What is the clinical significance of elevated LDL cholesterol.
Reading File
Finding Sources
Searching PubMed
"LDL cholesterol" AND "cardiovascular risk"
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Here is a thorough answer synthesized from authoritative medical textbooks and current evidence.
Clinical Significance of Elevated LDL Cholesterol
1. LDL as a Causal Agent for Atherosclerosis
Elevated LDL-C is an established causal agent for atherosclerosis, not merely an association. The positive correlation between plasma LDL concentration and atherosclerosis incidence is one of the most well-replicated findings in medicine. When LDL receptors are defective (as in familial hypercholesterolemia), LDL is not cleared from the blood, leading to accelerated plaque deposition - Harper's Illustrated Biochemistry, 32nd Ed.
Hypercholesterolemia is most often due to elevated LDL-C, which is an established causal agent for atherosclerosis. - Fuster and Hurst's The Heart, 15th Edition
2. The Atherogenic Mechanism
The diagram below illustrates how LDL drives atherosclerotic plaque formation:
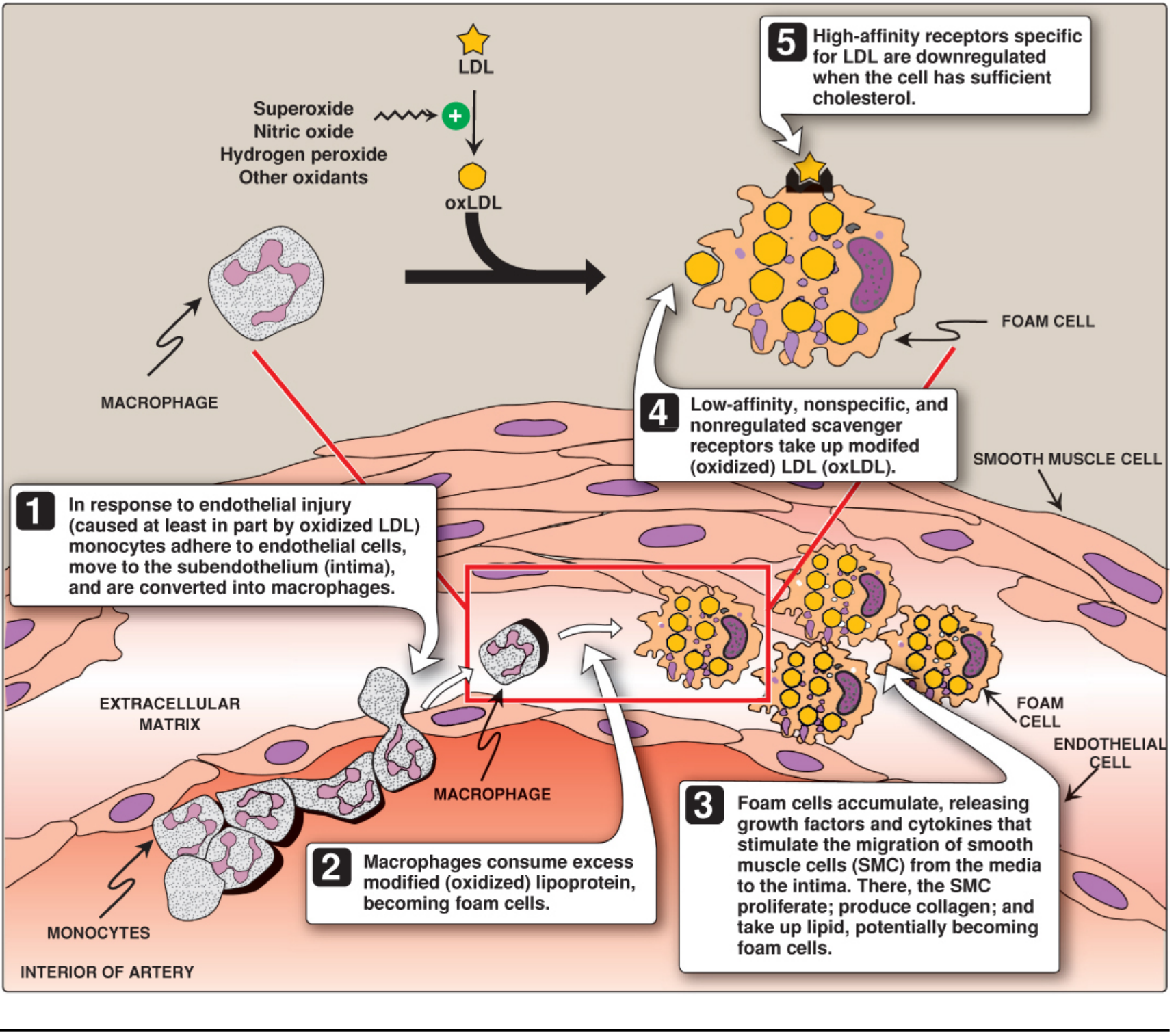
The sequence of events:
- LDL enters the arterial intima and is oxidized (oxLDL) by reactive oxygen species (superoxide, hydrogen peroxide, nitric oxide).
