Appendix anatomy, vascular,nerve structure, preop indication, indication for surgery, post op management, types of surgery , types of appendix and other important relations refer from Bailey and love
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive data from Bailey and Love. Let me compile the complete, well-structured answer.
The Vermiform Appendix - Bailey and Love's Short Practice of Surgery (28th Edition)
1. Anatomy
General
The vermiform appendix is present only in humans, certain anthropoid apes, and the wombat. It is a blind muscular tube with mucosal, submucosal, muscular, and serosal layers. Morphologically it represents the undeveloped distal end of the large caecum found in many lower animals.
At birth the appendix is short and broad at its junction with the caecum, but differential growth of the caecum produces the typical tubular structure by about age 2 years. During childhood, continued growth commonly rotates the appendix into a retrocaecal but intraperitoneal position.
Gross Anatomy
- Base: Constant in position - found at the confluence of the three taeniae coli of the caecum, which fuse to form the outer longitudinal muscle coat of the appendix. At operation, gentle traction on the taeniae coli (especially the anterior taenia) leads the surgeon to the base of the appendix.
- Mesoappendix: Arises from the lower surface of the mesentery of the terminal ileum. Subject to great variation - sometimes the distal one-third of the appendix is bereft of mesoappendix. In childhood it is transparent enough to see contained blood vessels; in many adults it becomes laden with fat.
- Length: Average 7.5-10 cm. The lumen is irregular, encroached on by multiple longitudinal folds of mucous membrane lined by columnar cell intestinal mucosa of colonic type.
Microscopic Anatomy
- Crypts present but not numerous
- Base of crypts contains argentaffin (Kulchitsky) cells - may give rise to neuroendocrine tumours (NETs)
- Submucosa contains numerous lymphatic aggregations/follicles - prominent in young adults; important in aetiology of appendicitis
- Walls: mucosal, submucosal, muscularis propria, serosal layers
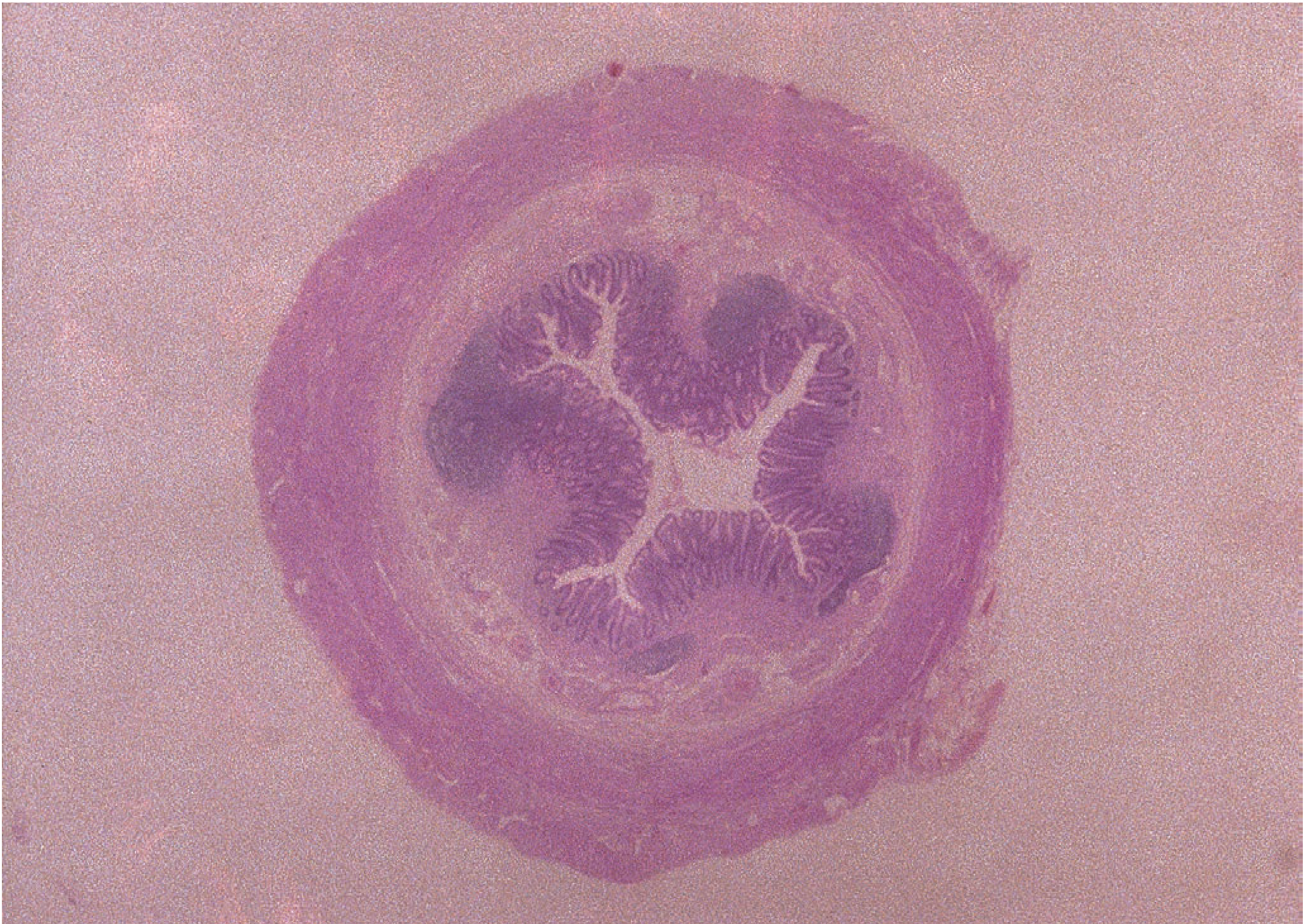
Fig 76.4 - Normal vermiform appendix. Narrow lumen bounded by mucosa with abundant lymphoid tissue.
