Letrozole (5 mg days 3-7) - preferred first-line; superior to clomiphene for live birth rates in PCOS
- Clomiphene citrate (50 mg days 3-7) - alternative; ~75-80% conception rate with either agent
- Metformin (500-2000 mg/day) - less effective than letrozole/clomiphene for ovulation induction alone, but useful adjunctively
- Exogenous gonadotropins + hCG - specialist-directed, for clomiphene/letrozole-resistant cases
- Laparoscopic ovarian drilling (LOD) - ovarian diathermy or laser; achieves unifollicular ovulation; risk of adhesions limits use to non-responders to medical therapy
5. Metabolic Management
- Metformin 1500-2000 mg/day in divided doses: suppresses hepatic gluconeogenesis, improves insulin sensitivity, reduces androgens, restores ovulation in 60-70% of women
- Screen and manage dyslipidemia, hypertension, and glucose intolerance
- GLP-1 receptor agonists (e.g., semaglutide, liraglutide): 2024 meta-analysis (PMID 39178623) shows efficacy for weight loss and hormonal regulation in obese PCOS women
Recent Evidence (2024-2025)
- Lifestyle interventions remain cornerstone therapy per a 2025 systematic review (PMID 39861440) - exercise and dietary changes improve metabolic and reproductive outcomes
- GLP-1 agonists show significant benefit for weight loss and androgen reduction in obese PCOS (PMID 39178623)
- Probiotics/prebiotics/synbiotics may improve insulin resistance and hormonal profiles in PCOS per a 2024 systematic review (PMID 39599701), though evidence is still emerging
Sources: Goldman-Cecil Medicine, p. 2560; Berek & Novak's Gynecology, pp. 1935-1936; Dermatology 5e (diagnostic flowchart)
This is a shared conversation. Sign in to Orris to start your own chat.