- oxLDL causes endothelial injury, triggering monocyte adhesion and migration into the subendothelium, where they become macrophages.
- Macrophages ingest modified LDL via low-affinity, nonregulated scavenger receptors (unlike the regulated LDL receptor, these are not downregulated when cholesterol is sufficient), becoming lipid-laden foam cells.
- Foam cells accumulate and release growth factors and cytokines, recruiting smooth muscle cells (SMCs) from the media into the intima, where they proliferate and produce collagen - forming the fibrous cap.
- The lipid/necrotic core builds up as normal phagocytic processes are overwhelmed, forming a vulnerable plaque prone to rupture or erosion.
- Goldman-Cecil Medicine, 2-Volume Set and Lippincott's Biochemistry, 8th Ed
3. Small, Dense LDL - An Independent Risk Factor
Not all LDL is equal. Small, dense LDL particles are particularly atherogenic:
- They are more susceptible to oxidation.
- They penetrate the vascular wall more readily.
- They upregulate endothelial adhesion molecules (ICAM-1, VCAM-1) and MCP-1.
- They activate macrophages via TLR-4 and the NF-κB inflammatory pathway.
The Atherosclerosis Risk in Communities (ARIC) study prospectively showed that small, dense LDL levels independently predict incident coronary heart disease, even when overall LDL-C is not markedly elevated. - Fuster and Hurst's The Heart, 15th Edition
4. Cardiovascular Risk by LDL Level
| LDL-C Level | Clinical Implication |
|---|---|
| < 100 mg/dL | Optimal |
| 100-129 mg/dL | Near optimal |
| 130-159 mg/dL | Borderline high |
| 160-189 mg/dL | High - evaluate for secondary causes |
| ≥ 190 mg/dL | Very high - likely genetic; 5-fold higher lifetime ASCVD risk |
| FH (untreated) | 20-fold higher lifetime ASCVD risk |
- Goldman-Cecil Medicine
5. Genetic Conditions: Familial Hypercholesterolemia (FH)
- Heterozygous FH affects ~1 in 250 persons worldwide. Caused by loss-of-function mutations in the LDLR gene (most common), PCSK9 gain-of-function mutations, or altered Apo B binding site mutations.
- Heterozygous FH causes premature coronary artery disease in men in their 30s-40s and women in their 40s-50s.
- Homozygous FH (1 in 500,000) manifests with ASCVD events in childhood and myocardial infarction by age 20.
- Goldman-Cecil Medicine and Robbins & Kumar Basic Pathology
6. Quantifying the Benefit of LDL Reduction
Each 39 mg/dL (1 mmol/L) reduction in LDL-C is associated with a 22% reduction in cardiovascular events. This linear, dose-dependent relationship is the strongest argument for treating elevated LDL aggressively. - Goldman-Cecil Medicine
A 2024 meta-analysis of 60 RCTs (PMID: 39126771) confirmed this time-dependent benefit: the cardiovascular risk reduction from LDL lowering accumulates progressively over time, reinforcing early and sustained treatment.
