Geriatric Services
Asking for Preferences
It looks like the response came through as "Park" - that may be a selection error. Could you clarify what you'd like to know about Geriatric Services? For example:
- A general overview of geriatric care
- Geriatric syndromes (falls, delirium, frailty, dementia)
- Comprehensive Geriatric Assessment (CGA)
- Polypharmacy and medication management in older adults
- A specific condition, drug, or clinical scenario
Just let me know and I'll dive in!
Textbooks park
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
I now have comprehensive content from Park's Textbook. Here is a thorough summary of the Geriatric Services section:
Geriatric Services
Source: Park's Textbook of Preventive and Social Medicine
1. Definitions and Scope
| Term | Meaning |
|---|---|
| Gerontology | Study of physical and psychological changes incident to old age |
| Geriatrics / Clinical Gerontology | The care of the aged |
| Social Gerontology | Deals with the social problems of the increasing elderly population |
| Experimental Gerontology | Research into the basic biology of ageing - physiology, biochemistry, pathology, psychology |
| Geriatric Gynaecology | An emerging field addressing prolapse repair, non-specific vaginitis, ovarian tumours, and sexual problems in elderly women |
"You do not heal old age. You protect it; you promote it; you extend it." - Sir James Sterling Ross
2. Size of the Problem (Epidemiology)
- In 2019, an estimated 694 million older persons worldwide; 540 million in developing countries
- Italy and Japan have the highest proportions (~24% and ~16% respectively)
- By 2025: expected to exceed 1.2 billion elderly globally, with ~840 million in low-income countries
- In India (2019): 9.3% of the total population was above 65 years - a significant sociological and healthcare policy challenge
3. Health Problems of the Aged
(a) Problems Due to the Ageing Process
- Senile cataract and glaucoma
- Nerve deafness
- Osteoporosis affecting mobility
- Emphysema
- Failure of special senses
- Changes in mental outlook
(b) Long-Term / Chronic Illness
- Cardiovascular disease: Atherosclerosis, hypertension, thrombus formation - major cause of death in developed countries
- Cancer: Risk rises sharply after age 40; prostate cancer common after 65
- Accidents: Fragile bones due to decalcification; fracture neck of femur is a classic geriatric problem; accidents more common at home
- Diabetes: ~75% of diabetics are over 50 years of age
- Locomotor disorders: Osteoarthritis, rheumatoid arthritis, gout, spondylitis, fibrositis - cause more disability than any other chronic disease in the elderly
- Respiratory illnesses: Chronic bronchitis, asthma, emphysema
- Genitourinary: Prostatic enlargement, dysuria, nocturia, urgency
(c) Psychological Problems
- Mental changes: Impaired memory, rigidity of outlook, dislike of change
- Sexual adjustment: Cessation of reproduction in women (40-50 years), diminished sexual activity in men; irritability, jealousy, despondency
- Emotional disorders: Depression, inner withdrawal, bitterness, suicidal tendency - from failure to adapt to ageing
4. Lifestyle and Healthy Ageing
Key modifiable factors:
- Diet and nutrition: Good diet reduces disease risk; overnutrition replaces undernutrition as countries develop
- Physical activity: Regular exercise
- Avoidance of smoking and alcohol
- Sleep hygiene
5. Prevention - Three Tiers (Table 31)
| Level | Focus |
|---|---|
| Primary | Health habits - smoking cessation, reducing alcohol, obesity control, nutrition, physical activity, sleep; also coronary heart disease prevention |
| Secondary | Screening for hypertension, diabetes, periodontal disease, dental caries, sensory impairment, medication side-effects |
| Tertiary | Rehabilitation of physical, cognitive, and functional deficits; caretaker support; measures to prevent loss of autonomy |
6. Social Welfare Measures for the Elderly (Western Model)
- National assistance and supplementary pensions
- Home services and home care services
- Meals on wheels services
- Old folk's homes and day-care centres
- Sitters-up service
- Health visitor services
HelpAge India supports: free cataract operations, mobile medicare units, income generation, micro-credit, old-age homes, "Adopt-a-Gran" scheme, disaster mitigation - reaching 6 million senior citizens through 3,084 projects.
7. National Programme for Health Care of Elderly (India - NPHCE)
Services at Community Health Centre (CHC) level:
Essential services:
- Medical rehabilitation
- Compilation of elderly data from PHC, forwarding to district nodal officers
- Home visits to disabled/bed-ridden persons by rehabilitation workers
- Geriatric clinic: twice a week
Desirable services:
- Physical Medicine & Rehabilitation (PMR): exercise therapy, heat therapy, ROM exercises, cervical and lumbar traction, referral and follow-up
- Primary prevention of disabilities
- Screening, early identification, counselling
- Disability certification
8. Implications for Preventive and Social Medicine
- The ageing population is both a medical and sociological challenge
- Developing countries face a double burden - infectious AND non-communicable diseases, without sufficient resources
- The predicted explosion of NCDs (cardiovascular disease, cancer, depression) will cause enormous human and social costs unless preventive action is taken
- Modern philosophy: older persons must remain active community members; the community must help fight the "triple evils" of poverty, loneliness, and ill-health
Park's Textbook of Preventive and Social Medicine, Block 9 - Preventive Medicine and Geriatrics
Mental health
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
From parks
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from Park's on Mental Health. Here is the complete summary:
Mental Health
Source: Park's Textbook of Preventive and Social Medicine
1. Definition of Mental Health
WHO Definition: "Mental health is a state of well-being in which an individual realizes his or her own abilities, can cope with the normal stress of life, can work productively and is able to make a contribution to his or her community."
