Other methods of approximation of wound other then sutures with images I.E stapplers ,glues
wound closure methods staplers tissue glue steri-strips alternatives to sutures with images
hair apposition technique wound closure scalp zipper wound closure device images
Wound Approximation Methods - Alternatives to Sutures
Comparison Table
| Method | Advantages | Disadvantages |
|---|---|---|
| Staples | Rapid application; low tissue reactivity; low cost; low needle-stick risk | Less meticulous closure; may interfere with CT/MRI; requires removal |
| Tissue adhesives | Fastest application; no removal needed; microbial barrier; patient comfort | Lower tensile strength; dehiscence on high-tension areas; cannot use on hands or in wet areas |
| Adhesive tapes | Least reactive; lowest infection rates; rapid; no needle-stick risk | Frequently fall off; highest dehiscence rate; cannot use in hair-bearing areas; cannot get wet |
| Hair apposition | Simple; low cost; no foreign body; no needle-stick risk | Scalp only; limited to non-gaping lacerations |
1. Skin Staples
- Evert and approximate skin edges manually or with forceps (an assistant helps)
- Align the center of the stapler over the center of the wound
- Squeeze the handle - the anvil automatically bends the staple to the correct configuration
- Leave a 2-3 mm gap between the crossbar and skin surface to prevent ischemia
- Remove with a staple remover in 7-10 days (face), 10-14 days (trunk/extremities)

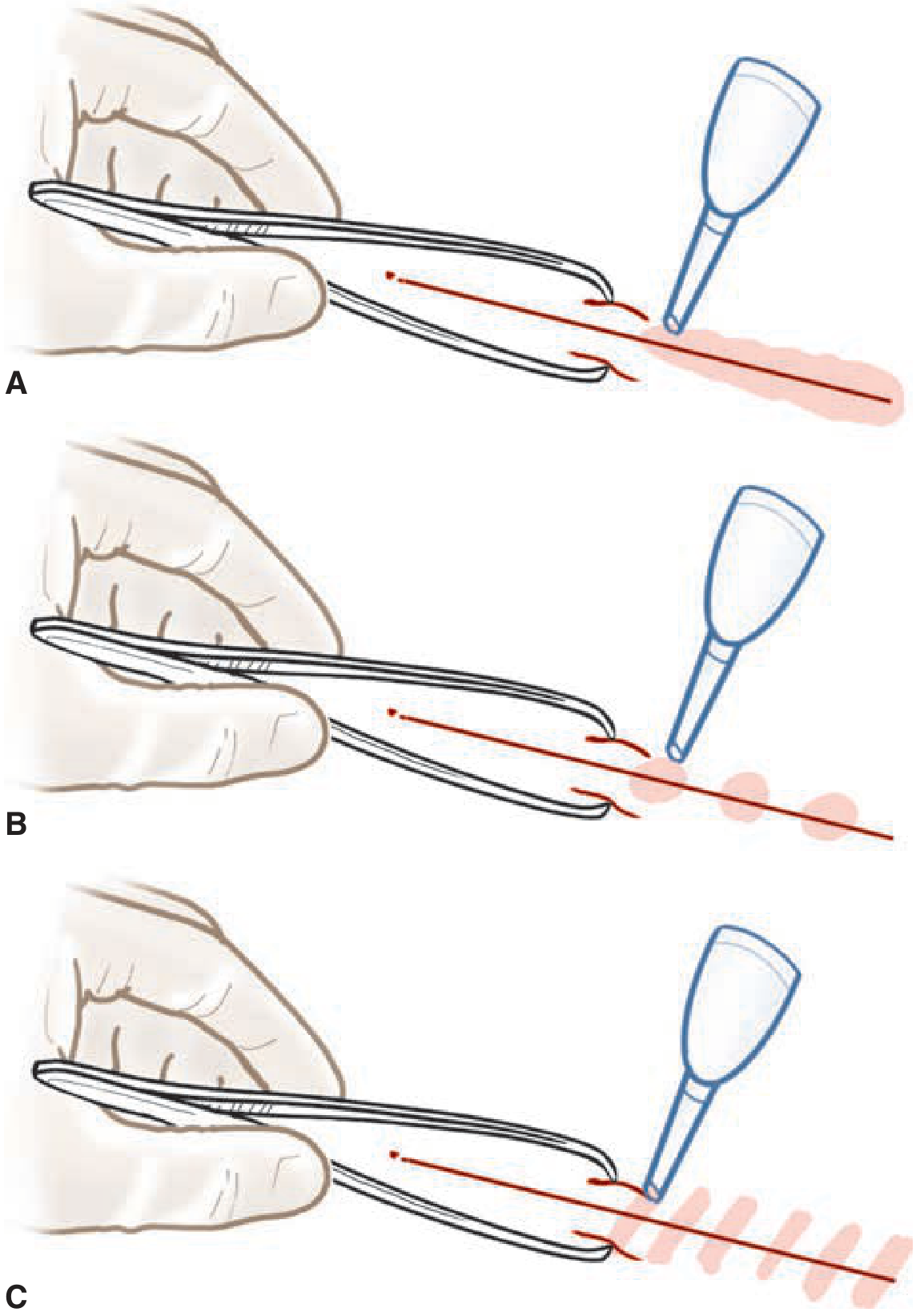
2. Cyanoacrylate Tissue Adhesives (Glues)
- Octyl-cyanoacrylate (Dermabond): stronger, more flexible, longer working time (2-3 min), no refrigeration needed, used for longer lacerations
- Butyl-cyanoacrylate (Histoacryl): faster set (5-10 s), lower bursting strength, requires refrigeration
- Fibrinogen-based (Tisseel) and hydrogel-based (Duraseal) - specialized uses
- Octyl-cyanoacrylate (A): Brush continuously along wound surface, parallel to wound edges, covering 5-10 mm on each side. Apply 1 layer, allow 30-45 sec to dry. Repeat 3-4 layers.
- Butyl-cyanoacrylate (B/C): Apply in discrete drops as "spot welds" or in bands across the wound.
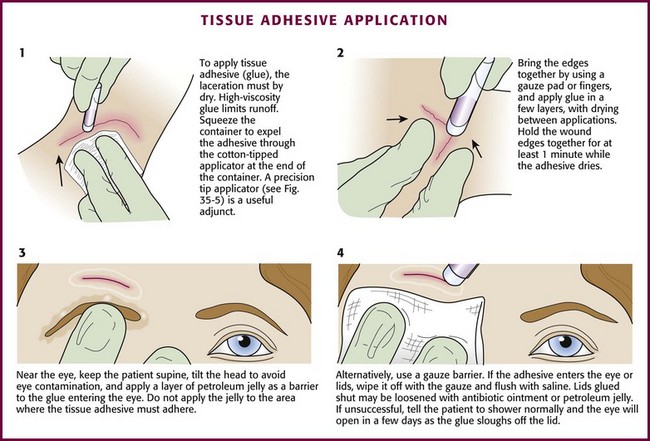
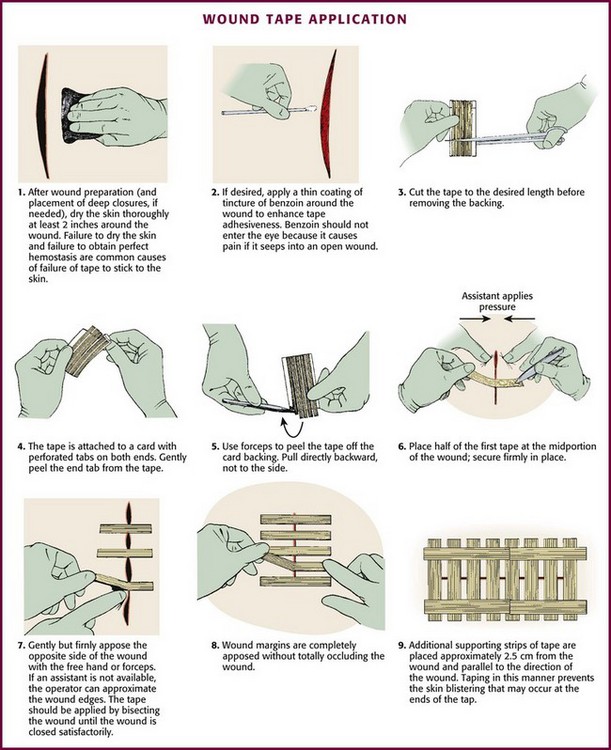
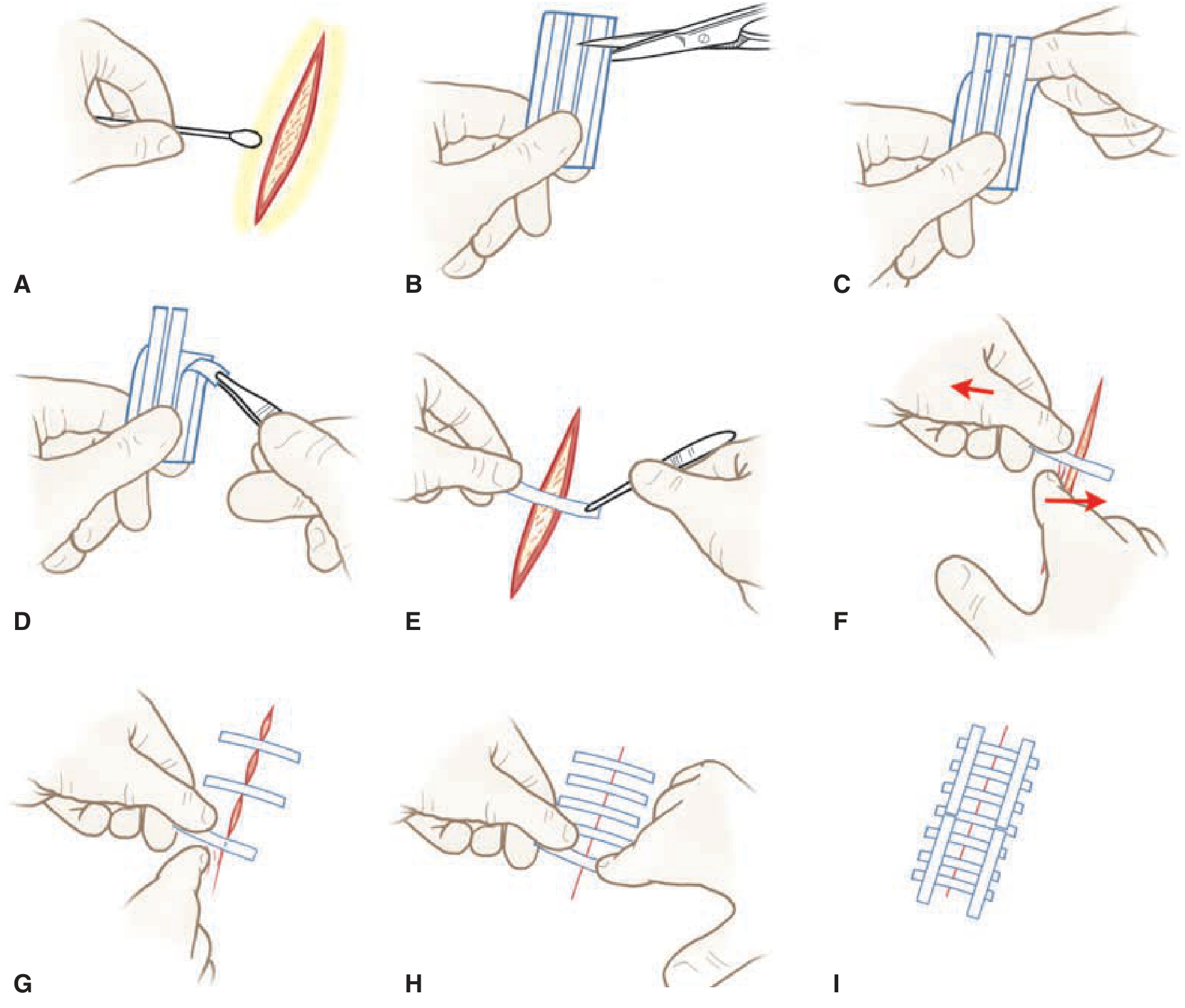
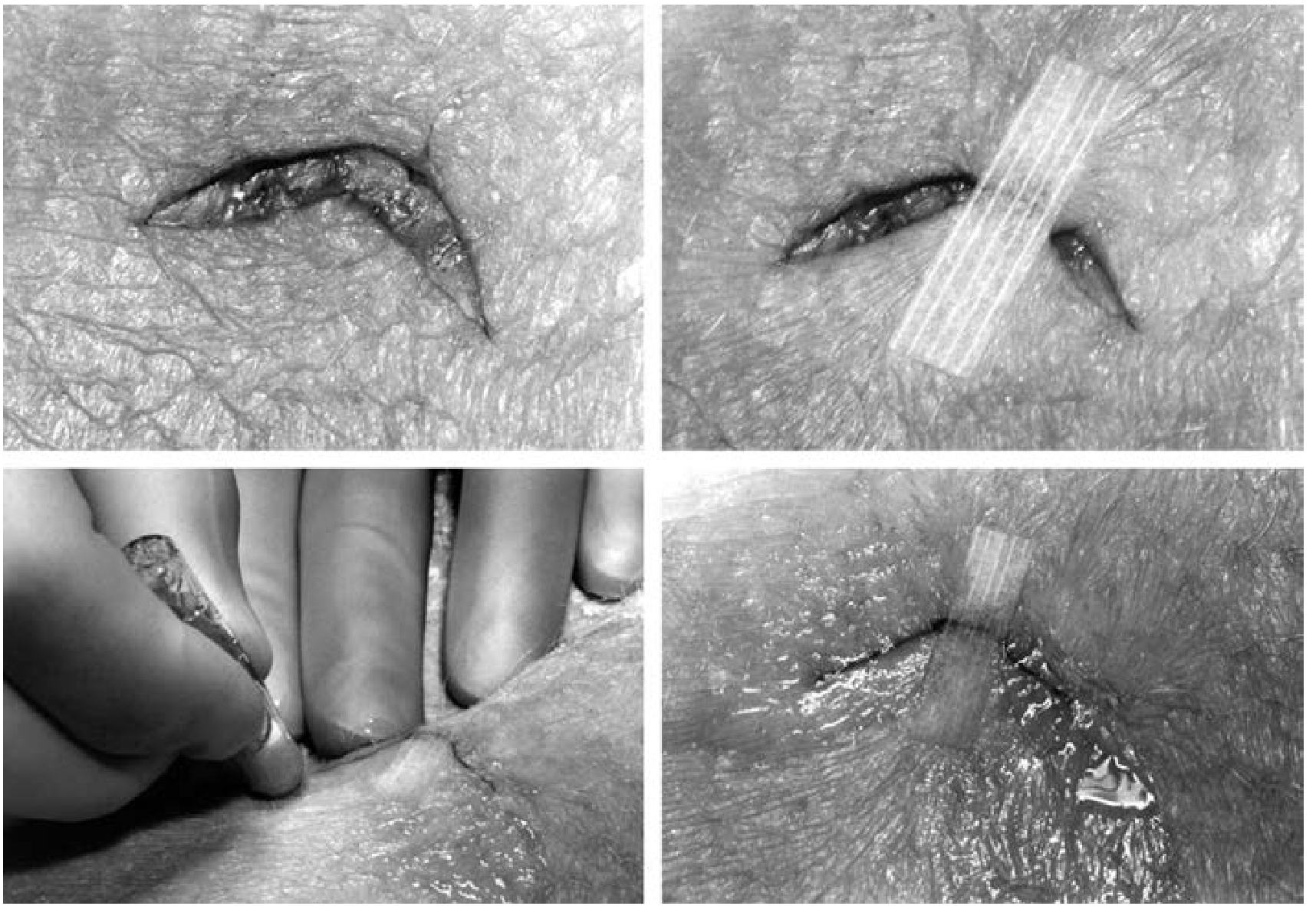
3. Adhesive Skin Tapes (Steri-Strips / Wound Closure Strips)
- Dry the skin thoroughly (key - moisture is the most common cause of failure)
- Optionally apply tincture of benzoin to adjacent skin to enhance adhesion (do not get benzoin in the wound)
- Cut tape to length; peel the end-tab off gently