2. Vascular Supply
Arterial
- Appendicular artery: A branch of the lower division of the ileocolic artery. It passes behind the terminal ileum to enter the mesoappendix a short distance from the base, then lies in the free border of the mesoappendix.
- An accessory appendicular artery may be present, but in most people the appendicular artery is an "end-artery" - thrombosis of which leads directly to necrosis (gangrenous appendicitis).
Venous
- Venous drainage follows the arterial supply via the ileocolic vein into the superior mesenteric vein and then into the portal system. In gangrenous appendicitis, portal pyaemia (pylephlebitis) can occur, causing septicaemia in the portal venous system and multiple intrahepatic abscesses.
Lymphatics
- Four, six or more lymphatic channels traverse the mesoappendix and empty into the ileocaecal lymph nodes.
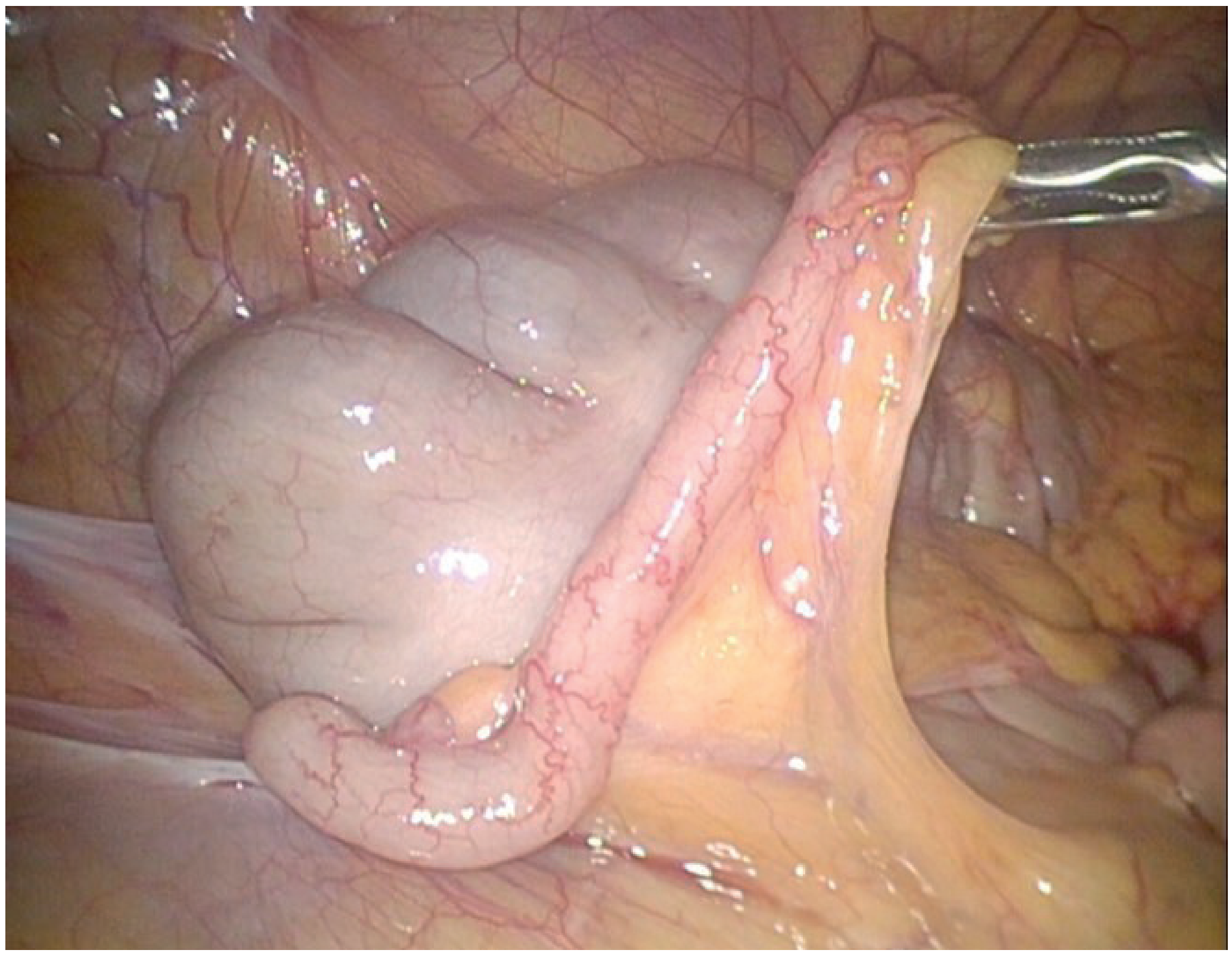
Fig 76.3 - Laparoscopic view of a normal appendix with mesoappendix displaying the appendicular artery.
3. Nerve Supply
The appendix receives its nerve supply via the superior mesenteric plexus (sympathetic, T10-L1 dermatomes). This is why the initial visceral pain of appendicitis is referred to the periumbilical region (T10). As inflammation spreads to the parietal peritoneum overlying the appendix, somatic pain shifts to the right iliac fossa (McBurney's point). The parasympathetic supply is from the vagus nerve.
