Utero vaginal prolapse detailed description
Reading File
Finding Sources
Finding Sources
Searching PubMed
"uterovaginal prolapse" OR "uterine prolapse" management
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
Reading File
I now have all the information needed to write a comprehensive, detailed answer. Let me compile it.
Uterovaginal Prolapse - Detailed Description
Definition
Uterovaginal prolapse (also called pelvic organ prolapse, POP) is defined as the "descent of one or more of the anterior vaginal wall, posterior vaginal wall, the uterus (cervix), or the apex of the vagina (vaginal vault or cuff scar after hysterectomy)," correlated with symptoms. It is the progressive herniation of the pelvic organs through the urogenital diaphragm, most commonly leading to vaginal bulge symptoms. - Berek & Novak's Gynecology, p. 1594
Epidemiology
- Affects up to 40% of women at some point in their lifetime.
- The prevalence of at least one pelvic floor disorder is 23.7% in the general female population; more than doubles in women aged 80+.
- The lifetime probability a woman will undergo surgical correction for POP is approximately 1 in 8 (12.6%) by age 80.
- The condition is increasingly common as populations age; projections suggest the burden will substantially grow through 2050. - Berek & Novak's Gynecology, p. 1594
Anatomy of Pelvic Support (Three Levels)
Normal pelvic organ support relies on three interconnected levels of connective tissue and muscle:
Level I (Apical/Suspensory): The cardinal and uterosacral ligament complex suspends the uterus and upper vagina from the pelvic side wall. Their origin is at the lateral borders of sacral vertebrae S2-S4, and they insert at the upper vagina and cervix. These are the primary supports against apical descent.
Level II (Lateral Attachment): Lateral connective tissue attachments of the anterior vaginal wall to the arcus tendineus pelvis (white line) and of the posterior vaginal wall to the fascia of the levator ani. Loss of these paravaginal supports leads to cystocele and rectocele.