- Secure half the tape to one side of the wound, appose edges, then secure to the opposite side
- Place strips perpendicular to the wound, 2-3 mm apart, using bisection technique
- Place additional parallel strips 2.5 cm from wound margins to prevent blistering
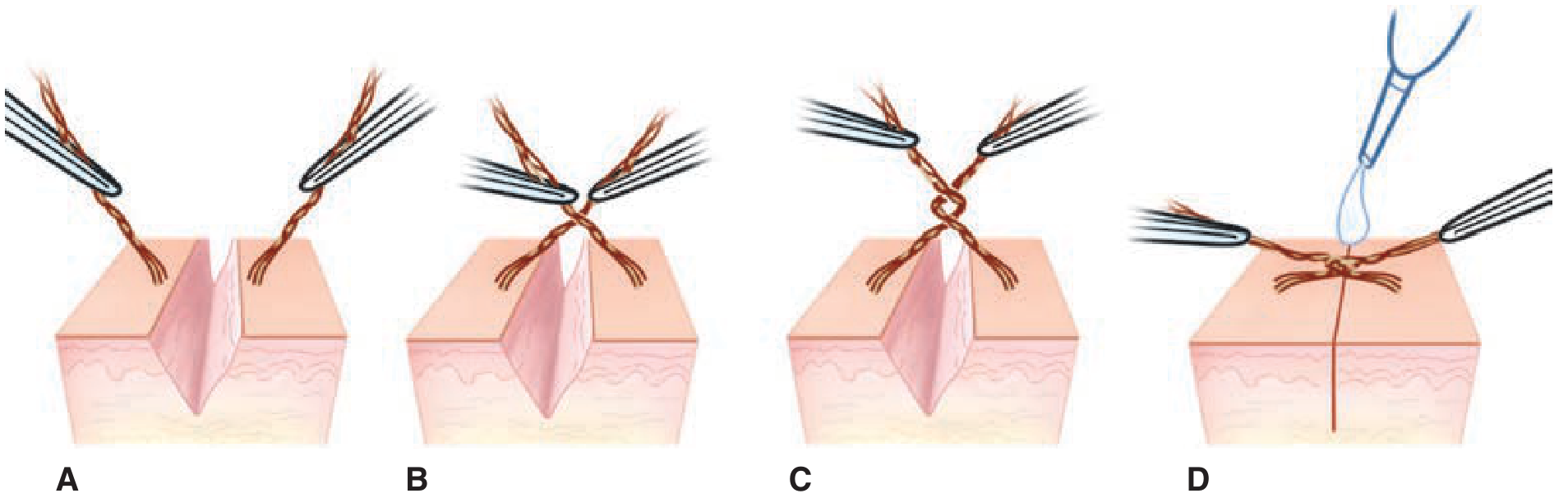
4. Hair Apposition Technique (HAT) - Scalp Only
- Irrigate wound and achieve hemostasis
- Twist 3-7 strands of hair on one side of the wound into a bundle
- Twist 3-7 strands on the opposite side into another bundle
- Cross-twist both bundles together through a full 360° revolution
- Apply a few drops of cyanoacrylate tissue adhesive to secure the intertwined bundle
- Repeat at intervals along the full laceration length

5. Wound Closure Clips (MicroMend)
6. Experimental / Emerging Methods
- Laser welding (Nd:YAG, CO₂ lasers): Fuses wound edges using thermal energy - still experimental, infrequently used clinically
- Photochemical welding (Rose Bengal + green light): Experimental technique crosslinking collagen using photoactivated dye
Decision Guide: How to Choose
| Clinical situation | Preferred method |
|---|---|
| High-tension wound | Sutures (or deep sutures + epidermal tape/adhesive) |
| Low-tension, linear facial lac | Tissue adhesive or fine sutures |
| Scalp laceration with adequate hair | Hair apposition (HAT) |
| Scalp/trunk/extremity linear lac | Staples (fastest) |
