
17802699511305196501682287791689.jpg
Diagonise this image
Reading File
Finding Sources
Finding Sources
Searching PubMed
rectal cancer MRI staging pelvis
Reading File
Finding Sources
Loading Image
Finding Sources
I now have enough information to provide a thorough analysis. Here is the full interpretation:
MRI Pelvis - Radiological Analysis
Patient: Mr. Shrawan Kumar Kayeti | Age: 40 years (DOB: 31-May-1986) | Sex: Male
Scan date: 31-May-2026 | Sequence: T2 FSE Oblique Sagittal, 3mm slices | Protocol: MRI Pelvis with contrast
Key Findings on this T2-Weighted Sagittal MRI
1. Large Heterogeneous Pelvic Mass
There is a large, lobulated, heterogeneous soft-tissue mass occupying the mid-to-upper pelvis. It shows mixed T2 signal intensity - areas of intermediate signal interspersed with hyperintense foci - consistent with a neoplastic process. The mass is bulky and appears to arise from or closely involve the rectum/rectosigmoid region.
2. Rectal Wall Involvement
The mass clearly involves the rectal wall. The normal hypointense T2 rectal wall muscularis propria appears disrupted, with tumor signal extending beyond it - consistent with at minimum a T3 lesion (penetration through the rectal wall into mesorectal fat). Given the size and lobulated morphology, T4 invasion of adjacent structures cannot be excluded.
3. Relationship to Prostate and Seminal Vesicles
On this sagittal view, the mass lies immediately posterior and superior to the prostate. The plane of separation between the mass and the prostate/seminal vesicles is difficult to assess clearly, raising concern for T4b disease (invasion of adjacent organs). This is a critical finding that needs dedicated high-resolution axial T2 sequences to confirm.
4. Bladder
The urinary bladder (black signal - fluid-filled) is seen anteriorly. There is posterior bladder wall compression by the mass. Bladder wall invasion needs to be excluded on axial sequences.
5. Mesorectal Fat and Lymph Nodes
The mesorectal envelope appears expanded and infiltrated. Enlarged/irregular lymph nodes within the mesorectum would indicate N1-N2 disease - this sagittal slice does not allow complete nodal assessment but the mesorectal fat shows abnormal soft tissue.
6. Bowel / Proximal Obstruction
There is evidence of dilated bowel loops superiorly, which may indicate partial obstruction from the mass.
Impression / Most Likely Diagnosis
Locally Advanced Rectal Adenocarcinoma (cT3-T4b, probable N+)
This is the leading diagnosis based on:
- Large irregular rectal mass with wall disruption
