
57623FB7-676A-4D9F-8BFA-5EA9EA73D53D.jpeg
??
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
Here is a detailed analysis of the X-ray:
Lateral Cervical Spine X-Ray - Analysis
Patient: Mrs. Mamta | Date: 31/05/2026 | Facility: Digital X-Ray, Shujalpur, Mandi M.P. | View: LAT (Lateral)
What I can observe on this X-ray:
1. Loss of Normal Cervical Lordosis
The most prominent finding is a straightening (loss) of the normal cervical lordosis. Normally, the cervical spine has a gentle forward curve (lordosis). In this film, the spine appears relatively straight or mildly kyphotic. This is a classic sign of:
- Cervical muscle spasm (most common acute cause)
- Cervical spondylosis / degenerative disc disease
- Poor positioning during imaging (though less likely here)
2. Intervertebral Disc Spaces
The disc spaces in the mid-lower cervical region (roughly C4-C7) appear reduced in height, suggesting disc degeneration. Disc space narrowing is a hallmark of cervical spondylosis.
3. Vertebral Bodies
There are suggestions of hypertrophic/osteophytic changes at the vertebral endplates (anterior osteophytes), consistent with degenerative disease. This is common in females in the perimenopausal/postmenopausal age group.
4. Upper Cervical Spine (C1-C2)
The atlanto-axial region (C1/C2) appears unremarkable at this resolution - no gross instability or atlantoaxial subluxation is visible.
5. Prevertebral Soft Tissues
The prevertebral soft tissue shadow appears within normal limits - no obvious swelling or retropharyngeal mass.
Reference: The 5 Lines to Check on a Lateral Cervical X-Ray
Using the standard approach from Miller's Review of Orthopaedics:
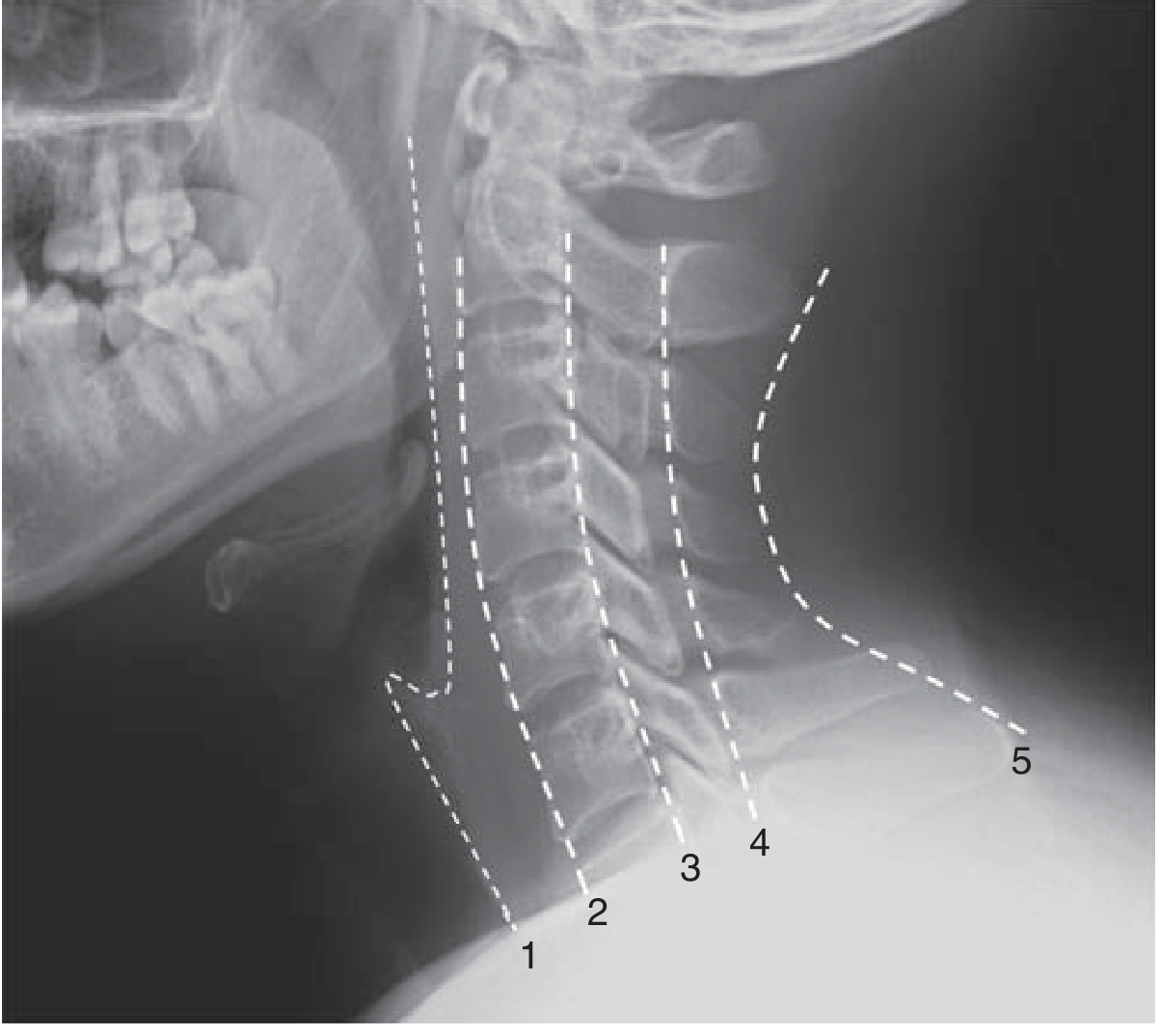
| Line | Structure | What to Check |
|---|---|---|
| 1 | Prevertebral soft tissue | Swelling = retropharyngeal pathology |
| 2 | Anterior vertebral line | Fracture/subluxation |
| 3 | Posterior vertebral line | Alignment |
| 4 | Spinolaminar line | Canal diameter (normal ≥14 mm) |
| 5 | Spinous process line | Posterior element integrity |
Canal diameter is measured between lines 3 and 4. A diameter <14 mm raises concern for stenosis; <10 mm = absolute stenosis.
