

IMG_6091.png
IMG_6092.png
Teach me this
Reading File
Searching the Web
neonatal jaundice phototherapy exchange transfusion thresholds guidelines
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Now I have everything I need. Here is a full teaching session on everything in your slides:
Neonatal Jaundice - Complete Teaching Guide
What Is Neonatal Jaundice?
Jaundice (hyperbilirubinemia) in newborns is yellow discolouration caused by accumulation of unconjugated bilirubin in the skin and sclerae. The newborn liver is immature and cannot process bilirubin efficiently for the first week of life.
Why Does It Matter?
Unconjugated bilirubin is lipid soluble - it crosses the blood-brain barrier and deposits in basal ganglia/brainstem nuclei causing kernicterus (bilirubin encephalopathy = permanent brain damage). This is what you're trying to prevent.
Causes by Timing (Exam Table)
| Timing | Key Causes |
|---|---|
| < 24 hours | Always pathological - ABO/Rh haemolysis, congenital infection |
| 2-3 days | Physiological jaundice (most common) |
| 3 days - 1 week | Sepsis, UTI, G6PD deficiency, Crigler-Najjar |
| > 1 week | Breast milk jaundice, biliary atresia, hypothyroidism, metabolic |
The AMC Question: 4-Day Baby, Total Bilirubin 380, Conjugated = 12
Key reasoning chain:
- Day 4 of life
- Total bilirubin = 380 µmol/L (very high)