| Very superficial, well-apposed wound | Adhesive tape |
| Patient prone to keloid | Minimize foreign material → tapes or adhesive |
| Child, needle-phobic patient | Tissue adhesive |
| Post-suture/staple removal support | Adhesive tape reinforcement |
Sources: Tintinalli's Emergency Medicine (9th ed.), Dermatology 2-Volume Set (5th ed., Table 146.9), Roberts and Hedges' Clinical Procedures in Emergency Medicine
Make a ppt
mkdir -p /home/daytona/workspace/wound-closure-ppt && node /home/daytona/skills/shared/scripts/fetch_images.js \ "https://storage.googleapis.com/dl.dentistrykey.com/clinical/MethodsofWoundClosure/8_3s20B978032335478300035X.jpg" \ "https://veteriankey.com/wp-content/uploads/2016/09/B9781455706068000355_f035-pb004-9781455706068.jpg" \ "https://veteriankey.com/wp-content/uploads/2016/09/B9781455706068000355_f035-pb006-9781455706068.jpg" \ "https://cdn.orris.care/cdss_images/01692b368a392562168921406c9756c6284bd0c45393c5d7889a01c92ee309a0.png" \ "https://cdn.orris.care/cdss_images/e65906a7d12e790804a5c9387d60f16402d958e0d7d269f9ad549568d13d1c1c.png" \ "https://cdn.orris.care/cdss_images/7096b4f51a5832ba5af708481ebfbc01b87cd849886dee4ae5faed6056916a44.png" \ 2>/dev/null | node -e " const data = require('fs').readFileSync('/dev/stdin','utf8'); const imgs = JSON.parse(data); imgs.forEach((img,i) => { if(img.error) { console.log(i, 'ERROR', img.error); } else { console.log(i, 'OK', img.base64.substring(0,40)); } }); "