The WHO's broader definition of health - "a state of complete physical, mental and social well-being" - recognizes mental health as inseparable from overall health.
Mental health is not just about the individual; it is also about the individual's relationship to the community, social institutions, and the way society guides living, working, leisure, and economic life.
2. Problem Statement
Global Burden
- Depression: 300 million people affected
- Bipolar affective disorders: 60 million
- Schizophrenia and other psychoses: 23 million
- Dementia: 50 million
- Mental, neurological, and substance use disorders together account for 13% of the total global burden of disease
- Depression alone contributes 4.3% of the global burden and is among the largest single causes of disability - accounting for 11% of all years lived with disability globally, particularly in women
- Economic impact: cumulative global loss estimated at US$ 16.3 trillion between 2011 and 2030
India - National Mental Health Survey (NMHS) 2015
Key findings from the survey conducted across 12 states:
- Nearly 150 million Indians aged 13 and above are likely to suffer from one or more mental health problems
- Mental health problems are more prevalent in urban areas
- 7.3% of young adolescents had a mental health disorder
- Neurosis and stress-related disorders (phobias, anxiety) affected twice as many women as men
- Alcohol use disorder in men: 4.6% among the 18+ population
- Illicit substance use disorders: 0.6%
- Less than 2% had severe mental illness (psychosis or bipolar disorder)
3. Warning Signals of Poor Mental Health
(William C. Menninger, Menninger Foundation)
- Always worrying
- Unable to concentrate without recognized reason
- Continually unhappy without cause
- Losing temper easily and often
- Troubled by regular insomnia
- Wide mood fluctuations (depression to elation and back) causing incapacitation
- Dislike of being with people
- Upset when daily routine is disturbed
- Children consistently getting on one's nerves
- Constantly bitter or "browned off"
- Afraid without real cause
- Always right, the other person always wrong
- Numerous aches and pains for which no physical cause is found
Help is necessary if the answer to any of these is a definite "yes."
4. Types of Mental Illness (ICD-10 Classification)
| Category | Examples |
|---|---|
| Organic / symptomatic mental disorders | Dementia in Alzheimer's disease, delirium |
| Disorders due to psychoactive substance use | Harmful use of alcohol, opioid dependence |
| Schizophrenia, schizotypal & delusional disorders | Paranoid schizophrenia, acute psychotic disorders |
| Mood (affective) disorders | Bipolar affective disorder, depressive episode |
| Neurotic, stress-related & somatoform disorders | Generalized anxiety disorder, OCD |
| Behavioural syndromes with physiological disturbances | Eating disorders, non-organic sleep disorders |
| Disorders of adult personality and behaviour | Paranoid personality disorder, trans-sexualism |
| Mental retardation | - |
| Disorders of psychological development | Specific reading disorders, childhood autism |
5. Causes of Mental Ill-Health
(a) Organic Conditions
Cerebral arteriosclerosis, neoplasms, metabolic diseases, neurological and endocrine diseases, chronic diseases (TB, leprosy, epilepsy)
(b) Heredity
- A child of two schizophrenic parents is 40 times more likely to develop schizophrenia than a child of healthy parents
(c) Social and Pathological Causes
Worries, anxieties, emotional stress, tension, frustration, unhappy marriages, broken homes, poverty, industrialization, urbanization, changing family structure, population mobility, economic insecurity, cruelty, neglect
(d) Environmental Factors
- Toxic substances: carbon disulfide, mercury, manganese, lead
- Psychotropic drugs: barbiturates, alcohol, griseofulvin
- Nutritional deficiencies: thiamine, pyridoxine
- Minerals: iodine deficiency
- Infective agents: measles, rubella during prenatal/perinatal periods
- Traumatic factors: road and occupational accidents
- Radiation: especially during neural development
6. Crucial Points in the Lifecycle for Mental Health
| Life Stage | Key Mental Health Concern |
|---|---|
| Prenatal period | Pregnancy is stressful; emotional support needed |
| First 5 years | Roots of mental health lie in early childhood; warm mother-father-child relationship is essential |
| School child | Teacher-pupil relationship and classroom climate are critical; child guidance clinics for emotional problems |
| Adolescence | Stormy transition; needs: being needed, independence, adjustment to opposite sex, freedom to question beliefs |
| Old age | Mental illness due to organic brain conditions, economic insecurity, lack of home, poor social status |
7. Comorbidity with Physical Disease
- Depression predisposes to myocardial infarction and diabetes; both conditions conversely increase likelihood of depression
- Low socioeconomic status, alcohol use, and stress are common risk factors for both mental and non-communicable diseases
- Mental disorders + substance use disorders together impose an enormous toll
Human Rights Dimension
People with mental disorders are frequently:
- Led into poverty
- Made homeless or inappropriately incarcerated
- Denied rights to work, education, marriage, voting, and reproductive rights
- Subject to physical/sexual abuse and neglect in health facilities
8. Mental Health Services
A community mental health service addresses not just treatment but also promotion, preservation, and prevention. Components include:
- Early diagnosis and treatment
- Rehabilitation
- Group and individual psychotherapy
- Mental health education
- Use of modern psychoactive drugs
- After-care services
9. Comprehensive Community Mental Health Programme
Since 95% of psychiatric cases can be treated at or near the patient's home, the modern trend is full integration of psychiatric services with general health services.