Level III (Distal/Perineal): Less dense areolar connective tissue surrounding the retroperineal portion of the pelvic organs, including the perineal body and distal vaginal supports.
An intact pelvic floor including a functional puborectalis muscle and an intact cardinal/uterosacral complex prevent POP by posterior deflection of the rectum and vagina and compression of these structures against the pelvic floor in the upright position. - Berek & Novak's Gynecology, pp. 1199-1208
Types of Prolapse
Uterovaginal prolapse is not a single entity but a term encompassing several forms depending on the anatomical compartment involved:
| Type | Compartment | Structures Involved |
|---|---|---|
| Urethrocele | Anterior | Urethra herniates into vagina |
| Cystocele | Anterior | Bladder herniates into anterior vaginal wall |
| Uterine prolapse | Apical/Middle | Descent of uterus and cervix into or through vagina |
| Enterocele | Apical/Posterior | Small bowel descends into posterior vaginal wall |
| Rectocele | Posterior | Rectum herniates into posterior vaginal wall |
| Vaginal vault prolapse | Apical | Post-hysterectomy descent of vaginal apex |
Procidentia = complete prolapse of the uterus through the introitus (maximal descent).
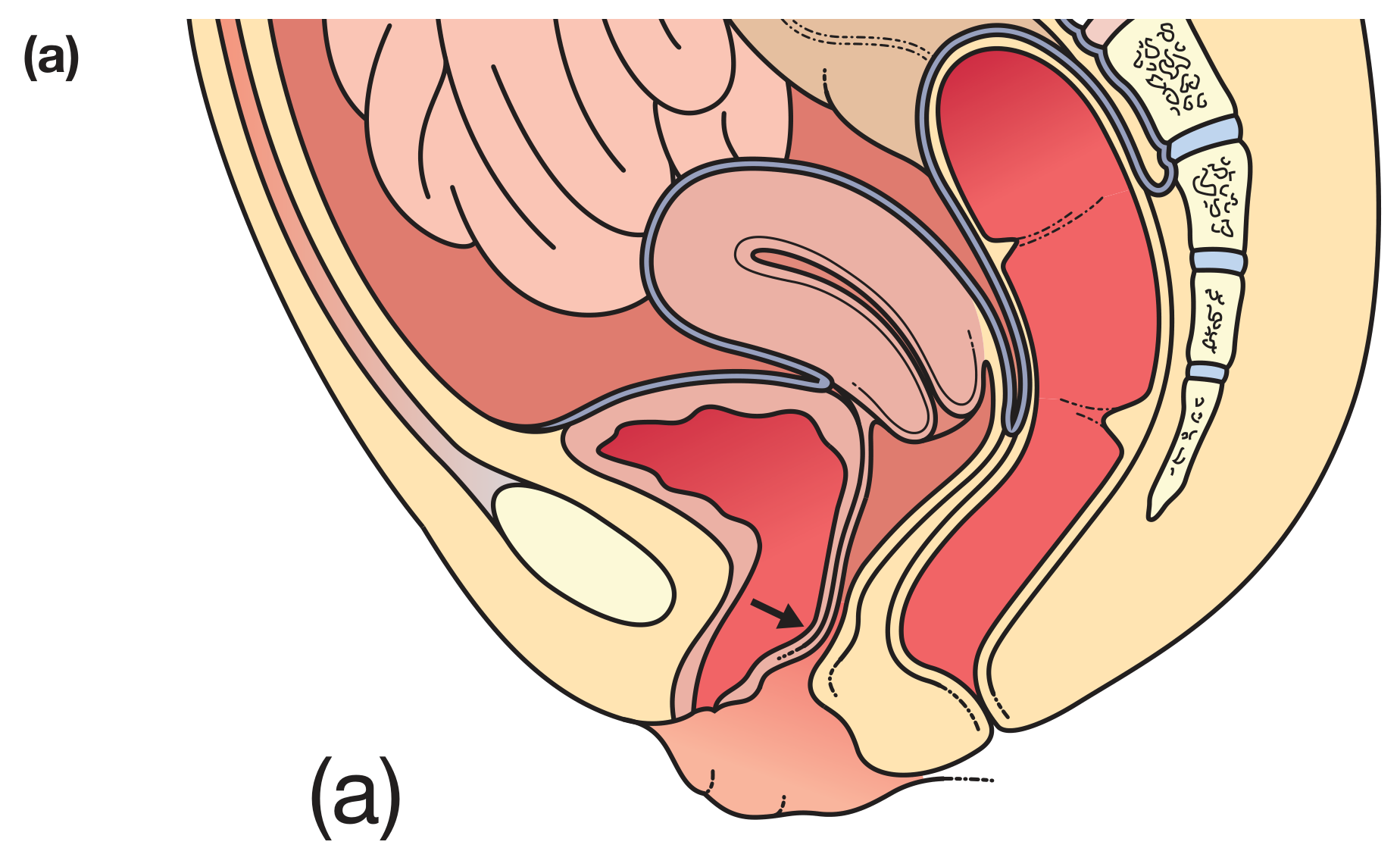
(a) Cystocele/urethrocele:
(d) Vaginal vault prolapse:
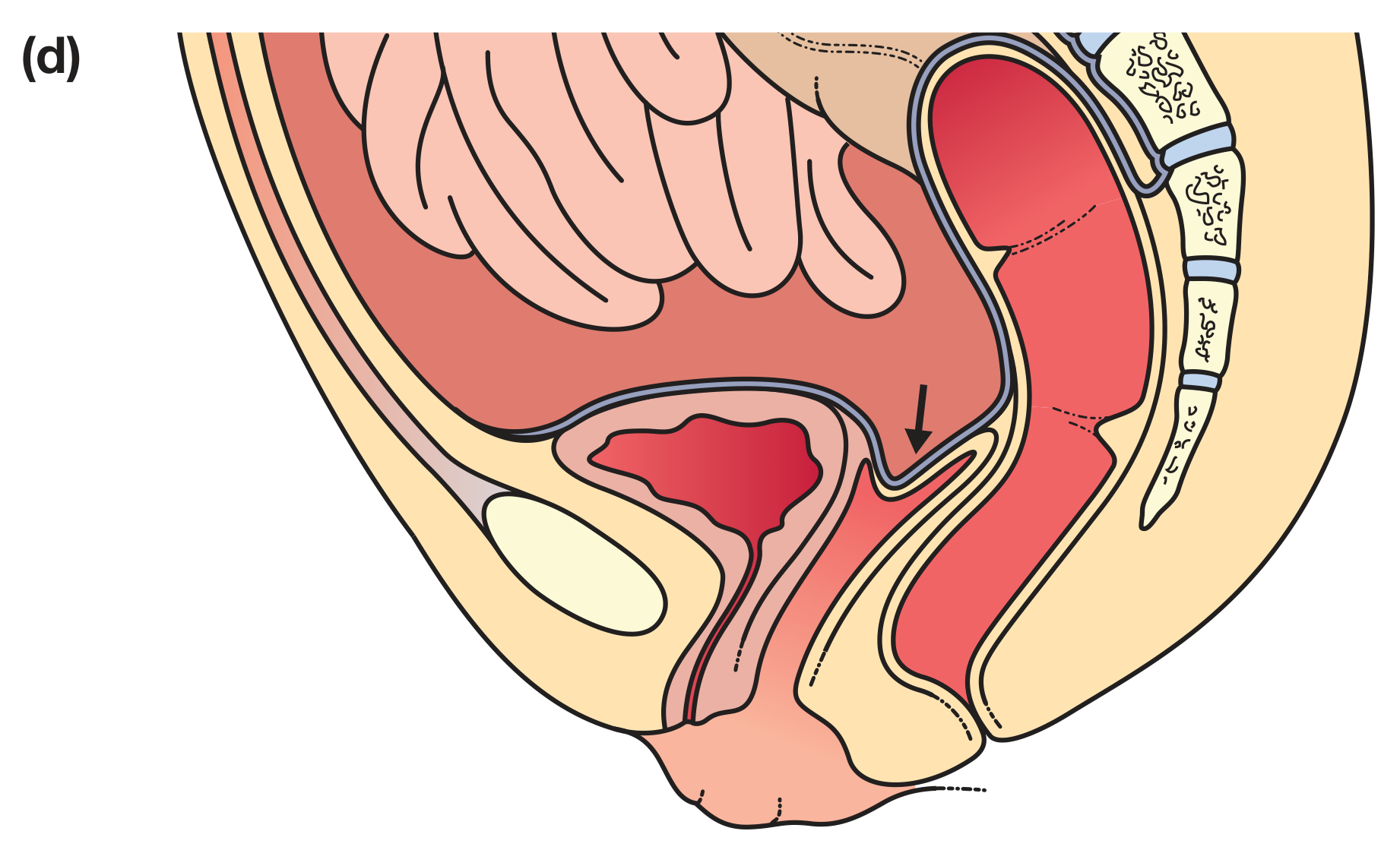
Figure 87.23 - Bailey & Love's Short Practice of Surgery 28th Edition
Risk Factors / Aetiology
Causes are multifactorial, combining structural, hormonal, and mechanical elements:
-
Older age - age is the strongest independent risk factor
-
Parity - vaginal deliveries, high parity, prolonged labours (nerve and tissue trauma)
-
Obesity - increases intra-abdominal pressure chronically
-
Chronic constipation / straining - repeated Valsalva increases downward forces
-
Heavy lifting - occupational or habitual
-