7. Indications for Treatment (2018 AHA/ACC Guideline)
Four groups qualify for high-intensity statin therapy (targeting ≥50% LDL-C reduction):
- Established clinical ASCVD
- LDL-C > 190 mg/dL
- Diabetes mellitus aged 40-75 years with high-risk features
- 10-year ASCVD risk ≥ 7.5% (with risk-enhancing factors)
8. Treatment Hierarchy
| Agent | Mechanism | LDL Reduction |
|---|---|---|
| High-intensity statins | Inhibit HMG-CoA reductase → upregulate hepatic LDL receptors | 40-60% |
| Ezetimibe | Inhibits intestinal cholesterol absorption | Additional ~15-20% |
| PCSK9 inhibitors (evolocumab, alirocumab) | Block PCSK9-mediated LDL receptor degradation | Additional 50-60% on top of statin |
| Bile acid sequestrants | Interrupt enterohepatic circulation | 15-25% |
Plaque regression - not just stabilization - is possible with dramatic LDL reduction: decreased subendothelial LDL retention allows normal phagocytic and inflammation-resolving mechanisms to heal the plaque, reducing foam cell formation, and restoring macrophage efferocytosis. - Goldman-Cecil Medicine
Summary: Elevated LDL-C is a direct, causal driver of atherosclerosis via oxidation, endothelial injury, foam cell formation, and plaque growth. The risk is graded and continuous, with LDL > 190 mg/dL carrying a 5-fold (and FH a 20-fold) lifetime ASCVD risk. Each 1 mmol/L reduction in LDL reduces cardiovascular events by ~22%, making LDL the primary target of lipid-lowering therapy.
Exam oriented, ready to write
Asking for Preferences
Here is a high-yield, exam-ready structured answer on the clinical significance of elevated LDL cholesterol, formatted for quick writing and recall.
Clinical Significance of Elevated LDL Cholesterol
Definition & Normal Values
| Category | LDL-C (mg/dL) |
|---|---|
| Optimal | < 100 |
| Near optimal | 100 - 129 |
| Borderline high | 130 - 159 |
| High | 160 - 189 |
| Very high | ≥ 190 |
Pathophysiology (Write This as a Flow)
Elevated LDL → Oxidation (oxLDL) → Endothelial injury → Monocyte recruitment → Macrophage foam cell formation → Fatty streak → Fibrous plaque → Vulnerable plaque → Rupture → Thrombus → ACS/Stroke
Key steps to remember:
- oxLDL is taken up by macrophages via scavenger receptors (non-regulated - do NOT switch off)
- Normal LDL receptors downregulate when cell has enough cholesterol - scavenger receptors do NOT
- Foam cells release cytokines → recruit smooth muscle cells → produce collagen (fibrous cap)
- Small, dense LDL is more atherogenic than large LDL (more easily oxidized, penetrates wall more)
Clinical Consequences of Elevated LDL
| Organ | Consequence |
|---|---|
| Coronary arteries | CAD, Stable angina, MI |
| Cerebral arteries | Ischemic stroke, TIA |
| Peripheral arteries | PAD, claudication |
| Aorta | Aortic atherosclerosis, aneurysm |
| Renal arteries | Renovascular hypertension |
Genetic Condition: Familial Hypercholesterolemia (FH) (High-Yield)
| Feature | Heterozygous FH | Homozygous FH |
|---|---|---|
| Prevalence | 1 in 250 | 1 in 500,000 |
| LDL-C | > 190 mg/dL | > 400-500 mg/dL |
| Defect | Loss-of-function LDLR mutation | Both LDLR alleles affected |
| Other mutations | PCSK9 gain-of-function, Apo B mutation | Same |
| CAD onset (men) | 30s - 40s | Childhood |
| CAD onset (women) | 40s - 50s | Childhood |
| ASCVD risk | 20-fold higher (lifetime) | Severe - MI by age 20 |
| Clinical signs | Tendon xanthomas, xanthelasma, corneal arcus | Same + more severe |
Exam trap: In FH, LDL receptor is defective → hepatic LDL uptake reduced → blood LDL rises despite normal dietary intake.