4. Types / Positions of the Appendix
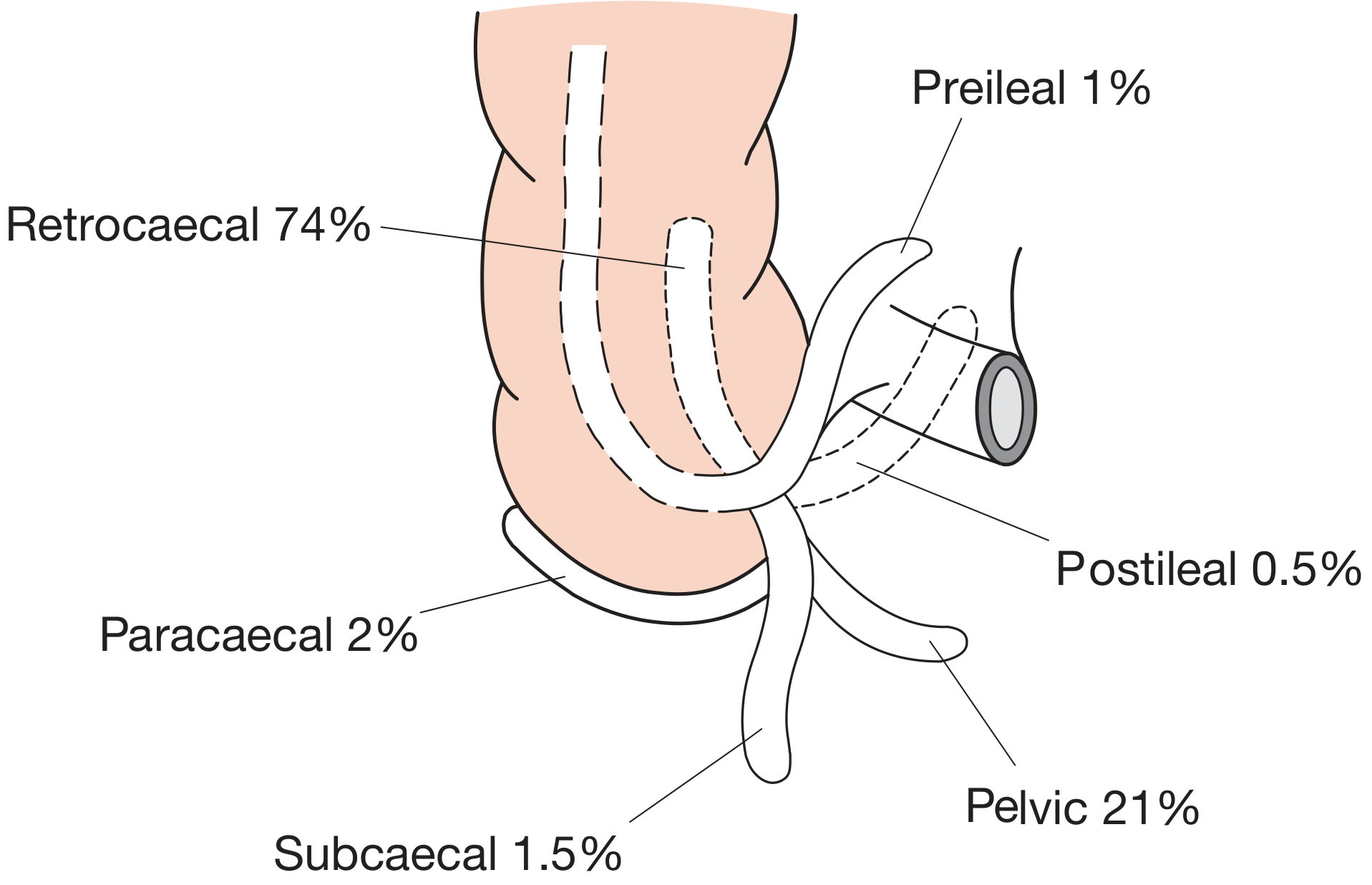
Fig 76.1 - The various positions of the appendix (after Sir C. Wakeley, London).
| Position | Frequency |
|---|---|
| Retrocaecal | 74% |
| Pelvic | 21% |
| Paracaecal | 2% |
| Subcaecal | 1.5% |
| Preileal | 1% |
| Postileal | 0.5% |
In approximately one-quarter of cases, rotation does not occur, resulting in a pelvic, subcaecal, or paracaecal position. Occasionally the tip becomes extraperitoneal, lying behind the caecum or ascending colon. Rarely, in intestinal malrotation, the appendix can be found near the gallbladder or in the left iliac fossa.
Clinical Significance of Position:
Retrocaecal appendicitis: The overlying caecum prevents contact with the anterior abdominal wall. Tenderness is present posteriorly. The psoas lies behind - hence psoas spasm and hip flexion. Rigidity may be absent. Pain may be in the loin.
Pelvic appendicitis: Abdominal tenderness may be absent. Tenderness is on rectal or vaginal examination. Urinary symptoms from proximity to the bladder and ureter. Diarrhoea can occur from irritation of the sigmoid colon.
Postileal appendicitis: May simulate small bowel obstruction. Diarrhoea may be a prominent feature.