Nine essential elements:
- In-patient services
- Out-patient services
- Partial hospitalization
- Emergency services
- Diagnostic services
- Pre-care and after-care (including foster home placement and home visiting)
- Education services
- Training
- Research and evaluation
10. National Mental Health Programme (NMHP) - India
Launched: 1982
Aims:
- (a) Prevention and treatment of mental/neurological disorders and their disabilities
- (b) Use of mental health technology to improve general health services
- (c) Application of mental health principles in national development to improve quality of life
Objectives:
- Ensure availability and accessibility of minimum mental health care for all - especially the most vulnerable
- Encourage application of mental health knowledge in general health care and social development
- Promote community participation and self-help in the community
Programme Strategies:
- Integration of mental health with primary health care through NMHP
- Provision of tertiary care institutions for mental disorders
- Eradicating stigmatization through Central and State Mental Health Authorities
District Mental Health Programme (DMHP) Components:
- (a) Training programmes for all mental health team workers
- (b) Public education to increase awareness and reduce stigma
- (c) OPD and indoor services for early detection and treatment
- (d) Data collection and research at community level
DMHP Promotive and Preventive Activities:
- School mental health services: Life skills education, counselling
- College counselling services: Through trained teachers/counsellors
- Workplace stress management: Formal and informal sectors (including farmers and women)
- Suicide prevention services: Counselling centres, sensitization workshops, IEC, helplines
Thrust Areas:
- Expanded and effective District Mental Health Programme nationwide
- Modernization of mental hospitals (away from custodial role)
- Upgrading psychiatry departments in medical colleges
- Strengthening Central and State Mental Health Authorities
Current coverage: 517 districts across 36 states
11. WHO Comprehensive Mental Health Action Plan 2013-2020
Vision: A world in which mental health is valued, promoted and protected; persons with mental disorders exercise full human rights and access high-quality, culturally appropriate care.
Overall Goal: Promote well-being, prevent disorders, provide care, enhance recovery, protect human rights, and reduce mortality/morbidity/disability.
Four Objectives:
- Strengthen effective leadership and governance for mental health
- Provide comprehensive, integrated, responsive mental health and social care services in community-based settings
- Implement strategies for promotion and prevention in mental health
- Strengthen information systems, evidence, and research for mental health
Park's Textbook of Preventive and Social Medicine - Block 11 (Mental Health) and Block 7 (NMHP)
Essential Medicines
From parks Essential Medicines
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive content. The list is extensive, so let me compile the full structured overview including concept, criteria, dosage forms, pharmacovigilance, and the complete medicine sections seen so far.
Essential Medicines
Source: Park's Textbook of Preventive and Social Medicine, Block 7
1. The Concept of Essential Medicines (WHO)
Definition: Essential medicines are those that satisfy the priority health care needs of the population.
They are intended to be:
- Available at all times within functioning health systems
- In adequate amounts
- In appropriate dosage forms
- With assured quality and adequate information
- At a price the individual and the community can afford
The concept is flexible and adaptable - which medicines are regarded as essential remains a national responsibility. Experience shows that careful selection of a limited range of essential medicines results in:
- Higher quality of care
- Better medicines management (including quality of prescribed medicines)
- More cost-effective use of available health resources
2. National List of Essential Medicines of India (NLEM) - 2015
India first prepared its National List of Essential Medicines in 1996, subsequently revised in 2003, 2011, and 2015.
India has adopted the WHO concept but maintains its own list that differs from the WHO list due to differences in national circumstances - addressing India's own disease burden, including medicines used in national health programmes and for emerging/re-emerging infections.
Medicines are categorized according to therapeutic use (a medicine with more than one indication may appear in more than one category).
Criteria for Inclusion in NLEM
| # | Criterion |
|---|---|
| 1 | Must be approved/licensed in India |
| 2 | Must be useful in a disease that is a public health problem in India |
| 3 | Must have proven efficacy and safety based on valid scientific evidence |
| 4 | Must be cost-effective |
| 5 | Must be aligned with current treatment guidelines for the disease |
| 6 | Must be stable under storage conditions in India |
| 7 | Price of total treatment to be considered - not just the unit price |
| 8 | Fixed dose combinations (FDCs) generally not included unless they unequivocally prove advantage over individual ingredients in terms of: increasing efficacy, reducing side effects, and/or improving compliance |
| 9 | List is level-based: P = Primary, S = Secondary, T = Tertiary health care |
3. Dosage Forms and Formulations
| Route | Forms |
|---|---|
| Oral solid | Tablet (immediate-release: film-coated, uncoated, sugar-coated, crushable, chewable, dispersible; enteric-coated for modified release), Capsule (hard/soft gelatin), Sachet |
| Oral liquid | Syrup, Suspension, Elixir |
| Injectable | Conventional liquid injection, Powder for injection, Depot, Liposomal/lipid complex |
| Topical | Ointment, cream, and others |
Crushable, chewable, and dispersible tablets are especially useful for paediatric and elderly patients.