- Conjugated bilirubin = 12 µmol/L (low - so this is predominantly unconjugated)
- Conjugated Bil. is NOT elevated, so this is NOT biliary atresia or hepatitis
Correct answer: Phototherapy (option 2)
Why not exchange transfusion? Because the slide's second graph (below) shows that on Day 4, phototherapy threshold is 350-450 µmol/L. At 380, you START with phototherapy - exchange transfusion comes only if bilirubin keeps rising despite phototherapy, or if it exceeds the exchange transfusion threshold (~425-500+ at Day 4 for an infant at lower risk).
The Two Critical Treatment Graphs
Graph 1 - Phototherapy Thresholds
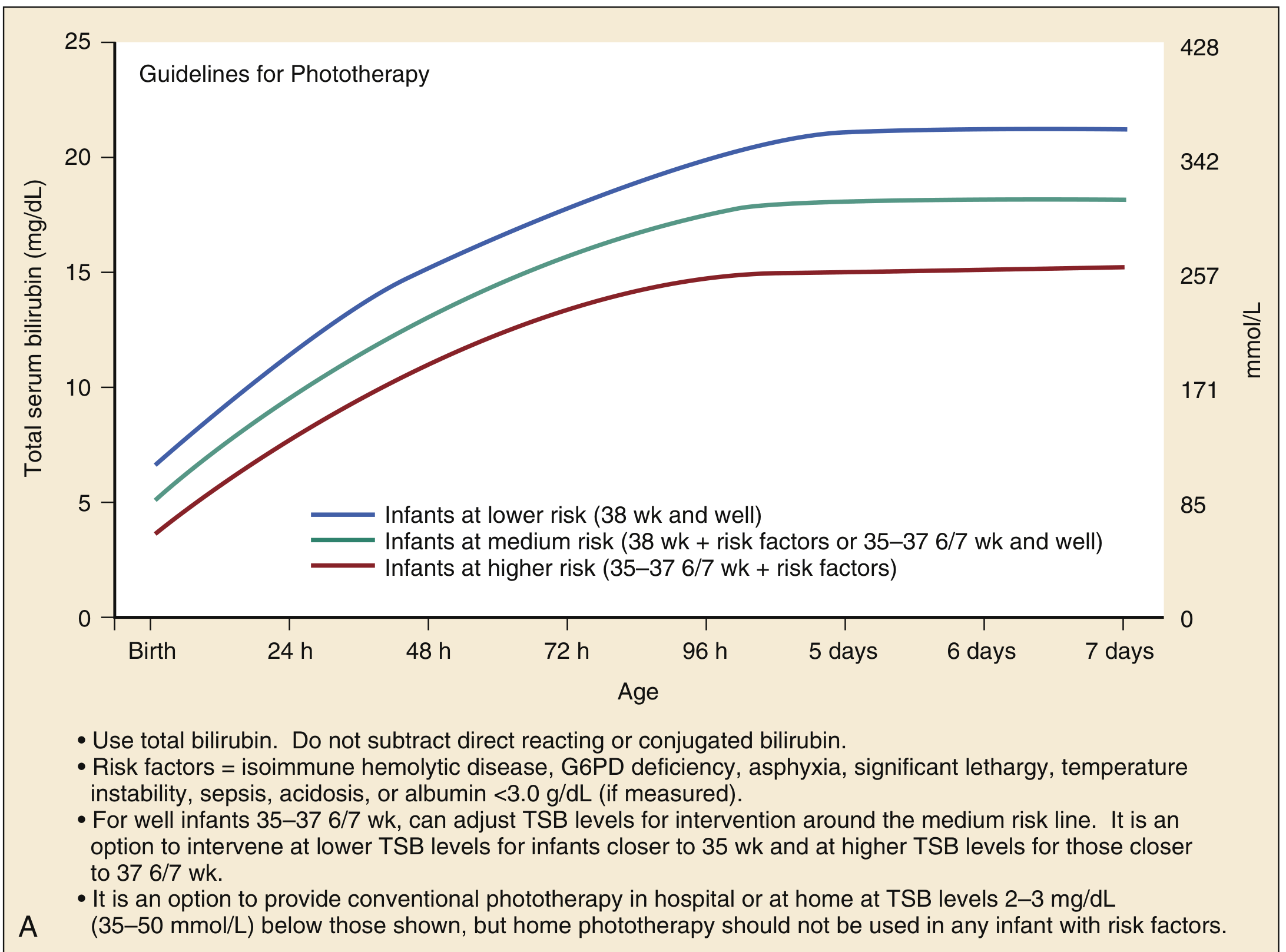
Three risk lines:
- Lower risk (blue) - 38 weeks gestation, well baby
- Medium risk (green) - 38 weeks + risk factors, OR 35-37 weeks + well
- Higher risk (red) - 35-37 weeks + risk factors
Risk factors include: isoimmune haemolytic disease, G6PD deficiency, asphyxia, lethargy, temperature instability, sepsis, acidosis, albumin < 3.0 g/dL
At Day 4 (~96 hours):
- Lower risk threshold: ~18 mg/dL (~308 µmol/L)
- Higher risk threshold: ~15 mg/dL (~257 µmol/L)
Graph 2 - Exchange Transfusion Thresholds
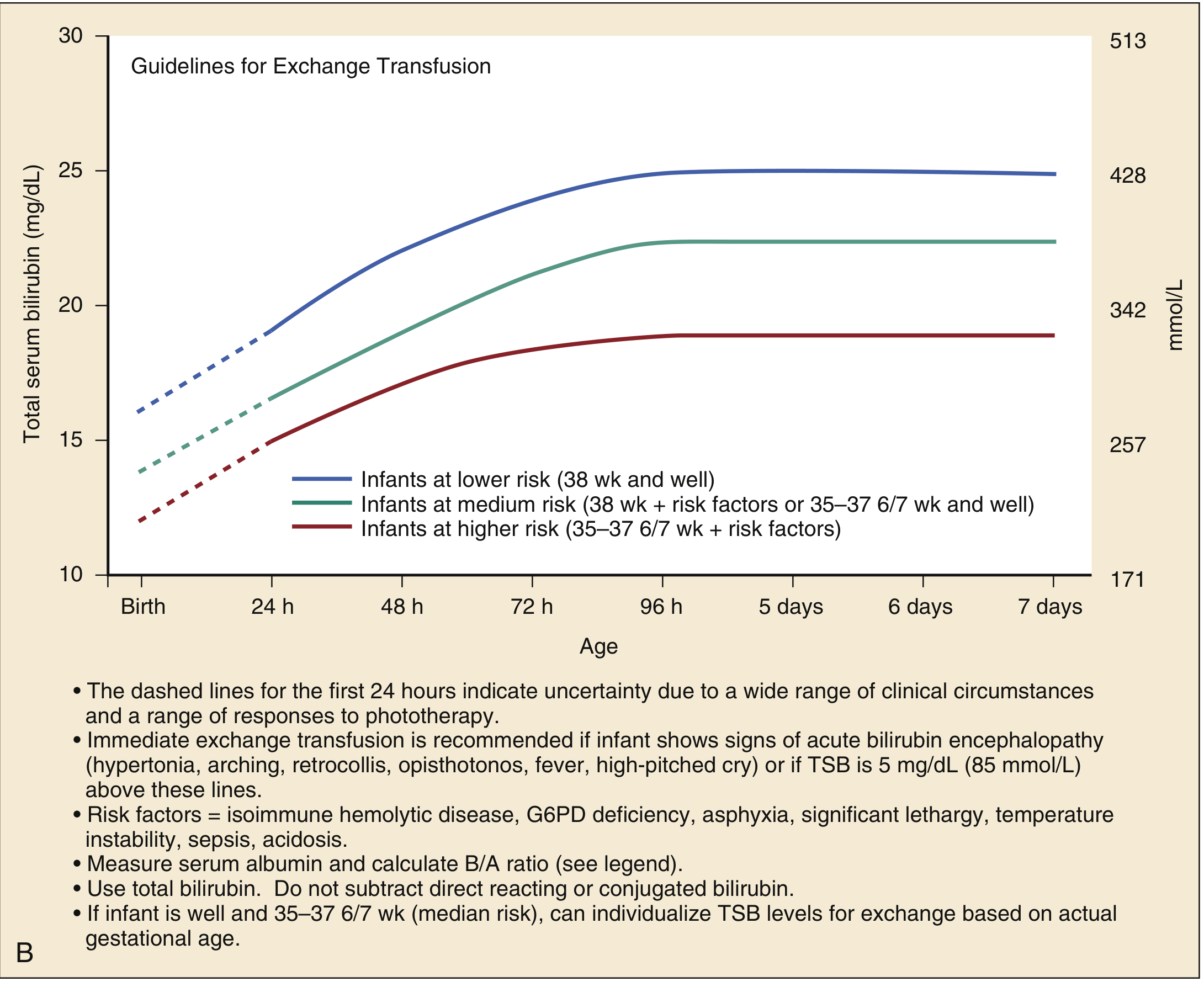
Exchange transfusion thresholds sit approximately 5 mg/dL (85 µmol/L) ABOVE the phototherapy thresholds.