5. Preoperative Indications & Investigations
Indications for Surgery (Appendicectomy)
- Acute appendicitis - the primary indication
- Perforated appendicitis with generalised peritonitis
- Gangrenous appendicitis
- Failure of conservative (antibiotic) management of uncomplicated appendicitis
- Appendix abscess failing to resolve on conservative management (Ochsner-Sherren regime)
- Incidental appendicectomy during other abdominal surgery (controversial)
- Tumours of the appendix (neuroendocrine tumours, mucinous neoplasms)
- Recurrent acute appendicitis after initial conservative management
- Appendix mass in pregnancy - always proceed to surgery due to fetal risk
Preoperative Investigations (Summary Box 76.5)
Routine:
- Full blood count (leukocytosis, neutrophilia)
- Urinalysis (to exclude UTI/ureteric colic as differential)
Selective:
- Ultrasound of abdomen/pelvis (>90% accuracy; better in children and thin adults; no radiation)
- Contrast-enhanced abdominal and pelvic CT scan (~95% sensitive and specific; consider low-dose protocol in young adults)
- Serum C-reactive protein, β-hCG (women of reproductive age)
- LFTs in suspected portal pyaemia
Alvarado (MANTRELS) Scoring System
| Feature | Score |
|---|---|
| Symptoms | |
| Migratory RIF pain | 1 |
| Anorexia | 1 |
| Nausea and vomiting | 1 |
| Signs | |
| Tenderness (RIF) | 2 |
| Rebound tenderness | 1 |
| Elevated temperature | 1 |
| Laboratory | |
| Leukocytosis | 2 |
| Shift to left | 1 |
| Total | 10 |
- Score ≥7: Strongly predictive of acute appendicitis → proceed to surgery
- Score 5-6: Equivocal → ultrasound or CT to reduce negative appendicectomy rate
- Score <5: Low probability
Preoperative Preparation
- IV fluids (adequate urine output; catheterisation only in the very ill)
- IV antibiotics covering Gram-negative bacilli and anaerobic cocci (e.g., metronidazole + 3rd generation cephalosporin)
- VTE risk assessment + prophylaxis (mechanical and/or pharmacological)
- Treat hyperpyrexia in children with salicylates
- Appendicectomy may be safely deferred to the next morning list (first case) in the absence of obstructive appendicitis - does not increase morbidity
6. Surgical Approaches
Open Appendicectomy
Performed under general anaesthetic, patient supine.
Gridiron (McBurney's) incision - most commonly used. Made at right angles to a line joining the anterior superior iliac spine and umbilicus, centred on McBurney's point (junction of outer one-third and inner two-thirds of the line from ASIS to umbilicus). The wound is deepened through the external oblique, internal oblique, and transversus abdominis muscles (split in the line of their fibres - "gridiron"). The peritoneum is opened, appendix delivered, and the mesoappendix divided and ligated. The appendix base is double-ligated and divided.
Lanz incision - horizontal/transverse incision within the skin crease for better cosmesis.
Rutherford-Morrison incision - extended gridiron laterally, if more access needed.
Lower midline or right paramedian - used when the diagnosis is uncertain (exploration needed) or for complicated appendicitis with generalised peritonitis.
Laparoscopic Appendicectomy
Now the preferred approach when expertise and equipment are available.
Advantages:
- Initial laparoscopy confirms diagnosis - reduces negative appendicectomy rate
- Lower wound infection rate compared to open surgery
- Quicker recovery (minimally invasive)
- Incidence of postoperative pelvic collection is not increased (contrary to initial concerns)
Technique:
- Bladder must be empty preoperatively (patient must void before leaving ward)
- Entire abdomen prepared with antiseptic
- Right iliac fossa palpated for mass before draping (if mass felt, conservative approach may be preferable)
- Three-port technique typically used
- Hook diathermy dissection of mesoappendix → appendicular artery ligated with clips and divided → appendix base ligated with absorbable ties → appendix removed in retrieval bag
In pregnancy, laparoscopic approach is now considered safe in any trimester, initiated via the open Hasson technique.
7. Postoperative Management
Routine Postoperative Care
- Early mobilisation
- Adequate analgesia; physiotherapy to reduce respiratory complications
- Discharge typically at 24-48 hours after uncomplicated appendicectomy
- Advise patient before discharge: spiking fever, malaise, and anorexia developing 5-7 days postoperatively suggests an intraperitoneal collection - seek urgent medical advice
Postoperative Complications
| Complication | Detail |
|---|---|
| Wound infection | Most common; single perioperative antibiotic dose reduces incidence significantly |
| Intra-abdominal abscess | ~8% of patients post-appendicectomy. Interloop, paracolic, pelvic or subphrenic sites. USS or CT to diagnose; percutaneous drainage preferred |
| Ileus | Expected transiently after removal of gangrenous appendix. Ileus >4-5 days + fever = investigate for intra-abdominal sepsis |
| Faecal fistula | Leakage from appendicular stump; rare |
| Richter's hernia | Through laparoscopic port site - may simulate postoperative ileus; CT definitive |
| Respiratory complications | Rare in absence of lung disease; mitigated by analgesia + physiotherapy |
| VTE | Rare; pre-/postop prophylaxis important |
| Portal pyaemia (pylephlebitis) | Rare but serious. High fever + rigors + jaundice; multiple intrahepatic abscesses. Treat with systemic antibiotics + percutaneous hepatic drainage |
8. Non-Operative (Conservative) Management
Two scenarios:
1. Uncomplicated appendicitis (no faecolith, no perforation, no abscess)
- Treatment: bowel rest + IV antibiotics (metronidazole + 3rd generation cephalosporin)
- Initial success rate ~70-80%
- ~20-30% of initially treated patients will need surgery within 1 year for recurrent symptoms
- Overall postoperative complication rate is similar between groups when compared long-term
- Consider in: well patients with limited signs, those with high operative risk (multiple comorbidities)
- Patients over 40 must be followed up to exclude underlying malignancy
2. Appendix mass (Ochsner-Sherren regime)
- Conservative strategy based on the premise that inflammation is already localised
- Inadvertent surgery on a mass is difficult and dangerous (risk of faecal fistula, inability to find appendix)
