Im orthopedic hod. Done i would I like to know the recent treatment ozone for orthopedic n musculoskeletal problem fellowship in ozone therapy
ozone therapy musculoskeletal orthopedic treatment
ozone therapy fellowship training orthopedics 2024 2025 2026 India worldwide
ozone therapy orthopedics musculoskeletal recent advances 2025 disc herniation knee osteoarthritis
ozone therapy intervertebral disc herniation low back pain
ozone therapy fellowship certificate course India IOF ISCO3 WFOT 2025 2026
http://www.ozoneforumofindia.com
PMID: 38905033
Ozone Therapy in Orthopedics & Musculoskeletal Medicine - 2025/2026 Update
Mechanism of Action
- Oxidative preconditioning - triggers upregulation of Nrf2 pathway, antioxidant enzymes (superoxide dismutase, catalase, glutathione peroxidase)
- Anti-inflammatory effect - suppresses pro-inflammatory cytokines (IL-1β, TNF-α), reduces PGE2
- Analgesic effect - inhibits bradykinin synthesis, stimulates endorphin release
- Tissue repair - promotes neovascularization, fibroblast proliferation, collagen synthesis
- Proteolysis - in disc herniation: oxidizes nucleus pulposus proteoglycans, causing disc shrinkage and reducing nerve root compression
Orthopedic Indications with Current Evidence
1. Lumbar Disc Herniation / Radiculopathy (STRONGEST EVIDENCE)
- Intradiscal ozone injections at ≥6 months had OR = 3.95 (95% CI 2.44-6.39) superior treatment success vs. steroid injections
- VAS reduction comparable to microdiscectomy at 18 months (SMD = -0.05, non-inferior)
- Superior to conventional medications at both 6 and 12 months
- Route: Intradiscal + paravertebral/foraminal injection, O3 concentration 20-40 mcg/mL
2. Knee Osteoarthritis
3. Subacromial Impingement Syndrome / Shoulder
4. Tendinopathies
- Supraspinatus/rotator cuff calcific tendinitis - comparable to corticosteroids
- Plantar fasciitis - ozone injections match corticosteroids in pain relief
- Chronic supraspinatus tendinopathy - demonstrated superiority over mesotherapy
5. Other Orthopedic Applications
| Condition | Route | Evidence Level |
|---|---|---|
| Cervical disc disease | Paravertebral/foraminal | RCTs |
| Lumbar spinal stenosis | Epidural/paravertebral | RCT (Parvin 2024: superior to steroids at 8 weeks) |
| Osteonecrosis of femoral head | Intra-articular + IV AHT | Case series, preliminary studies |
| Chronic osteomyelitis | Local infiltration + topical | Case reports, series |
| Fracture healing | Topical + local | Animal models; clinical case reports |
| Chronic wound/diabetic foot | Topical (ozonated oil/water, gas bag) | Systematic reviews |
| Fibromyalgia/myofascial pain | Autohemotherapy (AHT) | RCTs |
| Carpal tunnel syndrome | Local infiltration | Clinical studies |
| Temporomandibular joint | Intra-articular | Clinical series |
Routes of Administration in Orthopedics
- Intra-articular injection - knee, shoulder, hip
- Intradiscal injection - under fluoroscopy/CT guidance
- Paravertebral/foraminal injection - lumbar/cervical
- Epidural - for spinal stenosis, radiculopathy
- Intramuscular (trigger point) - myofascial pain
- Minor/Major Autohemotherapy (AHT) - systemic inflammatory conditions
- Topical - ozonated oil, ozonated water (wound care)
Safety Profile
- No systemic toxicity at therapeutic doses
- No cartilage damage (unlike corticosteroids with repeated use)
- No tendon weakening
