Acute onset painless vision loss detailed information
Reading File
Finding Sources
Finding Sources
Searching PubMed
"acute vision loss" painless causes
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive data from multiple authoritative sources. Let me compile the detailed answer.
Acute Onset Painless Vision Loss - Detailed Overview
Classification Framework
The first step in evaluating acute painless vision loss is determining whether it is monocular or binocular, and whether it is transient (< 24 hours) or persistent. This classification narrows the differential dramatically.
The Wills Eye Manual provides the following framework:
| Monocular - Persistent | Monocular - Transient | Binocular | |
|---|---|---|---|
| Painless | CRAO, CRVO, Ischemic optic neuropathy, GCA, Vitreous hemorrhage, Retinal detachment | Amaurosis fugax, Optic disc drusen, Impending CRVO, Ocular ischemic syndrome, Orthostatic hypotension | Occipital stroke (homonymous hemianopsia), Vertebrobasilar insufficiency, Papilledema, Pituitary apoplexy |
Causes - Monocular Persistent
1. Central Retinal Artery Occlusion (CRAO)
Presentation: Unilateral, painless, acute vision loss (counting fingers to light perception in 94% of eyes) occurring over seconds. A history of transient visual loss (amaurosis fugax) may precede it.
Fundoscopic signs:
- Superficial opacification/whitening of the retina in the posterior pole
- Cherry-red spot at the center of the macula (pathognomonic)
- Marked relative afferent pupillary defect (RAPD)
- Narrowed retinal arterioles; "boxcarring" or segmentation of the blood column
- Occasionally visible retinal arteriolar emboli (Hollenhorst plaques - refractile, yellow, at vessel bifurcations)

Etiology:
- Emboli - Cholesterol (Hollenhorst plaque, from ulcerated carotid atheromas), Calcium (from cardiac valves), Platelet-fibrin (from carotid atheromas)
- Thrombosis
- Giant Cell Arteritis (GCA) - can also cause BRAO, ophthalmic artery occlusion, or ischemic optic neuropathy
- Hypercoagulable states - antiphospholipid syndrome, factor V Leiden, protein C/S deficiency, hyperhomocysteinemia, polycythemia, multiple myeloma
- Collagen vascular disease - SLE, polyarteritis nodosa
- Rare - migraine, Behçet disease, syphilis, sickle cell disease
- Trauma
Risk factors: Age 50-70 years, hypertension, hyperlipidemia, diabetes, cardiac valvular disease, sickle cell disease, increased orbital pressure (acute glaucoma, retrobulbar hemorrhage)
Workup:
- Treat as acute stroke - immediate ER referral, preferably to a stroke center (AAO 2018 guidelines)
- ESR, CRP, platelets (if ≥55 years, to rule out GCA)
- Blood pressure, fasting glucose/HbA1c, CBC, PT/PTT, lipid profile
- Carotid Doppler ultrasound
- Cardiac evaluation: ECG, echocardiography, Holter monitoring
- OCT, IVFA; consider hypercoagulability workup in patients <50 years
Treatment:
- Poor prognosis - spontaneous resolution in only 1-8% of cases
- If GCA suspected: high-dose systemic steroids immediately
- For ocular signs (only if within 90-120 minutes of onset, none proven in RCTs):
- Ocular massage (digital or fundus contact lens)
- Anterior chamber paracentesis
- IOP reduction with acetazolamide 500 mg IV or topical beta-blocker (timolol 0.5%)
- Follow-up: Check for neovascularization of iris/disc/retina at 1-4 weeks (develops in ~20% at mean 4 weeks); treat with PRP and/or anti-VEGF if present
2. Branch Retinal Artery Occlusion (BRAO)
Presentation: Unilateral, painless, abrupt partial visual field loss; may have prior amaurosis fugax.
Signs: Superficial retinal whitening/opacification along the distribution of the affected branch retinal artery. Narrowed arterioles, boxcarring. Cholesterol emboli (Hollenhorst plaques) may be visible at vessel bifurcations.
Etiology: Same as CRAO (emboli most common).