- Mark limits of mass on skin with skin pencil; serial examination
- CT abdomen + IV antibiotics
- Percutaneous drainage of any abscess if present
- Interval appendicectomy at 6-8 weeks after resolution
Criteria to STOP Conservative Treatment (Summary Box 76.6):
- Rising pulse rate
- Increasing or spreading abdominal pain
- Increasing size of the mass
9. Tumours of the Appendix
Neuroendocrine Tumours (NETs)
- Most common tumour of the appendix
- Arise from Kulchitsky (argentaffin) cells at the base of the crypts
- Most are found incidentally at appendicectomy
- Majority are <2 cm and benign behaviour
- If >2 cm: higher risk of metastasis - right hemicolectomy recommended
Epithelial Tumours
Classification (Bailey and Love Table 76.3):
| Type | Features |
|---|---|
| Low-grade appendiceal mucinous neoplasm (LAMN) | Pushing rather than infiltrative borders; mucin production |
| High-grade appendiceal mucinous neoplasm (HAMN) | High-grade cytology |
| Mucinous adenocarcinoma | Infiltrative; peritoneal spread common |
| Adenocarcinoma (colonic type) | Right hemicolectomy required |
Pseudomyxoma Peritonei
- Characteristic complication of mucinous appendiceal neoplasms
- Rupture of a mucocele or low-grade mucinous neoplasm seeds mucin-secreting cells throughout the peritoneal cavity
- Results in accumulation of gelatinous mucin in peritoneal cavity ("jelly belly")
- Treated with cytoreductive surgery (CRS) + hyperthermic intraperitoneal chemotherapy (HIPEC)
Management of Incidental or Unexpected Appendix Tumour at Surgery:
- Tumour <2 cm: appendicectomy alone is adequate
- Tumour ≥2 cm OR at appendix base OR mucinous adenocarcinoma: formal right hemicolectomy
- All cases should be referred to specialist MDT
10. Important Relations of the Appendix
| Structure | Relation |
|---|---|
| Caecum | The appendix arises from the posteromedial wall, 2 cm below the ileocaecal junction |
| Terminal ileum | Lies anterosuperiorly; appendicular artery passes behind it |
| Ileocaecal valve | Above the base of appendix |
| Psoas major | Lies posteriorly - explains hip flexion/psoas spasm in retrocaecal appendicitis |
| Ureter | Right ureter passes medially - explains urinary symptoms in pelvic appendicitis |
| Bladder/Sigmoid colon | Anteroinferior in pelvic position - causes urinary irritation/diarrhoea |
| Ovary and fallopian tube | Right adnexa - relevant differential in women (mittelschmerz, PID, ectopic) |
| Obturator internus | Obturator sign positive when pelvic appendicitis irritates the obturator muscle |
| Greater omentum | Migrates to wall off pericaecal infection - forms appendix mass |
All content sourced from Bailey and Love's Short Practice of Surgery, 28th Edition, Chapter 76 - The Appendix.
Appendix anatomy, vascular,nerve structure, preop indication, indication for surgery, post op management, types of surgery , types of appendix and tumor and other important relations refer from Bailey and love
The previous response already covered all of this in full detail from Bailey and Love's 28th Edition. Here is the complete, consolidated reference:
The Vermiform Appendix
Bailey and Love's Short Practice of Surgery, 28th Edition - Chapter 76
1. Anatomy
General
The vermiform appendix is present only in humans, certain anthropoid apes, and the wombat. It is a blind muscular tube with mucosal, submucosal, muscular, and serosal layers. Morphologically it represents the undeveloped distal end of the large caecum found in many lower animals.
At birth the appendix is short and broad at its junction with the caecum. Differential growth of the caecum produces the typical tubular structure by about age 2 years. During childhood, continued growth commonly rotates the appendix into a retrocaecal but intraperitoneal position. In approximately one-quarter of cases, rotation does not occur, resulting in a pelvic, subcaecal, or paracaecal position.
Rarely, the caecum does not migrate to its normal position in the right lower quadrant - in intestinal malrotation, the appendix can be found near the gallbladder or in the left iliac fossa, causing diagnostic difficulty.
Gross Anatomy
- Base of appendix: Constant in position - at the confluence of the three taeniae coli of the caecum, which fuse to form the outer longitudinal muscle coat of the appendix. At operation, gentle traction on the taeniae coli (especially the anterior taenia) leads the surgeon to the base of the appendix - the key surgical landmark when the appendix is elusive.
- Length: Average 7.5-10 cm
- Mesoappendix: Arises from the lower surface of the mesentery of the terminal ileum. Subject to great variation - sometimes the distal one-third of the appendix is bereft of mesoappendix. In childhood it is transparent; in many adults it becomes laden with fat, obscuring the vessels.
Microscopic Anatomy
- Lumen is irregular, encroached on by multiple longitudinal folds of mucous membrane lined by columnar cell intestinal mucosa of colonic type
- Crypts present but not numerous
- Base of crypts contains argentaffin (Kulchitsky) cells - precursors of neuroendocrine tumours (NETs)
- Submucosa contains numerous lymphatic aggregations/follicles - especially prominent in young adults; central to the aetiology of appendicitis
Fig 76.4 - Normal vermiform appendix. Narrow lumen, mucosal folds, abundant submucosal lymphoid tissue (courtesy of Dr P Kelly, FRCPath, Dublin).
2. Vascular Supply
Arterial Supply
- Appendicular artery: Branch of the lower division of the ileocolic artery (a branch of the superior mesenteric artery)
- Passes behind the terminal ileum to enter the mesoappendix a short distance from the base
- Runs in the free border of the mesoappendix
- An accessory appendicular artery may be present
- In most people, the appendicular artery is an "end-artery" - thrombosis directly causes appendicular necrosis (gangrenous appendicitis)
Venous Drainage
- Appendicular vein drains into the ileocolic vein → superior mesenteric vein → portal vein
- Gangrenous appendicitis can lead to portal pyaemia (pylephlebitis): portal septicaemia causing multiple intrahepatic abscesses, presenting with high fever, rigors, and jaundice
Lymphatics
- 4-6 or more lymphatic channels traverse the mesoappendix
- Drain into the ileocaecal lymph nodes
Fig 76.3 - Laparoscopic view of a normal appendix with mesoappendix displaying the appendicular artery.