4. Monitoring of Medicine Safety - Pharmacovigilance
- Safety monitoring is an integral part of the overall surveillance of medicine use
- Aims of pharmacovigilance:
- Identify new, previously unrecognized adverse effects of medicines
- Quantify their risks
- Communicate findings to drug regulatory authorities, health professionals, and the public
- Voluntary reporting of adverse effects (the basis of the International WHO Programme for Drug Monitoring) has effectively identified previously undescribed adverse effects
- Risk of adverse effects is evaluated using observational epidemiological methods: case-control, cohort, and case-population studies
5. National List of Essential Medicines - India 2015 (Selected Sections)
(P = Primary care, S = Secondary care, T = Tertiary care)
Section 1: Anaesthetic Agents
1.1 General Anaesthetics and Oxygen
| # | Medicine | Level | Dosage Form |
|---|---|---|---|
| 1.1.1 | Halothane | S, T | Inhalation |
| 1.1.2 | Isoflurane | S, T | Inhalation |
| 1.1.3 | Ketamine | P, S, T | Injection 10 mg/ml; 50 mg/ml |
| 1.1.4 | Nitrous oxide | P, S, T | Inhalation |
| 1.1.5 | Oxygen | P, S, T | Inhalation (Medicinal gas) |
| 1.1.6 | Propofol | P, S, T | Injection 10 mg/ml |
| 1.1.7 | Sevoflurane | T | Inhalation |
| 1.1.8 | Thiopentone | P, S, T | Powder for Injection 0.5 g / 1 g |
1.2 Local Anaesthetics
| # | Medicine | Level | Dosage Form |
|---|---|---|---|
| 1.2.1 | Bupivacaine | S, T | Injection 0.25%, 0.5%, 0.5% with 7.5% glucose |
| 1.2.2 | Lignocaine | P, S, T | Topical 2-5%; Injection 1%, 2%, 5% with glucose |
| 1.2.3 | Lignocaine + Adrenaline | P, S, T | Injection 1%/2% + 1:200,000 adrenaline |
| 1.2.4 | Prilocaine + Lignocaine | T | Cream 2.5% + 2.5% |
Section 6.5: Anti-Infective Medicines (Selected)
6.5.1 Antiamoebic and Antigiardiasis
| Medicine | Level | Dosage Form |
|---|---|---|
| Diloxanide furoate | P, S, T | Tablet 500 mg |
| Metronidazole | P, S, T | Tablet 200 mg, 400 mg; Injection 500 mg/100 ml; Oral liquid 200 mg/5 ml |
6.5.2 Antileishmaniasis
| Medicine | Level | Dosage Form |
|---|---|---|
| Amphotericin B (conventional + liposomal) | S, T | Powder for Injection 50 mg |
| Miltefosine | P, S, T | Capsule 10 mg, 50 mg |
| Paromomycin | P, S, T | Injection 375 mg/ml |
6.5.3 Antimalarial Medicines
For Curative Treatment:
| Medicine | Level | Dosage Form |
|---|---|---|
| Artemether + Lumefantrine | P, S, T | Tablets 20/120 mg; 40/240 mg; 80/480 mg; Oral liquid |
| Artesunate | P, S, T | Powder for Injection 60 mg, 120 mg |
| Artesunate + Sulphadoxine-Pyrimethamine | P, S, T | Combi packs in multiple strengths |
| Chloroquine | P, S, T | Tablet 150 mg; Oral liquid 50 mg/5 ml |
| Clindamycin | P, S, T | Capsule 150 mg, 300 mg |
| Primaquine | P, S, T | Tablet 2.5 mg, 7.5 mg, 15 mg |
Note: The NLEM 2015 contains medicines across all major therapeutic categories including analgesics, antibiotics, cardiovascular drugs, antidiabetics, antiretrovirals, vaccines, and many more. The full list runs across 27+ sections. The sections shown above are a representative sample from Park's.
Park's Textbook of Preventive and Social Medicine - Block 7, pp. 547 onwards
From parks Health Planning & Management
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I have all the content needed. Here is the comprehensive write-up:
Health Planning & Management
Source: Park's Textbook of Preventive and Social Medicine, Block 12
1. Planning and Management - Overview
Administration = "getting things done" Management = "the purposeful and effective use of resources - manpower, materials and finances - for fulfilling a pre-determined objective"
The four basic activities of management:
| Activity | Meaning |
|---|---|
| (i) Planning | Determining what is to be done |
| (ii) Organizing | Setting up the framework/apparatus; enabling groups to do the work |
| (iii) Communicating | Motivating people to do the work |
| (iv) Monitoring (Controlling) | Checking that work is progressing satisfactorily |
2. Health Planning
Definition (National Health Planning):
"The orderly process of defining community health problems, identifying unmet needs and surveying the resources to meet them, establishing priority goals that are realistic and feasible and projecting administrative action to accomplish the purpose of the proposed programme."
Health planning is part of national development planning. Its purpose is to improve health services through the economic utilization of material, manpower, and financial resources.
Key Terms
| Term | Definition |
|---|---|
| Objective | Precise end-point - either achieved or not achieved |
| Target | A discrete activity (e.g., number of vasectomies done, blood films collected); allows a degree of achievement |
| Goal | The ultimate desired state; not constrained by time or resources; not necessarily attainable |
| Plan | A blueprint for taking action. Contains: objectives, policies, programmes, schedules, and budget |
| Programme | A sequence of activities designed to implement policies |
Health Needs vs. Demands
- Health needs = deficiencies in health calling for preventive, curative, control, or eradication measures (e.g., safe water, nutrition, immunization, family planning)
- People's needs as perceived by themselves may differ from experts' assessments
- In a democratic society, people's needs may be presented as demands
Resources
Resources = manpower, money, materials, skills, knowledge, techniques, and time needed for action towards stated objectives. Resources can be readily wasted without proper planning and management.