Immediate exchange transfusion (don't wait) if the infant shows signs of acute bilirubin encephalopathy:
- Hypertonia
- Arching/retrocollis
- Opisthotonus
- High-pitched cry
- Fever
Treatment Decision Framework (Memory Aid)
Bilirubin Rising →
Below phototherapy line? → Monitor, feed well, follow up
Above phototherapy line? → START PHOTOTHERAPY
Rising despite phototherapy? → Consider exchange transfusion
Above exchange line OR encephalopathy signs? → EXCHANGE TRANSFUSION NOW
The slide's note: "Day 4 - phototherapy is between 350-450" means the phototherapy zone at Day 4 is approximately 350-450 µmol/L. At 380, you're within the phototherapy zone - start phototherapy, do NOT jump to exchange transfusion.
Exchange Transfusion Thresholds by Age (from your slide - for ≥35 weeks)
| Age | Higher Risk (SBR µmol/L) | Medium Risk | Lower Risk (38 wk, well) |
|---|---|---|---|
| Birth | 200 | 235 | 270 |
| 12 hrs | 230 | 255 | 295 |
| 24 hrs | 255 | 280 | 320 |
| 48 hrs | 290 | 320 | 375 |
| 72 hrs | 315 | 360 | 405 |
| 96 hrs | 320 | 380 | 425 |
| 5-7 days | 320 | 380 | 425 |
For low birthweight infants (< 1500g): thresholds are much lower (>170-255 µmol/L even at <24h).
Why Phototherapy Works
Blue light (wavelength 460-490 nm) converts unconjugated bilirubin in the skin into water-soluble isomers (lumirubin) that can be excreted in bile and urine WITHOUT needing hepatic conjugation. It's non-invasive and very effective.
Q2: 6-Year-Old Boy - Learning Difficulties + Congenital Heart Defect
Clues in the question:
- Difficulty learning since starting school (6 months ago)
- IQ = 86 (borderline low, but not severe intellectual disability)
- Adopted with unknown history
- Mild conductive hearing loss
- Flat nasal bridge
- Grade 3 holosystolic murmur on the left side of the heart (likely VSD)
Correct answer: Karyotype analysis → Down syndrome
Why Karyotype, not FMR1 DNA analysis (Fragile X)?
| Feature | Down Syndrome (Trisomy 21) | Fragile X Syndrome |
|---|---|---|
| Cause | Karyotype abnormality (extra chromosome 21) | FMR1 gene mutation (CGG repeat expansion) |
| Diagnosis | Karyotype / chromosomal microarray | FMR1 DNA analysis |
| Facial features | Flat nasal bridge, epicanthal folds, small ears, upslanting palpebral fissures | Long face, large prominent ears, prominent jaw |
| Heart defect | VSD, AVSD (very common ~40-50%) | Less commonly associated |
| Hearing loss | Conductive (common - due to chronic ear infections) | Sensorineural or conductive |
| Body build | Short, stocky | Tall, large body habitus ("everything big" as the slide notes) |
| Intellect | Mild-moderate intellectual disability | Usually moderate intellectual disability in males |
The flat nasal bridge + VSD (holosystolic murmur on left = VSD) + conductive hearing loss + unknown history = classic Down syndrome presentation. The fact the child is adopted (unknown history) means antenatal screening was never done.
Karyotype will show 47,XX or XY +21 (trisomy 21) in ~95% of Down syndrome cases. The remaining ~5% are translocation or mosaic types - all detectable by karyotype.
Summary - What To Remember for AMC
| Scenario | Answer |
|---|---|
| Day 4, Total Bil. 380 µmol/L, Conj. Bil. 12 | Phototherapy |
| Bilirubin not responding to phototherapy | Exchange transfusion |
| Baby with acute encephalopathy signs (opisthotonus, high-pitched cry) | Immediate exchange transfusion |
| Child with flat nasal bridge, VSD, conductive hearing loss, learning difficulties | Karyotype (Down syndrome) |
| Child with large ears, large body, learning difficulties (male) | FMR1 DNA analysis (Fragile X) |
| Jaundice in first 24 hours | Always pathological - think haemolysis |
| Conjugated bilirubin elevated | Always pathological - think biliary atresia |
The core principle running through all neonatal jaundice management is: escalate based on bilirubin level + gestational age + risk factors, with phototherapy as the first-line step and exchange transfusion reserved for failure or severe cases. For the genetics question, the physical exam clues (flat nasal bridge, VSD) point you directly toward Down syndrome and karyotyping.
This is a shared conversation. Sign in to Orris to start your own chat.