~/wound-closure-ppt/build.js
const pptxgen = require("pptxgenjs");
const { execSync } = require("child_process");
// ── Fetch all images ─────────────────────────────────────────────────────────
const imageUrls = [
"https://storage.googleapis.com/dl.dentistrykey.com/clinical/MethodsofWoundClosure/8_3s20B978032335478300035X.jpg", // 0 staples technique
"https://veteriankey.com/wp-content/uploads/2016/09/B9781455706068000355_f035-pb004-9781455706068.jpg", // 1 wound tape application
"https://veteriankey.com/wp-content/uploads/2016/09/B9781455706068000355_f035-pb006-9781455706068.jpg", // 2 tissue adhesive technique
"https://cdn.orris.care/cdss_images/01692b368a392562168921406c9756c6284bd0c45393c5d7889a01c92ee309a0.png", // 3 steri-strips application
"https://cdn.orris.care/cdss_images/e65906a7d12e790804a5c9387d60f16402d958e0d7d269f9ad549568d13d1c1c.png", // 4 hair apposition illustration
"https://cdn.orris.care/cdss_images/7096b4f51a5832ba5af708481ebfbc01b87cd849886dee4ae5faed6056916a44.png", // 5 cyanoacrylate application types
];
const imgRaw = execSync(
`node /home/daytona/skills/shared/scripts/fetch_images.js ${imageUrls.map(u => `"${u}"`).join(" ")}`
).toString();