- Main risks: improper technique (embolism if IV; pneumothorax if paravertebral poorly guided), use of non-medical grade ozone generators
Fellowship & Training in Ozone Therapy
India - Ozone Forum of India (OFI)
- Conducts regular Training Programmes (131st programme completed Mumbai, April 2026)
- Annual conferences (2025 conference held in Mumbai)
- Published the 2nd edition of their textbook (July 2025)
- Certificate-based training for doctors
- Contact: ozoneforumofindia.com | Based in Mumbai
International Bodies
| Organization | What They Offer |
|---|---|
| ISCO3 (International Scientific Committee of Ozone Therapy) | Sets global training standards; curriculum for Orthopedics/Traumatology specialization module (~25 hrs classroom + 75 hrs distance); isco3.org |
| WFOT (World Federation of Ozone Therapy) | Founded in New Delhi (2005); promotes global ozone therapy training and credentialing |
| AEPROMO (Spain) | Fellowship/expert certification in ozone therapy; internationally recognized |
| Journal of Ozone Therapy (JO3T) | Peer-reviewed open-access journal for keeping updated |
ISCO3 Orthopaedics & Traumatology Specialization Module Covers:
- Cervical spine: examination + ozone infiltration technique
- Lumbar spine: intramuscular, facet joint, paravertebral, intradiscal approaches
- Peripheral joints: intra-articular injection technique
- Mechanism of ozone action in spine
- Imaging guidance (fluoroscopy, US)
Steps to Pursue Fellowship
- Complete a basic ozone therapy course - OFI training (India) or ISCO3-affiliated centre
- Advanced specialization - ISCO3 Orthopedics module or AEPROMO Spain program
- Credentialing - Certificate from WFOT or ISCO3-recognized body
- Hands-on supervised practice - Under an experienced ozone therapist
- Keep updated - Subscribe to Journal of Ozone Therapy and Ozone Therapy Global Journal
Key Takeaways for Your Practice
- Ozone therapy is not experimental for orthopedic indications - level 1 evidence now exists for disc herniation and knee OA
- It is a strong alternative or adjunct to corticosteroids with a safer long-term profile
- Results for disc herniation are non-inferior to microdiscectomy in selected patients (mild-moderate herniation without severe neurological deficits)
- Imaging guidance (ultrasound or fluoroscopy) is recommended for intra-articular and spinal injections
- Regulatory status varies by country - in India, OFI and WFOT-recognized training is the pathway
Generate a comparison chart: ozone vs. corticosteroids vs. surgery for common indications
A professional medical comparison chart for orthopedic surgeons titled "Ozone Therapy vs. Corticosteroids vs. Surgery: Orthopedic Indications". The chart is a detailed table with 4 columns: Indication, Ozone Therapy, Corticosteroids, Surgery. Rows cover: 1) Lumbar Disc Herniation, 2) Knee Osteoarthritis, 3) Subacromial Impingement, 4) Plantar Fasciitis, 5) Spinal Stenosis, 6) Tendinopathy. Each cell has brief bullet points on efficacy, duration of relief, side effects, and repeat dosing. Color coding: green column for Ozone, orange for Corticosteroids, blue for Surgery. Clean clinical white background, bold headers, medical infographic style, suitable for a hospital HOD presentation.
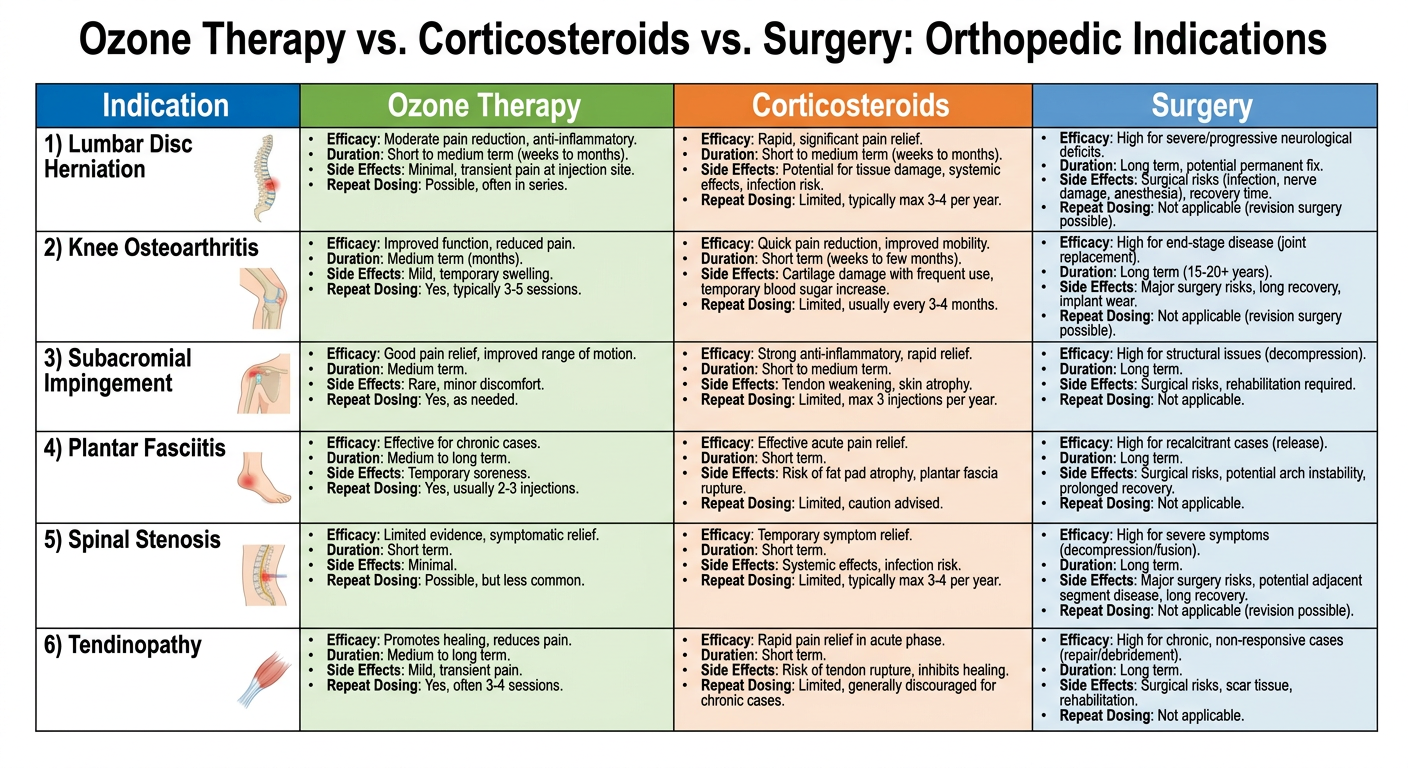
Ozone Therapy vs. Corticosteroids vs. Surgery - Orthopedic Comparison
| Indication | Ozone Therapy | Corticosteroids | Surgery |