3. Pre-Planning Conditions
For successful health planning, the following pre-conditions are required:
- (a) Political will - Commitment at the highest levels (e.g., India's Family Planning Act, 1971)
- (b) Legal framework - Legislative backing (e.g., acts passed by Parliament)
- (c) Organization for planning - A structured body for preparing the plan (e.g., India's Planning Commission)
- (d) Administrative capacity - Coordination and implementation capacity at all levels (vested in Central and State Ministries of Health in India)
4. The Planning Cycle
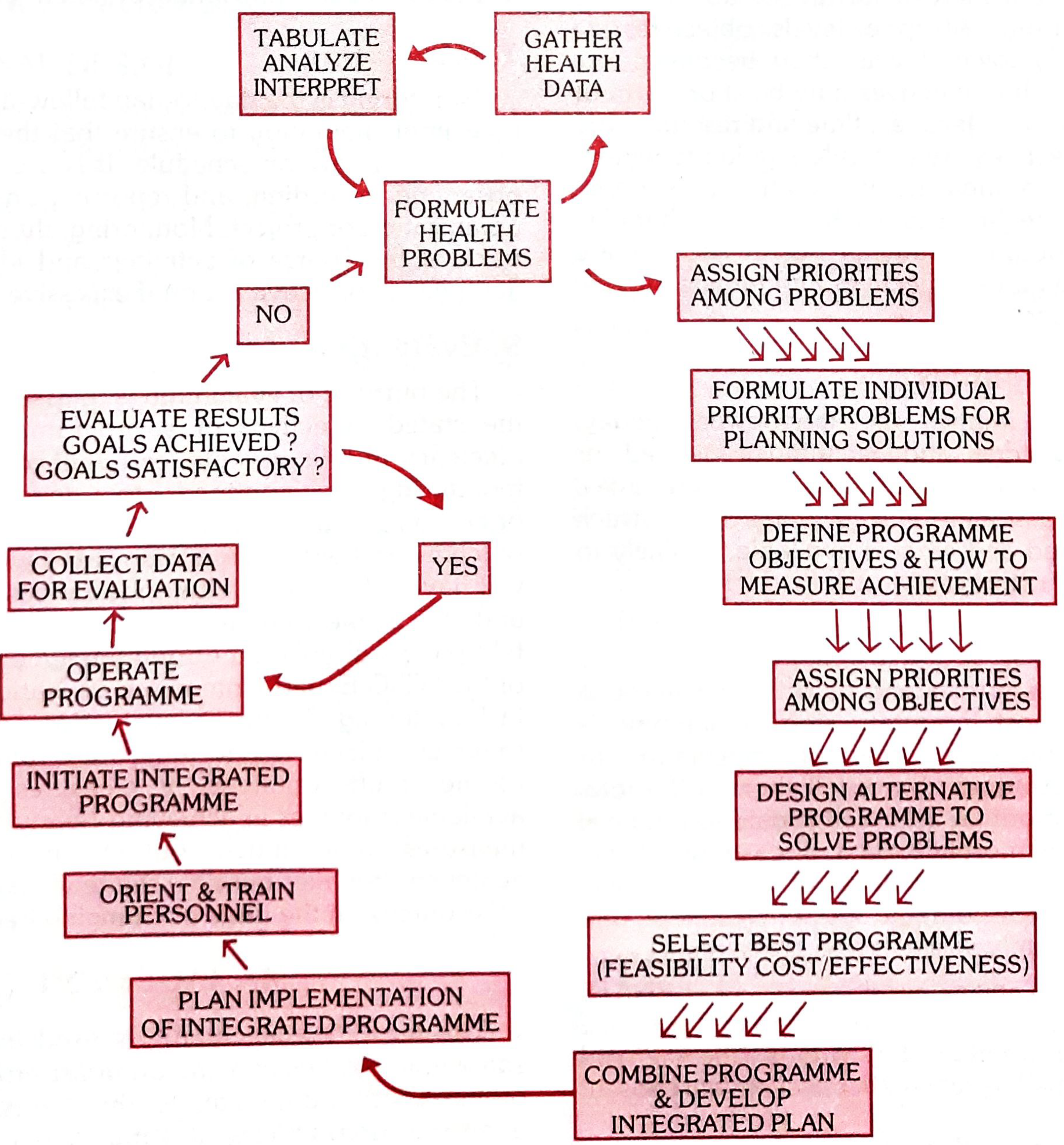
The planning cycle involves a succession of steps:
Step 1: Analysis of the Health Situation
Minimum data required:
- (a) Population, age and sex structure
- (b) Statistics of morbidity and mortality
- (c) Epidemiology and geographical distribution of diseases
- (d) Medical care facilities - hospitals, health centres, public and private agencies
- (e) Technical manpower of various categories
- (f) Training facilities available
- (g) Attitudes and beliefs of the population towards disease, cure, and prevention
Step 2: Establishment of Objectives and Goals
- Objectives must be set at all organizational levels (general at the top, specific at lower levels)
- May be short-term or long-term
- Serve both as a guide to action and a yardstick to measure performance
- Modern tools: cost-benefit analysis, input-output study
Step 3: Assessment of Resources
Balance struck between what is required and what is available (manpower, money, materials, skills, knowledge, techniques)
Step 4: Fixing Priorities
Once problems, resources, and objectives are determined, priorities are set among competing needs
Steps 5-8: Programme Design, Implementation, Monitoring, and Evaluation
The cycle is continuous - evaluation feeds back into re-analysis and re-planning
5. Management Methods and Techniques
A. Methods Based on Behavioural Sciences
1. Organizational Design
- Poor organization = waste of resources
- Organization must be suited to its current situation and the needs it serves
- Health service organization should meet the health needs and demands of the people
- Should be reviewed every few years due to changing concepts, problems, and technology
2. Personnel Management
- Skilful use of human resources; includes:
- Proper selection, training, and motivation
- Division of responsibility and distribution of roles
- Avoiding "square pegs in round holes" (technical staff not suited to administration should not be given administrative burdens)
- Incentives for better work and opportunities for promotion
- Effective design of "health teams"
3. Communication
- Communication barriers exist at multiple levels: doctor-patient, doctor-nurse, senior-junior, directorate-ministry, and between ministries
- Barriers cause: delays in reporting, delays in statistics compilation, delays in release of supplies and salaries, delays in remedial action
- A key task of health management is to establish suitable vertical and horizontal communication channels
4. Information Systems
- Information needed for day-to-day management of the health system
- System must be tailored to management needs
- Sources: both formal and informal
- Health Management Information System (HMIS): core tool for decision-making
5. Management by Objectives (MBO)
- Setting clear, measurable objectives at all levels of the organization
- Staff are evaluated against the objectives they help to set
B. Quantitative Methods
1. Cost-Benefit Analysis
- Economic benefits of a programme are compared with its cost
- Benefits expressed in monetary terms
- Main drawback: benefits in health (e.g., lives saved) cannot always be monetized
2. Cost-Effectiveness Analysis
- More promising for health field than cost-benefit analysis
- Benefits expressed as results achieved (e.g., lives saved, days free from disease) rather than monetary terms
3. Cost-Accounting
- Provides basic data on cost structure of any programme
- Three purposes: (a) cost control; (b) planning and allocation of manpower and financial resources; (c) pricing of cost reimbursement
4. Input-Output Analysis
- Input = all health service activities consuming resources (manpower, money, materials, time)