3. Nerve Supply
| Component | Detail |
|---|---|
| Sympathetic | Via superior mesenteric plexus (T10-L1) |
| Parasympathetic | Via vagus nerve |
| Referred visceral pain | Periumbilical (T10 dermatome) - early appendicitis |
| Somatic pain shift | Shifts to RIF (McBurney's point) when parietal peritoneum is involved |
The T10 level explains the classic migratory pain pattern of appendicitis - central/periumbilical at onset, shifting to the right iliac fossa as peritoneal involvement develops.
4. Types / Positions of the Appendix
Fig 76.1 - Various positions of the appendix (after Sir C. Wakeley, London).
| Position | Frequency | Clinical Feature if Inflamed |
|---|---|---|
| Retrocaecal | 74% | Loin pain, psoas spasm, hip flexion, absent anterior rigidity |
| Pelvic | 21% | Absent abdominal tenderness; rectal/vaginal tenderness; urinary & bowel symptoms |
| Paracaecal | 2% | Classical presentation |
| Subcaecal | 1.5% | Classical presentation |
| Preileal | 1% | Small bowel-like symptoms |
| Postileal | 0.5% | Diarrhoea; may simulate bowel obstruction |
Specific Clinical Features by Position
Retrocaecal: The overlying caecum prevents contact with the anterior abdominal wall - abdominal tenderness and rigidity may be absent. The psoas muscle lies posteriorly, hence hip flexion and psoas spasm. Pain may localise to the loin. Tenderness is elicited posteriorly.
Pelvic: Abdominal tenderness may be entirely absent. Tenderness present only on rectal or vaginal examination. Urinary symptoms arise from proximity to the bladder and ureter. Diarrhoea can occur from irritation of the sigmoid colon. Easily confused with pelvic inflammatory disease in women.
Postileal: May simulate small bowel obstruction. Diarrhoea is prominent.
5. Indications for Surgery
Absolute Indications
- Acute appendicitis (confirmed or high clinical suspicion)
- Perforated appendicitis with generalised peritonitis
- Gangrenous appendicitis
- Failure of conservative (antibiotic) management of uncomplicated appendicitis
- Appendix abscess failing to resolve with Ochsner-Sherren conservative management
- Acute appendicitis in pregnancy (always operate - delay is the greatest risk to mother and fetus)
Relative Indications
- Recurrent appendicitis following initial conservative management
- Tumours of the appendix (NETs ≥2 cm, mucinous adenocarcinoma, adenocarcinoma)
- Incidental appendicectomy during other abdominal procedures (controversial)
- Patients >40 years after conservative management - interval surgery + workup to exclude malignancy
Risk Factors for Perforation (Summary Box 76.1)
- Extremes of age
- Immunosuppression
- Diabetes mellitus
- Faecolith obstruction of the lumen
- Pelvic appendix (free-lying, cannot be walled off by omentum)
- Previous abdominal surgery (limits omental migration)
6. Preoperative Investigations
Routine
- Full blood count - leukocytosis with neutrophilia
- Urinalysis - exclude UTI/renal calculus as differential
Selective
- Serum CRP - elevated in appendicitis
- β-hCG - all women of reproductive age (exclude ectopic pregnancy)
- Ultrasound abdomen/pelvis - >90% accuracy; preferred in children and thin adults; gynaecological pathology assessment; no radiation
- Contrast-enhanced CT abdomen and pelvis (~95% sensitive and specific):
- Reduces negative appendicectomy rate without increasing perforation rate
- Consider low-dose protocol in young adults (reduces radiation by up to 80%)
- Especially useful in elderly (differentiating from diverticulitis, obstruction, neoplasm)
- MRI - preferred in pregnancy (greater sensitivity than USS; no radiation)
Alvarado (MANTRELS) Score
| Feature | Score |
|---|---|
| Symptoms | |
| Migratory RIF pain | 1 |