Oestrogen deficiency (menopause) - reduces tissue strength and elasticity
-
Connective tissue disorders - Ehlers-Danlos syndrome, Marfan syndrome
-
Family history / genetic predisposition
-
Bailey & Love's Short Practice of Surgery, p. 1611
Classification and Grading (POP-Q System)
The Pelvic Organ Prolapse Quantification (POP-Q) System, approved by the International Continence Society, is the current standard. It uses nine measurements at specific vaginal landmarks relative to the hymen (hymen = 0; above = negative; below = positive).
POP-Q Stages:
| Stage | Criteria |
|---|---|
| Stage 0 | No prolapse demonstrated |
| Stage I | Most distal portion >1 cm above hymen |
| Stage II | Most distal portion ≤1 cm above or below hymen |
| Stage III | Most distal portion >1 cm below hymen, but <2 cm less than total vaginal length |
| Stage IV | Maximal descent / complete eversion |
Six key anatomical points measured:
- Aa, Ba - anterior compartment (bladder neck and most dependent anterior wall)
- C, D - middle/apical compartment (cervix and posterior fornix)
- Ap, Bp - posterior compartment
Plus genital hiatus (gh), perineal body (pb), and total vaginal length (tvl).
- Berek & Novak's Gynecology, pp. 1352-1368
Clinical Presentation / Symptoms
Women with minor prolapse may be asymptomatic. Symptoms depend on compartment involved:
- General: sensation of "something coming down", feeling of pelvic pressure or heaviness
- Cystocele/urethrocele: lump in the vagina, urinary urgency (OAB), recurrent urinary tract infections, voiding difficulty
- Uterine descent: dragging sensation, vaginal lump; in procidentia - vaginal discharge, mucosa ulceration, and bleeding
- Rectocele: difficulty with defecation, sensation of incomplete emptying, relief with digital reduction of the posterior vaginal wall
- Enterocele: pressure and pelvic heaviness, especially on standing
Associated symptoms may include sexual dysfunction, lower back pain, and urinary or fecal incontinence.