- Output = useful outcomes (cases treated, lives saved, inoculations performed)
- Shows how much input is needed to produce a unit of output; allows modeling effects of changing inputs
5. Model
- An abstraction of reality used to understand how factors in a situation interact
- Basic concept of management science; aids the decision-making process
6. Systems Analysis
- Helps decision-makers choose a course of action by investigating the problem, searching out objectives, finding alternative solutions, and evaluating them in terms of cost-effectiveness
- Applicable to: hospital supply systems, information systems, outpatient clinics, total community health service systems
7. Network Analysis
- A graphic plan of all events and activities required to reach an end objective
- Two common types: PERT (Programme Evaluation and Review Technique) and CPM (Critical Path Method)
- Brings greater discipline in planning
8. Planning-Programming-Budgeting System (PPBS)
- Helps decision-makers allocate resources to achieve objectives in the most effective way
- Groups activities into programmes related to each objective
- Related approach: Zero Budget Approach - all budgets start at zero and must be justified on a year-to-year basis
9. Work Sampling
- Systematic observation and recording of activities at predetermined or random intervals
- Parameters analyzed: type of activities performed, time needed for specified jobs
- Used for doctors, nurses, pharmacists, and laboratory technicians
- Helps standardize methods and determine manpower needs
10. Decision Making
- Analogous to differential diagnosis in clinical medicine
- Decisions should be made at the level where the best decisions can be made (not necessarily at the top)
- Should not be made with incomplete data
- Health sector decisions: development of resources, optimum workload, strategies for providing care
6. Health Planning in India
Health planning in India is an integral part of national socio-economic planning. Key milestones:
- Bhore Committee (1946): Laid guidelines for national health planning
- Alma-Ata Declaration: Made primary health care the central function and main focus of the national health system
- National Health Policy (1983 & 2002): Guided approach for health sector in Five-Year Plans
- Goal: Health for All by the year 2000
Planning Commission (1950-2015)
- Set up in 1950 to assess material, capital, and human resources and draft development plans
- A Perspective Planning Division (1957) makes projections 20-25 years into the future
- Composition: Chairman, Deputy Chairman, 5 members
- Functions through: Programme Advisers, General Secretariat, and Technical Divisions
- Formulated successive Five-Year Plans
- Planning decentralised to Decentralised District Planning by 2000
NITI Aayog (2015-present)
- Replaced the Planning Commission on 1st January 2015
- Full form: National Institution for Transforming India
- Role: Strategic "think-tank" providing directional and technical advice to Central and State governments
- Also monitors and evaluates programme implementation; focuses on technology upgradation and capacity building
7. Health Sector Planning
The Planning Commission divided the health sector into the following sub-sectors:
- Water supply and sanitation
- Control of communicable diseases
- Medical education, training and research
- Medical care including hospitals, dispensaries, and primary health centres
- Family planning
- Other health activities
8. National Health Policy - 2017
The NHP 2017 was necessitated by four major contextual changes:
- Changing health priorities - declining maternal/child mortality but rising NCDs and some infectious diseases
- Growing health care industry - estimated at double-digit growth
- Catastrophic health expenditure - a major contributor to poverty
- Enhanced fiscal capacity due to rising economic growth
Primary Aim: To inform, clarify, strengthen and prioritize the Government's role in shaping health systems - including investments, healthcare organization, disease prevention, health promotion, technology access, human resources, medical pluralism, financial protection, regulation, and health assurance.