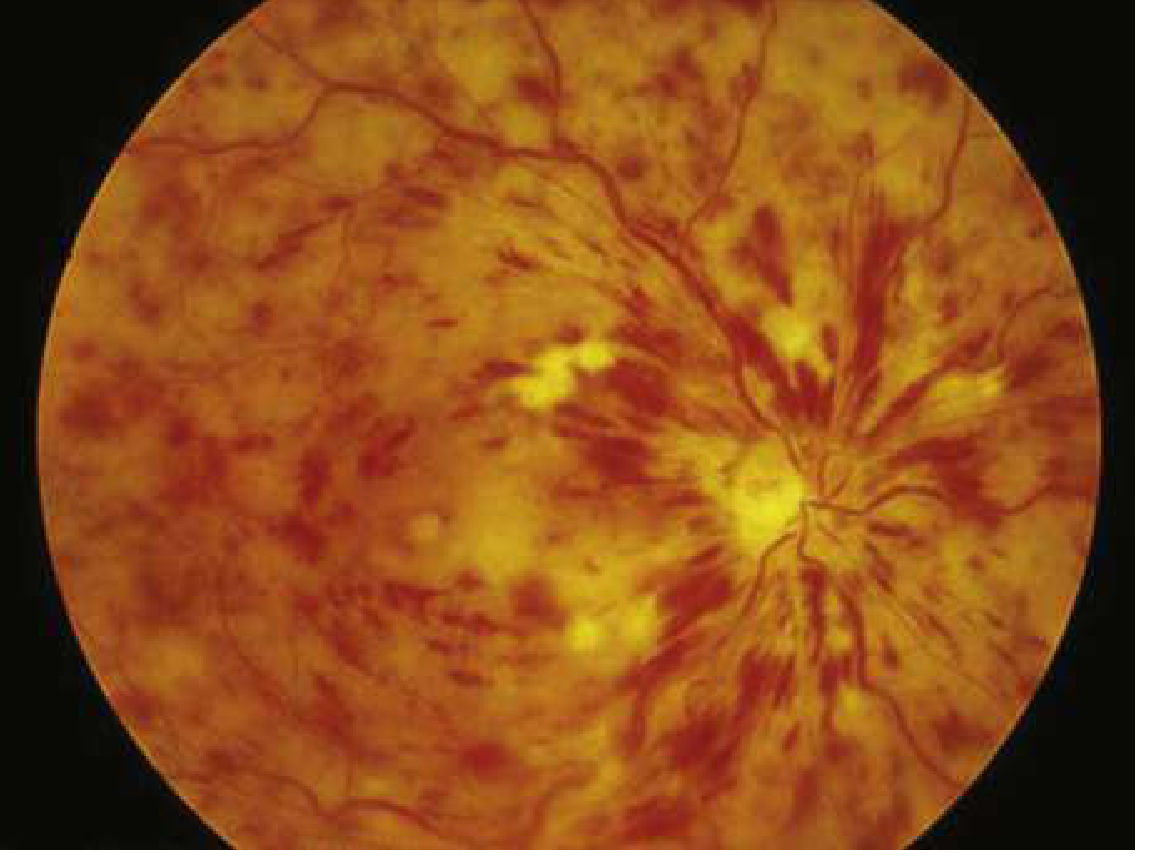
3. Central Retinal Vein Occlusion (CRVO)
Presentation: Sudden onset painless vision loss in one eye.
Fundoscopic signs - "Blood and Thunder" appearance:
- Diffuse retinal hemorrhages in all four quadrants
- Disc edema, dilated tortuous veins
- Cotton-wool spots
- Ischemic CRVO presents with sudden painless vision loss; non-ischemic (perfused) CRVO may have only mild visual impairment
Predisposing factors: Hypertension, hyperlipidemia, diabetes mellitus, vasculitides, hyperviscosity syndromes, smoking.
Complications: Macular edema (most common cause of vision loss), neovascular glaucoma, vitreous hemorrhage.