Non-Surgical (Conservative) Management
Indicated for grade 1-2 prolapse or for women who decline surgery or are unfit:
-
Lifestyle modifications:
- Avoidance of constipation
- Weight reduction
- Avoidance of heavy lifting
-
Pelvic floor muscle training (PFMT): Physiotherapy for at least 16 weeks - strengthens the levator ani and pelvic floor. Most effective for grade 1-2 prolapse.
-
Topical oestrogen: Improves tissue strength and elasticity in oestrogen-deficient women.
-
Vaginal pessaries: Mechanical support devices inserted vaginally. Most commonly used is the ring pessary (inserted between posterior fornix and pubic bone). Others include Gellhorn, Donut, Cube, Gehrung, and Hodge pessaries.
- Replaced every 3-6 months
- Main complications: vaginal ulceration, infection, discharge, and bleeding
- Bailey & Love's Short Practice of Surgery, p. 1611-1612
Surgical Management
Surgery aims to restore uterovaginal anatomy and position, relieve symptoms, and where possible maintain sexual function. It is considered when conservative therapy fails or is declined, or when prolapse is Stage II or above with progression.
Surgical procedures fall into three categories:
- Reconstructive (native tissue repair) - uses patient's own endogenous support structures
- Compensatory/augmentative - uses permanent graft material to replace deficient support
- Obliterative - closes/partially closes the vagina (colpocleisis) when sexual function is not desired
Surgical Options by Compartment (Table 87.12 - Bailey & Love):
| Condition | Procedure | Complications |
|---|---|---|
| Urethrocele/Cystocele | Anterior colporrhaphy (anterior vaginal wall repair without mesh) | Bleeding, infection, fistula, voiding dysfunction, unmasking SUI, recurrence |
| Uterine prolapse (family complete) | Vaginal hysterectomy ± sacrospinous fixation | Bleeding, infection, bladder/bowel/ureter injury, voiding dysfunction, dyspareunia, recurrence |
| Uterine prolapse (uterus-preserving) | - Manchester repair (cervical amputation + transverse cervical ligament suture) | Infertility, miscarriage, dystocia (Manchester-specific) |
| - Laparoscopic uterosacral ligament plication (McCall suture) | ||
| - Vaginal hysteropexy (cervix attached to sacrospinous ligaments) | ||
| - Sacrohysteropexy (laparoscopic/abdominal; polypropylene mesh to sacral promontory) | ||
| Enterocele | Enterocele repair | Bleeding, infection, bowel injury, recurrence |
| Vaginal vault prolapse | - Sacrospinous vault fixation (vaginal) | Bleeding, infection, failure, dyspareunia, buttock pain |
| - Sacrocolpopexy (abdominal/laparoscopic; mesh to sacral promontory) | ||
| Rectocele | Posterior colporrhaphy ± levatorplasty | Bleeding, infection, dyspareunia, recurrence |
| Colpocleisis | Total or partial closure of vagina (when no sexual function desired) | Permanent, urinary incontinence unmasking |
Key surgical principles:
-
Apical support is the cornerstone - failure to address the apex increases recurrence risk for all other compartments
-
Approach (vaginal vs. laparoscopic vs. open abdominal) is chosen based on type/severity, surgeon training, and patient preference
-
Concurrent anti-incontinence procedures should be considered
-
"Occult stress urinary incontinence" may be unmasked after anterior repair
-
Bailey & Love's Short Practice of Surgery, pp. 1612-1613; Berek & Novak's Gynecology, pp. 1599-1660
Summary
Uterovaginal prolapse is a common, multifactorial disorder resulting from failure of the pelvic support mechanisms. It encompasses several anatomical compartment defects, graded using the validated POP-Q system. Management is individualised - starting with conservative measures (PFMT, pessaries, oestrogen) and progressing to surgery when needed. Surgical success depends heavily on correct identification of all compartment defects and reliable apical support restoration.
Sources:
- Bailey & Love's Short Practice of Surgery, 28th Edition, Chapter 87
- Berek & Novak's Gynecology, Chapter 30
This is a shared conversation. Sign in to Orris to start your own chat.