Risk Quantification (Must-Know Numbers)
- LDL > 190 mg/dL → 5-fold higher lifetime ASCVD risk
- FH (untreated) → 20-fold higher lifetime ASCVD risk
- Every 39 mg/dL (1 mmol/L) reduction in LDL-C = 22% reduction in cardiovascular events
- Statin benefit is proportional to absolute LDL reduction
Treatment Ladder (Write in Order)
1. Lifestyle - Diet (reduce saturated fat, trans fats), exercise, weight loss
2. High-intensity statins (first-line pharmacotherapy)
- Mechanism: Inhibit HMG-CoA reductase → less hepatic cholesterol → upregulate LDL receptors → more LDL cleared from blood
- Reduce LDL by 40-60%
- Drugs: Rosuvastatin 20-40 mg, Atorvastatin 40-80 mg
3. Ezetimibe (add-on to statin)
- Inhibits NPC1L1 in intestinal brush border → blocks cholesterol absorption
- Additional ~15-20% LDL reduction
4. PCSK9 inhibitors (evolocumab, alirocumab)
- Block PCSK9 → prevent LDL receptor degradation → more receptors on hepatocytes → more LDL cleared
- Additional 50-60% LDL reduction on top of statin
- Used in FH, very high-risk patients, statin intolerance
5. Bile acid sequestrants (cholestyramine, colesevelam)
- Interrupt enterohepatic bile acid recirculation → liver uses cholesterol to make more bile acids
- 15-25% reduction; contraindicated when TG > 300 mg/dL (can worsen hypertriglyceridemia)
AHA/ACC 2018 Guideline: 4 Groups for High-Intensity Statin
- Clinical ASCVD (prior MI, stroke, PAD)
- LDL-C ≥ 190 mg/dL
- Diabetes mellitus, age 40-75 years
- 10-year ASCVD risk ≥ 7.5% (calculated by Pooled Cohort Equations)
Secondary Causes of Elevated LDL (Always Exclude First)
| Cause | Notes |
|---|---|
| Hypothyroidism | Most common secondary cause to test for |
| Nephrotic syndrome | Hepatic lipoprotein overproduction |
| Diabetes mellitus | Often raises TG + LDL |
| Obesity | Raises LDL, lowers HDL |
| Glucocorticoids | Raise LDL |
| Obstructive liver disease | Impaired bile excretion |
| Anorexia nervosa | Reduced LDL clearance |
Rule: Any LDL ≥ 160 mg/dL or TG ≥ 500 mg/dL → first rule out secondary causes before labeling primary.
One-Line Exam Answers
- Why does FH cause CAD early? - Loss of LDL receptors → no hepatic clearance → circulating LDL oxidizes and deposits in arteries
- Why are scavenger receptors dangerous? - They are not downregulated by intracellular cholesterol → unlimited foam cell formation
- Why can statins regress plaques? - Dramatic LDL reduction allows normal macrophage efferocytosis to clear necrotic debris and resolve inflammation
- Most atherogenic LDL subtype? - Small, dense LDL (sdLDL) - more oxidizable, penetrates endothelium more easily
- LDL reduction target in very high-risk patients? - < 55 mg/dL (European guidelines) or < 70 mg/dL (US guidelines) with ≥50% reduction
Memory hook for PCSK9: PCSK9 = "Protein that Chews up Statin-Cleared Kinase 9" - it destroys LDL receptors. Blocking it = more receptors = lower LDL.
This is a shared conversation. Sign in to Orris to start your own chat.