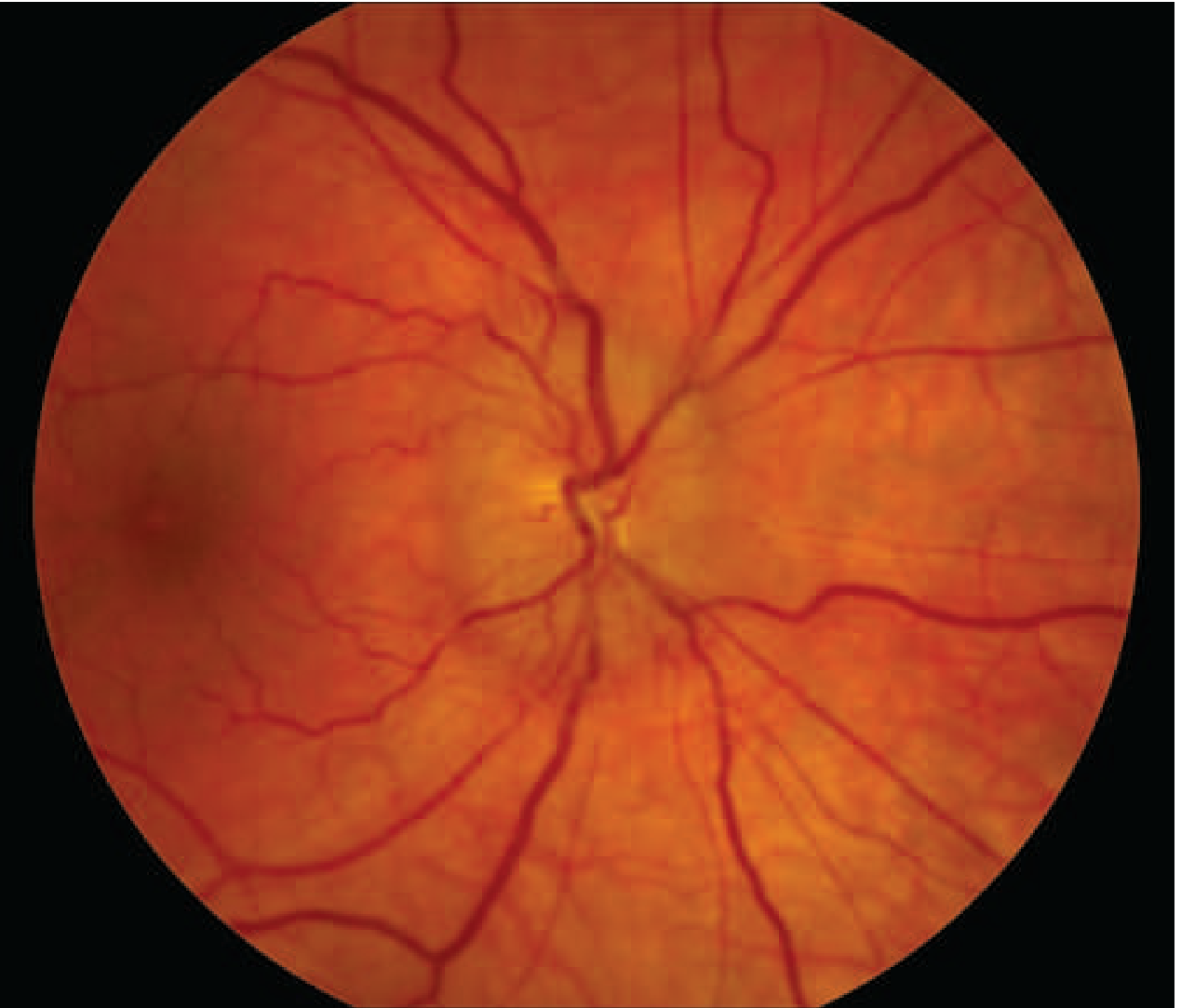
4. Ischemic Optic Neuropathy (ION)
There are two anatomical types and two etiological subtypes:
Anterior Ischemic Optic Neuropathy (AION)
- Arteritic AION (A-AION) - due to Giant Cell Arteritis (GCA/temporal arteritis)
- Non-arteritic AION (NA-AION) - noninflammatory vascular disease
Common features of both:
- Painless vision loss (though optic neuritis is typically painful)
- Age generally >60 for arteritic, >50 for non-arteritic
- Large RAPD
- Visual field defect respecting the horizontal midline (altitudinal defect)
- Pale and swollen optic disc on fundoscopy
A-AION (GCA-related):
- Accounts for ~5% of AION cases
- Associated systemic symptoms: jaw claudication, scalp tenderness, headache, polymyalgia rheumatica, weight loss, low-grade fever - but up to 25% present with vision loss as the only symptom
- Vision loss may be preceded by amaurosis fugax
- Can progress to involve the second eye (untreated): unilateral 46%, sequential 37%, simultaneous bilateral 17%
- ESR and CRP elevated (very high ESR typical)
- Treatment is a true emergency: high-dose IV methylprednisolone (1 g/day x 3 days) then oral prednisone; start immediately without waiting for biopsy
- Tocilizumab (anti-IL-6) is an effective steroid-sparing agent for sustained suppression
- Temporal artery biopsy confirms diagnosis (harvest long segment; treat first, biopsy second)
NA-AION:
- More common than arteritic
- Age typically >50 years, associated with vascular risk factors (HTN, DM, hyperlipidemia)
- Can be precipitated by: anemia, hypovolemia, dehydration, systemic hypotension, dialysis-related BP fluctuations
- Structural risk factor: "disc-at-risk" - small, crowded optic disc with a small cup-to-disc ratio
- No proven treatment - glucocorticoids should NOT be prescribed
- Contralateral eye risk is elevated
Posterior Ischemic Optic Neuropathy (PION)
- Uncommon
- Caused by severe anemia + hypotension (major surgery - cardiac or lumbar spine, GI bleeding, shock, renal dialysis)
- Normal fundus appearance initially; disc swelling may develop later
- Treatment: immediate blood transfusion and blood pressure reversal
5. Retinal Detachment
Presentation: Symptoms begin with dark floaters or "cobwebs" progressing over hours to painless visual loss; preceded by flashing lights (photopsia) and a curtain or veil in the visual field. Floaters associated with flashing lights indicate higher incidence of concurrent retinal tears.
Key point: If the detachment includes the fovea, central vision is lost and outcome is inversely related to duration of macular involvement.
Management:
- Emergent ophthalmology consultation
- Any suspected retinal tear/detachment requires immediate tamponade or retinopexy to prevent progression to macular involvement