|---|---|---|---|
| Lumbar Disc Herniation | ✅ Non-inferior to microdiscectomy at 18 months; OR 3.95 vs steroids at 6 months; intradiscal + foraminal route; 4-6 sessions | ⚠️ Short-term relief only (4-8 weeks); risk of disc degeneration with repeat; epidural/foraminal | ✅ Fastest for severe neurological deficit; microdiscectomy 85-90% success; invasive, GA, recovery 4-6 wks |
| Knee Osteoarthritis | ✅ Comparable to HA and corticosteroids; no cartilage toxicity; repeat courses safe; intra-articular; 3-5 sessions | ⚠️ Effective short-term; max 3-4 injections/year; chondrotoxicity risk with frequent use | ⚠️ TKR for end-stage only; irreversible; excellent for Gr III-IV; not suitable for younger patients |
| Subacromial Impingement | ✅ Multiple doses superior to single dose; comparable to steroids at 1 year; no tendon weakening | ⚠️ Rapid relief; risk of tendon rupture with repeated injection; max 2-3/year | ⚠️ Arthroscopic subacromial decompression if conservative fails; generally reserved for 6+ months failure |
| Plantar Fasciitis | ✅ Comparable to corticosteroids; longer-lasting; no fat pad atrophy; 3-4 sessions | ⚠️ Effective; risk of plantar fascia rupture and fat pad atrophy with repeat use | ⚠️ Fasciotomy last resort; risk of arch collapse; rarely needed (<5% cases) |
| Lumbar Spinal Stenosis | ✅ RCT 2024: superior to steroids at 8 weeks; paravertebral + epidural route | ⚠️ Epidural steroid - moderate relief; limited duration; not disease-modifying | ✅ Laminectomy/decompression for severe claudication/neurological deficit; definitive |
| Rotator Cuff Tendinopathy | ✅ Superior to mesotherapy; comparable to corticosteroids; promotes tendon healing, not degeneration | ⚠️ Rapid relief; repeat injections weaken collagen; risk of tendon rupture | ⚠️ Tendon repair for full-thickness tears; not indicated for tendinopathy alone |
| Myofascial / Trigger Points | ✅ IM ozone effective; reduces hyperalgesia; can be repeated safely | ⚠️ Triamcinolone injections; atrophy risk with repeat | ❌ Not applicable |
| Osteomyelitis (chronic) | ✅ Local ozone + systemic AHT - adjunct to antibiotics; promotes granulation, antibacterial | ❌ Not applicable | ✅ Debridement essential; ozone useful as adjunct post-debridement |
Summary - When to Choose What
| Factor | Ozone | Corticosteroids | Surgery |
|---|---|---|---|
| Onset of relief | 1-3 weeks | Days | Immediate (post-recovery) |
| Duration of benefit | 6-18 months | 4-12 weeks | Long-term / permanent |
| Repeat safety | ✅ High - no tissue toxicity | ⚠️ Limited (3-4/year max) | ❌ Not repeatable |
| Disease modification | Partial (anti-inflammatory, regenerative) | ❌ None | ✅ Yes (structural) |
| Neurological deficit | ❌ Not for severe acute deficits | ❌ Temporizing only | ✅ First choice |
| Cost | Low-moderate | Low | High |
| Invasiveness | Minimally invasive | Minimally invasive | Invasive |
| Cartilage safety | ✅ Safe, possibly chondroprotective | ⚠️ Chondrotoxic in excess | Depends on procedure |
- Mild-moderate disc herniation / OA / tendinopathy without neurological deficit → Try ozone first (or alongside rehab)
- Acute severe inflammation / need for rapid relief → Corticosteroid (short course, not repeated)
- Severe neurological deficit, instability, end-stage OA, full-thickness tear → Surgery
- Post-surgical / chronic wound / osteomyelitis adjunct → Ozone as complementary therapy