| Anorexia | 1 |
| Nausea and vomiting | 1 |
| Signs | |
| Tenderness (RIF) | 2 |
| Rebound tenderness | 1 |
| Elevated temperature (>37.3°C) | 1 |
| Laboratory | |
| Leukocytosis | 2 |
| Shift to left (neutrophilia) | 1 |
| Total | 10 |
- ≥7: Strongly predictive → proceed to surgery
- 5-6: Equivocal → ultrasound or CT scan
- <5: Low probability → observe/investigate further
Preoperative Preparation
- IV fluids (establish adequate urine output; catheterise only the very ill)
- IV antibiotics: metronidazole + third-generation cephalosporin (cover Gram-negatives and anaerobes)
- When no purulent peritonitis: single perioperative antibiotic dose sufficient to reduce wound infection
- VTE risk assessment + mechanical and/or pharmacological prophylaxis
- Treat hyperpyrexia in children with salicylates + antibiotics + IV fluids
- In the absence of obstructive appendicitis, deferring surgery to the first morning case does not increase morbidity
7. Types of Appendicectomy Surgery
A. Open Appendicectomy
Gridiron (McBurney's) Incision (most common)
- Centred on McBurney's point (junction of outer one-third and inner two-thirds of line from ASIS to umbilicus)
- Incision made at right angles to this line
- Layers split in line of fibres: external oblique → internal oblique → transversus abdominis
- Good access for straightforward appendicectomy
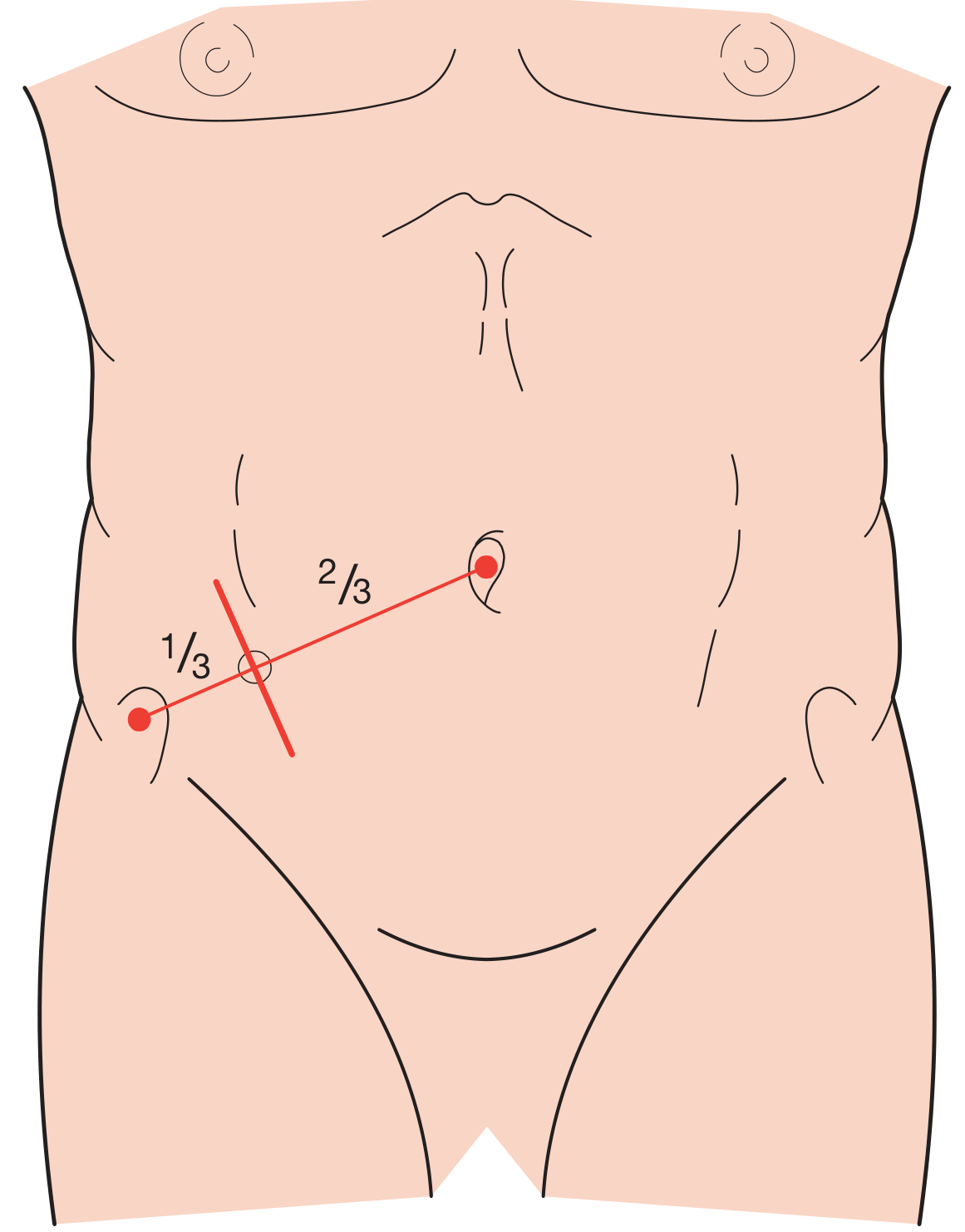
Fig 76.10 - Gridiron incision at right angles to the ASIS-umbilicus line, centred on McBurney's point.
- Lanz incision: Horizontal/transverse incision within the skin crease - better cosmesis
- Rutherford-Morrison incision: Gridiron extended laterally - greater access
- Lower midline/right paramedian: Used when diagnosis uncertain or for generalised peritonitis
Open Technique:
- Peritoneum opened; any free fluid collected for culture
- Caecum delivered into wound; taeniae coli followed to base of appendix
- Mesoappendix divided and ligated (appendicular artery secured)
- Appendix base double-ligated with absorbable suture and divided
- Stump may be invaginated (purse-string/Z-stitch) - though evidence for this is not strong
- Peritoneal lavage if peritonitis present
- Wound closed in layers
B. Laparoscopic Appendicectomy (now preferred where expertise available)
Advantages over open:
- Initial laparoscopy confirms the diagnosis - reduces negative appendicectomy rate
- Lower wound infection rate
- Quicker recovery (minimally invasive)
- Incidence of postoperative pelvic collection is not increased (contrary to initial concerns)
- Safe in any trimester of pregnancy (use open Hasson technique for entry)
Technique (three-port):
- Bladder emptied (patient voids before leaving ward)
- Entire abdomen prepared and draped
- Ports placed; laparoscopic survey performed
- Hook diathermy dissection of mesoappendix
- Appendicular artery ligated with clips and divided
- Appendix base ligated with absorbable ties
- Appendix removed in retrieval bag (prevents wound contamination)
Stump management options:
- Ligation with absorbable ties (Endoloops)
- Linear stapler division of the base
- Intracorporeal suturing
C. Non-Operative / Conservative Management
Uncomplicated Appendicitis (no faecolith/perforation/abscess)
- IV antibiotics (metronidazole + 3rd generation cephalosporin) + bowel rest
- Initial success ~70-80%
- ~20-30% will need surgery within 1 year for recurrent symptoms
- Safe option in well patients with limited signs or high operative risk
- Patients >40 years require follow-up to exclude underlying malignancy
Appendix Mass - Ochsner-Sherren Regime
Based on the premise that inflammation is already localised and inadvertent surgery risks faecal fistula or inability to find the appendix.