- Extension into/beyond mesorectal fat
- Proximity to prostate with possible anterior invasion
- Patient age 40 (young but not atypical for rectal cancer; Lynch syndrome / FAP should be considered)
- Contrast-enhanced MRI protocol appropriate for rectal staging
Reference MRI Comparison (Sabiston Textbook)
Below is a textbook reference image of T3N1 rectal cancer for comparison - note the similar pattern of tumor penetrating the rectal wall with mesorectal lymphadenopathy:
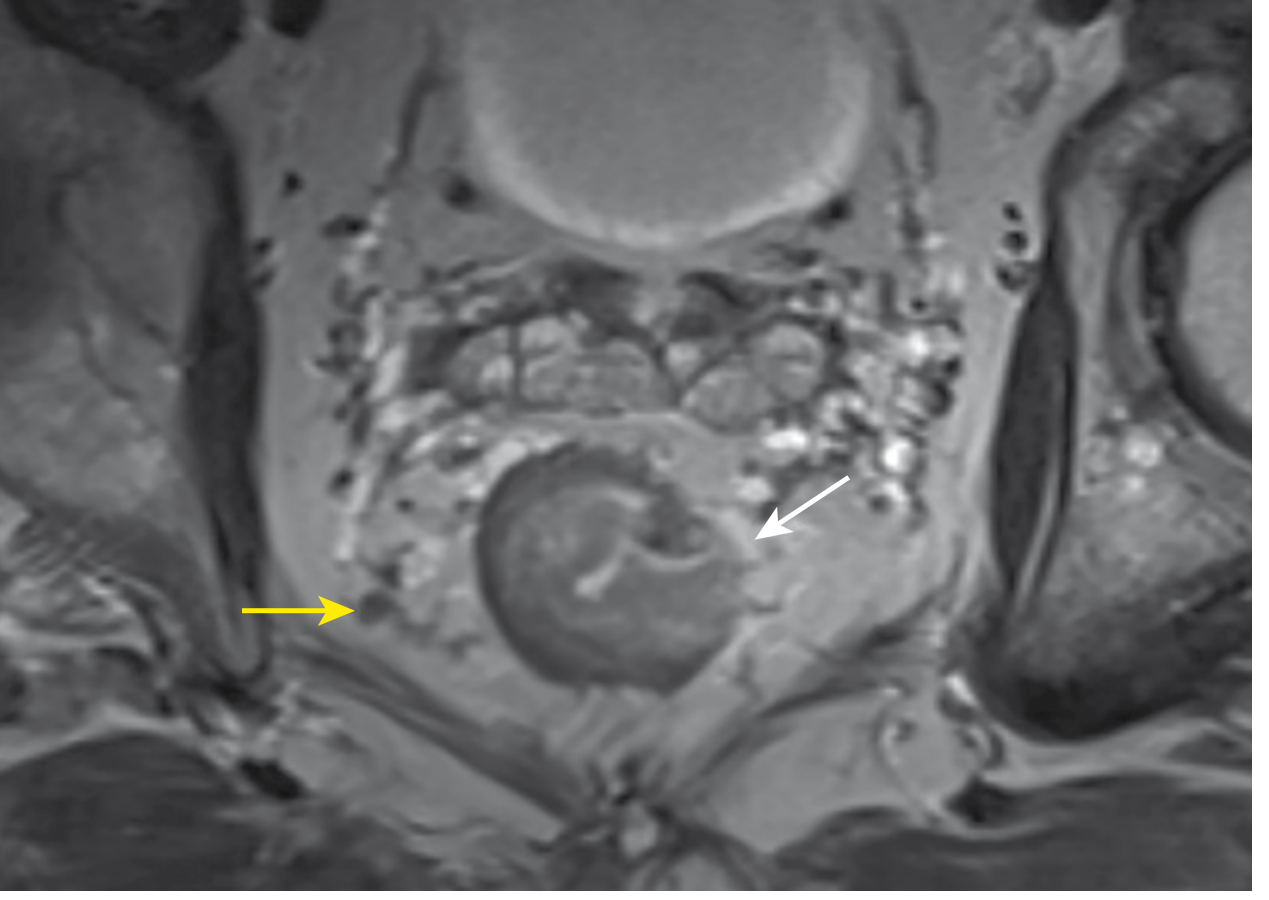
FIGURE 96.10 from Sabiston Textbook of Surgery: MRI pelvis showing a T3 tumor penetrating through the rectal wall into mesorectal fat (white arrow) with abnormal mesorectal adenopathy (yellow arrow), staged cT3N1.
Recommended Further Workup
| Investigation | Purpose |
|---|---|
| High-resolution axial T2 pelvis | Assess CRM (circumferential resection margin), prostate/bladder invasion |
| DWI sequences | Tumor characterisation and nodal staging |
| CT chest/abdomen/pelvis (contrast) | Distant metastasis staging (liver, lungs) |
| Colonoscopy | Confirm histology, assess synchronous lesions (~3% risk) |
| CEA level | Baseline tumour marker |
| MMR/MSI testing on biopsy | Lynch syndrome screening (important at age 40) |
| Multidisciplinary tumor board review | Standard of care per NAPRC guidelines |
Staging Summary (Provisional)
| Stage Element | Assessment |
|---|---|
| T stage | cT3 minimum; cT4b possible (prostate involvement) |
| N stage | Probable N+ (mesorectal soft tissue) |
| M stage | Unknown - CT staging needed |
| Overall | Likely Stage III (cIIIC) or potentially Stage IVA if distant mets present |
Clinical Implication
Per current guidelines (Sabiston/Bailey & Love/NCCN), locally advanced rectal cancer (T3/T4 or N+) is treated with neoadjuvant chemoradiotherapy (nCRT) or total neoadjuvant therapy (TNT) prior to surgical resection (low anterior resection or abdominoperineal resection), followed by adjuvant chemotherapy. Multidisciplinary tumor board discussion is mandatory before initiating treatment.
Disclaimer: This analysis is for educational and supportive purposes only. Final diagnosis and clinical management must be made by a qualified radiologist and the treating surgical/oncology team using the full imaging dataset and clinical context.
- Sabiston Textbook of Surgery, p. 2134 (Fig. 96.10)
- Bailey and Love's Short Practice of Surgery 28th Ed., Chapter on Rectal Cancer Staging
This is a shared conversation. Sign in to Orris to start your own chat.