Specific Goals (Three Components)
A. Health Status and Programme Impact
- Reduce under-5 mortality to 23 per 1,000 live births by 2025
- Reduce infant mortality rate to 28 by 2019
- Reduce maternal mortality ratio to 100 per 100,000 live births by 2020
- Reduce total fertility rate to 2.1 by 2025
- Reduce prevalence of blindness to 0.25% by 2025
- Reduce premature mortality from cardiovascular disease, cancer, diabetes and chronic respiratory disease by 25% by 2025
B. Health Systems Performance
- Increase utilization of public health facilities by 50% from current levels by 2025
- Ensure availability of free essential drugs and diagnostics to all patients in public facilities by 2025
- Establish primary and secondary care facilities as per norms in high-priority districts by 2025
C. Health System Strengthening (Health Management Information)
- Ensure district-level electronic database of health system components by 2020
- Strengthen health surveillance systems and establish disease registries by 2020
- Establish federated integrated health information architecture and national health information network by 2025
Park's Textbook of Preventive and Social Medicine - Block 12, Chapter: Planning and Management
From parks Health Care of the Community
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from Park's. Here is the full structured write-up:
Health Care of the Community
Source: Park's Textbook of Preventive and Social Medicine
1. Definitions
Health Care
"A multitude of services rendered to individuals, families or communities by the agents of the health services or professions, for the purpose of promoting, maintaining, monitoring or restoring health."
- Health care includes medical care, but the two are NOT synonymous
- Medical care is a subset of health care - it refers specifically to personal services provided directly by physicians or rendered on their instructions (ranging from domiciliary to resident hospital care)
- In many countries, health care is completely or largely a government function
Community Health
- Defined (EURO Symposium, 1966): "All the personal health and environmental services in any human community, irrespective of whether such services were public or private"
- WHO (1973) cautioned that the term "community health" is ambiguous without further qualification, as it is sometimes used as a synonym for environmental health or community health care
Community Medicine
- Successor to: public health, preventive medicine, social medicine, and community health
- First formally referenced in the Todd Report (1968) by the Royal Commission on Medical Education
- Borrowed concepts, approaches, and methods from public health, preventive medicine, and social medicine
- Deals with health of populations and the organizational and administrative aspects of health care
Social Medicine
- Term introduced by Jules Guerin (French physician) in 1848
- Revived by Alfred Grotjahn (Berlin) in 1911, emphasizing social factors as determinants of health
- Defined by Professor Crew (Edinburgh): "Social medicine stands upon two pillars - medicine and sociology. It is concerned with the health of groups of individuals with a view to create, promote, preserve, and maintain optimum health. The laboratory is the whole community; the tools for diagnosis are epidemiology and biostatistics; and social therapy consists of social and political action for the betterment of conditions of life."
2. Characteristics of Health Care
A good health care system must have the following characteristics:
| Characteristic | Meaning |
|---|---|
| Appropriateness (Relevance) | Whether the service is needed at all in relation to essential human needs, priorities, and policies |
| Comprehensiveness | Whether there is an optimum mix of preventive, curative, and promotional services |
| Adequacy | Whether the service is proportionate to the requirement |
| Availability | Ratio between population and health facility (e.g., population per centre; doctor-population ratio) |
| Accessibility | Geographic, economic, or cultural accessibility |
| Affordability | Cost of health care should be within means of the individual and the state |
| Feasibility | Operational efficiency; logistic support; manpower and material resources |
3. The Health System
Definition: "The human and material resources that a nation or community deploys to preserve, protect, and restore health and to minimize suffering caused by disease and injury, and the corresponding administrative and organizational arrangements."
Components of a health system:
- Concepts: e.g., health and disease
- Ideas: e.g., equity, coverage, effectiveness, efficiency, impact
- Objects: e.g., hospitals, health centres, health programmes
- Persons: e.g., providers and consumers
Aim: Health development - a process of continuous and progressive improvement of the health status of a population.
4. Levels of Health Care
Health services are organized at three levels, each supported by a higher level to which patients are referred:
(a) Primary Health Care
- First level of contact between the individual and the health system
- "Essential" health care is provided here
- A majority of prevailing health problems can be satisfactorily dealt with at this level
- Closest to the people
- In India: provided by Primary Health Centres (PHCs) and sub-centres with community participation
(b) Secondary Health Care
- Deals with more complex problems
- Comprises essentially curative services
- Provided by district hospitals and Community Health Centres (CHCs)
- Serves as the first referral level in the health system
(c) Tertiary Health Care
- Offers super-specialist care
- Provided by regional/central level institutions (Medical College Hospitals)
- Provides: highly specialized care + planning/managerial skills + teaching for specialized staff
- Also supports and complements actions at the primary level
5. Primary Health Care (PHC)
Alma-Ata Declaration (1978)
PHC was defined at the International Conference in Alma-Ata, USSR (1978) as:
"Essential health care based on practical, scientifically sound and socially acceptable methods and technology made universally accessible to individuals and families in the community through their full participation and at a cost that the community and the country can afford to maintain at every stage of their development in the spirit of self-determination."
Principles of PHC:
- Social equity
- Nationwide coverage
- Self-reliance
- Intersectoral coordination
- People's involvement in planning and implementation
PHC approach = "Health by the people" and "placing people's health in people's hands"
Components of PHC (Alma-Ata Declaration)
- Education about prevailing health problems and their prevention and control
- Promotion of food supply and proper nutrition
- Adequate supply of safe water and basic sanitation
- Maternal and child health care, including family planning
- Immunization against infectious diseases
- Prevention and control of endemic diseases
- Appropriate treatment of common diseases and injuries
- Provision of essential drugs
Some countries have additionally included: mental health, physical handicaps, and health and social care of the elderly.