- Surgery required for associated retinal detachment with vitreous hemorrhage
6. Vitreous Hemorrhage
Presentation: Sudden painless visual loss; floaters or "cobwebs" that may progress to complete visual obscuration.
Causes: Diabetic retinopathy (most common), retinal tear, posterior vitreous detachment, CRVO, trauma, subarachnoid hemorrhage, sickle cell disease, lupus.
Management:
- Limit activity, avoid anticoagulants, elevate head of bed (to let blood settle)
- Fundus ultrasonography if direct visualization is obscured
- Surgery (vitrectomy) if associated retinal detachment or persistent hemorrhage
7. Ophthalmic Artery Occlusion
- More severe than CRAO
- No cherry-red spot - the entire retina appears whitened (choroidal circulation also affected)
- Vision usually reduced to light perception or no light perception
- Increased concern for GCA
Binocular (Bilateral) Acute Painless Vision Loss
| Cause | Key Features |
|---|---|
| Occipital lobe stroke | Homonymous hemianopia; patient may not recognize binocularity; MRI/DWI confirms |
| Bilateral ischemic optic neuropathies | Rare; usually GCA |
| Pituitary apoplexy | Acute hemorrhage into pituitary adenoma; bitemporal field loss; prompt neurosurgical intervention + steroids required |
| Vertebrobasilar insufficiency | Transient, often with other brainstem signs |
| Head trauma | Bilateral cortical or optic nerve injury |
Transient Monocular Vision Loss (TMVL / Amaurosis Fugax)
- Vision loss lasting seconds to minutes, then fully recovering
- Most common cause: embolus to the retinal or ophthalmic artery (usually from ipsilateral carotid atheroma)
- Other causes: ocular ischemic syndrome, GCA, vasospasm (migraine), orthostatic hypotension, impending CRVO, optic disc drusen
- TMVL is a TIA equivalent - warrants full stroke workup (carotid imaging, cardiac echo, antiplatelet/anticoagulation)
- Reported prior to major events in: 2% of CRAO, 14% of BRAO, 32% of GCA with ocular involvement
Emergency Diagnostic Approach
History
- Onset (seconds = embolic; hours = detachment)
- Monocular vs. binocular
- Preceding floaters/flashing lights (retinal detachment)
- Prior episodes (amaurosis fugax)
- Systemic symptoms (headache, jaw claudication = GCA)
- Vascular risk factors (HTN, DM, smoking, AF)
- Age
Examination
| Finding | Diagnosis |
|---|---|
| Cherry-red spot + pale retina | CRAO |
| "Blood and thunder" fundus (diffuse hemorrhages) | CRVO |
| Pale, swollen disc + altitudinal field defect | AION |
| Absent red reflex, vitreous opacities | Vitreous hemorrhage |
| Billowing gray membrane, loss of choroidal pattern | Retinal detachment |
| RAPD (Marcus Gunn pupil) | Optic nerve or retinal disease |