Protocol:
- Mark extent of mass on abdominal wall with skin pencil; serial re-examination
- CT abdomen + IV antibiotics
- Percutaneous drainage of any abscess if identified
- Interval appendicectomy at 6-8 weeks after complete resolution
Criteria to STOP Conservative Treatment and Operate (Summary Box 76.6):
- Rising pulse rate
- Increasing or spreading abdominal pain
- Increasing size of the mass
8. Postoperative Management
Routine Care
- Early mobilisation
- Adequate analgesia; physiotherapy to reduce respiratory complications
- Discharge typically 24-48 hours post uncomplicated appendicectomy
- Pre-discharge counselling: fever, malaise, anorexia developing 5-7 days post-op suggests intraperitoneal collection - seek urgent medical review
Postoperative Complications
| Complication | Incidence / Notes | Management |
|---|---|---|
| Wound infection | Most common complication | Single perioperative antibiotic dose is preventive; wound care |
| Intra-abdominal abscess | ~8% of patients | USS/CT; percutaneous drainage. Sites: interloop, paracolic, pelvic, subphrenic |
| Adynamic ileus | Expected transiently | >4-5 days + fever = investigate for intra-abdominal sepsis |
| Faecal fistula | Rare; leakage from stump | Usually settles with conservative management |
| Richter's hernia | Port site; mimics ileus | CT definitive |
| Respiratory complications | Rare without lung disease | Analgesia + physiotherapy |
| VTE | Rare | Pre/postop prophylaxis essential |
| Portal pyaemia (pylephlebitis) | Rare but life-threatening | Systemic IV antibiotics + percutaneous hepatic drainage |
9. Tumours of the Appendix
A. Neuroendocrine Tumours (NETs) - Carcinoid Tumours
(formerly called carcinoid tumours)
- Most common appendix tumour (>50% of all appendix tumours)
- Arise from Kulchitsky (argentaffin) cells at the base of the crypts
- Usually found incidentally at appendicectomy
- Occur most commonly at the tip of the appendix
- Majority are <2 cm and behave in a benign manner
| Size | Management |
|---|---|
| <2 cm | Appendicectomy alone is curative |
| ≥2 cm | Right hemicolectomy (higher risk of lymph node metastasis and distant spread) |
| At base of appendix | Right hemicolectomy regardless of size |
B. Epithelial Tumours - Classification (Table 76.3)
| Type | Key Features | Management |
|---|---|---|
| Low-grade appendiceal mucinous neoplasm (LAMN) | Pushing (not infiltrative) borders; mucin production; risk of pseudomyxoma peritonei on rupture | Appendicectomy if intact; if ruptured, CRS + HIPEC |
| High-grade appendiceal mucinous neoplasm (HAMN) | High-grade cytology; higher peritoneal risk | Right hemicolectomy + specialist MDT |
| Mucinous adenocarcinoma | Infiltrative; peritoneal spread common | Right hemicolectomy; CRS + HIPEC if peritoneal disease |
| Adenocarcinoma (colonic type) | Identical to colonic adenocarcinoma | Right hemicolectomy |
C. Pseudomyxoma Peritonei (PMP)
- Characteristic complication of ruptured appendiceal mucinous neoplasms (classically LAMN)
- Rupture seeds mucin-secreting epithelial cells throughout the peritoneal cavity
- Progressive accumulation of gelatinous mucin ("jelly belly")
- Can cause bowel obstruction, abdominal distension, malnutrition
- Treatment: Cytoreductive surgery (CRS) + hyperthermic intraperitoneal chemotherapy (HIPEC) at specialist centres
D. Management of Unexpected/Incidental Tumour at Surgery
- Tumour <2 cm: Appendicectomy alone is adequate
- Tumour ≥2 cm OR at appendix base OR mucinous adenocarcinoma: Formal right hemicolectomy
- All cases require referral to specialist multidisciplinary team (MDT)
10. Important Anatomical Relations
| Structure | Relation | Clinical Relevance |
|---|---|---|
| Caecum | Appendix arises from posteromedial wall, ~2 cm below ileocaecal valve | Taeniae coli used to locate base at surgery |
| Terminal ileum | Anterosuperior; appendicular artery passes behind it | Postileal appendicitis mimics ileal pathology |
| Ileocaecal valve | Above the base | Involved in Crohn's disease differential |
| Psoas major | Posterior (retrocaecal position) | Psoas spasm, hip flexion, pain on hip extension (psoas sign) |
| Right ureter | Medial to caecum | Urinary symptoms in pelvic appendicitis; important to identify at surgery |
| Bladder | Anteroinferior (pelvic appendix) | Urinary frequency, dysuria, pyuria mimicking UTI |
| Sigmoid colon | Left/inferior (pelvic appendix) | Diarrhoea, tenesmus |
| Right ovary + fallopian tube | Right adnexa | Differential: PID, mittelschmerz, ectopic pregnancy, ovarian torsion |
| Obturator internus | Pelvic floor (pelvic appendix) | Obturator sign: pain on passive internal rotation of flexed hip |
| Greater omentum | Migrates to wall off infection | Forms the appendix mass/phlegmon; protective against generalised peritonitis |
| Anterior superior iliac spine | Surface landmark | McBurney's point defined relative to ASIS and umbilicus |
11. Key Eponymous Signs in Appendicitis
| Sign | Mechanism |
|---|---|
| McBurney's point | Maximum tenderness at junction of outer 1/3 and inner 2/3 of ASIS-umbilicus line |
| Rovsing's sign | Pressure in LIF causes pain in RIF (parietal peritoneum irritation) |
| Psoas sign | Pain on extension of right hip (retrocaecal appendicitis, psoas irritation) |
| Obturator sign | Pain on passive internal rotation of flexed right hip (pelvic appendicitis) |
| Dunphy's sign | Increased pain on coughing (peritoneal irritation) |
| Blumberg's sign | Rebound tenderness in RIF |
All content from Bailey and Love's Short Practice of Surgery, 28th Edition, Chapter 76: The Appendix.
This is a shared conversation. Sign in to Orris to start your own chat.