Obstacles to PHC in India:
- Shortage of health manpower
- Entrenchment of a curative culture within the existing health system
- High concentration of health services and personnel in urban areas
6. Health Promotion
Ottawa Charter (1986)
- First International Conference on Health Promotion, held in Ottawa, November 1986
- Built on the Alma-Ata Declaration and WHO discussions on intersectoral action
- Health promotion has a marked impact on determinants of health to: create the greatest health gain, reduce health inequities, and further human rights
- Ultimate goal: Increase health expectancy
Jakarta Declaration (1997)
- Fourth international conference on health promotion (July 1997)
- Identified fundamental conditions and resources for health: peace, shelter, education, social security, social relations, food, income, empowerment of women, a stable ecosystem, sustainable resource use, social justice, respect for human rights, and equity
- Above all, poverty is the greatest threat to health
7. Health for All (HFA)
- World Health Assembly (May 1977): Decided the main social goal of governments and WHO should be "the attainment by all people of the world by the year 2000 A.D. of a level of health that will permit them to lead a socially and economically productive life"
- Known as "Health for All by 2000" (HFA 2000)
- Primary health care was accepted by WHO member countries as the key to achieving HFA
8. The Health Team Concept
Definition: "A group of persons who share a common health goal and common objectives, determined by community members, and who work together to achieve them."
- Modern medicine is a joint effort of many groups: physicians, nurses, social workers, health assistants, ASHAs, and others
- Auxiliary worker = one who has less than full professional qualifications and is supervised by a professional; an essential team member
- The team must have a leader who evaluates, motivates, and stimulates team members
- Goal: produce the right "mix" of health personnel for providing full health coverage
- The mere presence of variety of health professionals is not sufficient - what matters is the proper division and combination of their operations
9. Hospitals and Community
WHO Definition of Hospital (1963):
"A residential establishment which provides short-term and long-term medical care consisting of observational, diagnostic, therapeutic and rehabilitative services for persons suffering or suspected to be suffering from a disease or injury and for parturients."
Criticism of hospitals:
- Exist in "splendid isolation" from the community - described as "an ivory tower of disease"
- Absorb 50 to 80% of the health budget
- Not people-oriented; procedures and styles are inflexible
- Overlooks cultural aspects of illness (treating the disease without treating the patient)
- Treatment is expensive; resistant to change
Dr. Rene Sand's Ideal: "The right patient should receive the right care at the right time in the right place at the right cost."
Modern trend: Redefine the hospital as a community health-oriented institution - not just disease-oriented, but with responsibilities in preventive medicine and health promotion. Primary health care requires effective hospital support for referred patients.
10. Community Health Centres (CHCs)
- As of 31st March 2017: 5,624 CHCs established across India
- Each CHC covers a population of 80,000 to 1.20 lakh (one per community development block)
- Beds: 30 beds
- Specialists: Surgery, Medicine, Obstetrics & Gynaecology, Paediatrics
- Facilities: X-ray and laboratory
- A Community Health Officer (non-medical) post has been created for preventive and promotive health care at each CHC
Indian Public Health Standards (IPHS) for CHCs
Services provided (Essential and Desirable):
| Service | Key Components |
|---|---|
| Surgery | Dressings, incision & drainage, hernia, hydrocele, appendicitis, haemorrhoids, fistula, wound stitching; emergencies: intestinal obstruction, haemorrhage; fracture reduction, plaster cast |
| Medicine | Dengue haemorrhagic fever, cerebral malaria, dog & snake bite, poisonings, CCF, LVF, pneumonia, meningoencephalitis, status epilepticus, burns, shock, acute dehydration; daily OPD |
| Maternal Health | 4 ANC check-ups; 24-hour delivery services (normal & assisted); Partograph use; management of PPH, eclampsia, sepsis; Caesar sections; post-natal care; Janani Suraksha Yojana |
Manpower at CHC (IPHS Revised Pattern)
Medical Staff (15-16 posts):
| Post | Number | Qualification |
|---|---|---|
| General Surgeon | 1 | MS/DNB |
| Physician | 1 | MD/DNB |
| Obstetrician & Gynaecologist | 1 | MD/DNB/DGO |
| Paediatrician | 1 | MD/DNB/DCH |
| Anaesthetist | 1 | MD/DNB/DA |
| Public Health Manager | 1 | MD (PSM)/MBA |
| Eye Surgeon | 1 (per 5 CHCs) | MS/DOMS/DNB |
| Dental Surgeon | 1 | BDS |
| General Duty Medical Officer | 6 (≥2 female) | MBBS |
| AYUSH Specialist | 1 | PG in AYUSH |
Support Manpower (64 posts): Staff nurses, ANM, PHN, pharmacists, lab technicians, radiographers, OT technicians, ward staff, and administrative personnel.
11. Functions of a Physician in the Community
A physician in India, soon after graduation, takes charge of a health centre (population 30,000) in a rural area. Functions include:
(a) Care of the individual:
- Clinical diagnosis, simple laboratory diagnosis
- Assessment of nutrition, level of development, social and emotional state, and health needs
(b) Care of the community:
- Epidemiological assessment; community diagnosis
- Promotive, preventive, curative, rehabilitative, and emergency care
- Special attention to vulnerable groups
Park's Textbook of Preventive and Social Medicine - Block 1 (Health Care, Levels, PHC, Community) & Block 12 (CHCs, IPHS)
Do u have fmt
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Forensic medicine
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Credits
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.