| Homonymous hemianopia | Cortical/retrochiasmal lesion |
Key Investigations
| Test | Purpose |
|---|---|
| ESR, CRP, platelets | Rule out GCA (if ≥55 years) |
| Blood pressure | Hypertensive urgency/emergency |
| Fasting glucose, HbA1c, CBC, PT/PTT | Metabolic/hematologic causes |
| Carotid Doppler ultrasound | Carotid stenosis (embolic source) |
| ECG, echocardiography, Holter monitor | Cardiac embolic sources (AF, valvular disease) |
| CT/MRI brain | Cortical/chiasmal/retrochiasmal lesion; pituitary apoplexy |
| OCT, IVFA | Retinal vascular mapping, macular assessment |
| Bedside B-scan ultrasonography | Vitreous hemorrhage vs. retinal detachment when fundus obscured |
| Temporal artery biopsy | Confirm GCA |
Differentiating Painful vs. Painless Vision Loss
Pain is an important triage feature:
Painful acute vision loss: Acute angle-closure glaucoma, corneal abrasion/ulcer, uveitis, endophthalmitis, optic neuritis (~90% have pain with eye movement), corneal hydrops
Painless acute vision loss: All the vascular and structural causes described above (CRAO, CRVO, AION, retinal detachment, vitreous hemorrhage, cortical stroke, amaurosis fugax)
Note: Optic neuritis is painful in about 90% of cases but ~10% are painless - keep it in the differential for younger patients with subacute monocular visual loss and RAPD.
Summary Table of Key Differentiators
| Condition | Age | Laterality | Onset | Fundus | Key Feature |
|---|---|---|---|---|---|
| CRAO | 50-70 | Unilateral | Seconds | Cherry-red spot, pale retina | Embolic; treat as stroke |
| CRVO | Any | Unilateral | Hours | Blood and thunder hemorrhages | HTN, DM risk factors |
| AION (arteritic) | >60 | Uni/Bilateral | Hours | Pale swollen disc | Jaw claudication, elevated ESR; emergency steroids |
| AION (non-arteritic) | >50 | Unilateral | Hours | Pale swollen disc, altitudinal defect | Disc-at-risk; no treatment |
| Retinal detachment | Any | Unilateral | Hours | Grey billowing retina | Floaters + flashes + curtain |
| Vitreous hemorrhage | Any | Unilateral | Sudden | Loss of red reflex | Diabetic/trauma/vein occlusion |
| Occipital stroke | Older | Bilateral | Sudden | Normal | Homonymous hemianopia |
| Amaurosis fugax | >50 | Unilateral | Seconds-minutes (recovers) | Normal | TIA equivalent; carotid workup |
Sources:
- The Wills Eye Manual, 7th ed. (Sections 1.1, 11.6, 11.7, 11.8)
- Rosen's Emergency Medicine, 9th ed. (Chapter 57)
- Harrison's Principles of Internal Medicine, 22nd ed. (Chapter 34)
- Bradley and Daroff's Neurology in Clinical Practice (Chapter 16)
- Textbook of Family Medicine, 9th ed.
- Goldman-Cecil Medicine (Chapter 57)
- Firestein & Kelley's Textbook of Rheumatology (Chapter 44)
This is a shared conversation. Sign in to Orris to start your own chat.