Likely Radiological Impression:
Cervical spondylosis with loss of normal lordosis, most likely involving C4-C7 level. The findings are consistent with:
- Degenerative disc disease (cervical spondylosis)
- Muscle spasm causing cervical straightening
- Age-related changes
Clinical Correlation Needed:
Symptoms to correlate with:
- Neck pain / axial pain - discogenic, most common
- Radiculopathy - numbness/tingling/pain in arm (suggests nerve root compression at C5-C6 or C6-C7, the most commonly affected levels)
- Myelopathy - if spinal cord compression - requires MRI to evaluate
Recommended next step: MRI cervical spine if the patient has neurological symptoms, as plain X-rays cannot assess the spinal cord, nerve roots, or disc herniation directly. MRI will define any cord or root compression that may need treatment.
Disclaimer: This analysis is for educational/informational purposes only. It is not a formal radiological report and does not replace assessment by a qualified radiologist or treating physician. Clinical correlation and expert interpretation are mandatory before any treatment decisions.
Pt had sign of vertigo + vomiting
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Excellent - the textbook content is directly relevant. Here is the full clinical correlation:
Clinical Correlation: Vertigo + Vomiting with Cervical Spondylosis
The Connection - Cervical Vertigo / Vertebrobasilar Insufficiency
Given Mrs. Mamta's X-ray showing loss of cervical lordosis + disc space narrowing (cervical spondylosis), her symptoms of vertigo and vomiting fit into a well-recognized clinical syndrome.
Mechanism (Why Vertigo Occurs in Cervical Spondylosis)
There are two main proposed mechanisms:
1. Vertebral Artery Compression / Ischemia
Osteophytes and degenerative changes compress or irritate the vertebral arteries (which run through the C1-C6 transverse foramina). This causes transient ischemia to the vestibular nuclei, brainstem, and cerebellum - producing vertigo.
2. Sympathetic Plexus Irritation (Barre-Lieou Theory)
Spondylosis irritates the periarterial sympathetic neural plexus around the vertebral and basilar arteries, causing vasospasm and temporary ischemia - triggering vertigo.
3. Proprioceptive Dysfunction
Loss of normal neck proprioception from degenerate cervical joints disrupts the vestibulo-cervical reflex, causing a sense of imbalance.
Vertebrobasilar Insufficiency (VBI) - Key Symptoms to Check
From K.J. Lee's Essential Otolaryngology:
| Symptom | Present in Mrs. Mamta? |
|---|---|
| Vertigo | YES |
| Nausea & vomiting (vagal response) | YES |
| Headache (occipital) | Ask patient |
| Visual symptoms (flashing lights) | Ask patient |
| Tinnitus / hearing loss (low freq) | Ask patient |
| Syncope / drop attacks | Ask patient |
| Symptoms triggered by neck position change | Very likely - ask |
"Drop attacks without loss of consciousness, precipitated by neck motion, are characteristic of vertebrobasilar insufficiency." - K.J. Lee's Essential Otolaryngology
Differential Diagnoses to Consider
| Diagnosis | Key Features |
|---|---|
| Cervical vertigo / VBI | Most likely given X-ray + symptoms |
| BPPV (Benign Paroxysmal Positional Vertigo) | Positional, brief episodes, Dix-Hallpike positive |
| Vestibular neuronitis | Sudden onset, no cochlear symptoms, spontaneous nystagmus |
| Meniere's disease | Triad: vertigo + tinnitus + hearing loss |
| Central cause (posterior fossa) | Must rule out - needs MRI if neurological signs |
Recommended Investigations
- MRI Cervical Spine - assess cord/nerve root compression, vertebral artery patency
- MRI/MRA Brain (posterior fossa + vertebrobasilar system) - rule out posterior fossa lesion, VBI
- Dix-Hallpike test - rule out BPPV at bedside
- ENG/Videonystagmography - objective vestibular function assessment
- Audiometry - if hearing symptoms present
- Blood pressure both arms - rule out subclavian steal (>20 mmHg difference is significant)
Management
Immediate / Symptomatic:
- Vestibular suppressants: Betahistine (16 mg TDS) - improves labyrinthine microcirculation
- Anti-emetics: Prochlorperazine or Ondansetron for vomiting
- Diazepam (short-term) for acute severe vertigo
For Cervical Spondylosis (underlying cause):
- Cervical collar - immobilization temporarily reduces vertebral artery irritation
- Cervical traction (light horizontal traction, a few pounds, several hours at a time)
- Physiotherapy - neck exercises, posture correction, heat massage
- NSAIDs / muscle relaxants for associated neck pain and spasm
- Avoid sudden neck rotation and hyperextension - these can precipitate vertebrobasilar ischemia
If symptoms persist or MRI shows significant cord/artery compromise:
- Neurosurgery/spine surgery referral for decompression
Important Red Flags requiring urgent referral: New neurological deficits (limb weakness, speech disturbance, diplopia, dysphagia), sudden severe headache, or drop attacks suggest possible posterior circulation TIA/stroke - refer immediately to neurology/emergency.
Disclaimer: This is educational information only. Treatment decisions must be made by the treating physician based on full clinical assessment.
This is a shared conversation. Sign in to Orris to start your own chat.