const imgs = JSON.parse(imgRaw);
// ── Color palette ─────────────────────────────────────────────────────────────
const C = {
navy: "0D2B45", // dominant dark
teal: "1A7B74", // supporting
tealLight: "2AAFA6", // accent
cream: "F5F0E8", // light bg
white: "FFFFFF",
orange: "E8633A", // hot accent
gray: "6B7280",
lightGray: "D1D5DB",
darkText: "1A1A2E",
};
let pres = new pptxgen();
pres.layout = "LAYOUT_16x9"; // 10 x 5.625 inches
pres.author = "Medical Education";
pres.title = "Wound Approximation - Alternatives to Sutures";
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 1 — Title
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
// Full dark background
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.navy } });
// Teal accent bar left
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 0.12, h: 5.625, fill: { color: C.teal } });
// Orange accent bar top
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 0.08, fill: { color: C.orange } });
// Decorative teal circle (design element)
s.addShape(pres.ShapeType.ellipse, {
x: 7.2, y: 3.0, w: 4.0, h: 4.0,
fill: { color: C.teal, transparency: 80 },
line: { color: C.teal, transparency: 70, width: 1 },
});
// Subtitle tag
s.addShape(pres.ShapeType.rect, { x: 0.5, y: 1.5, w: 3.8, h: 0.35, fill: { color: C.orange } });
s.addText("WOUND MANAGEMENT", {
x: 0.5, y: 1.5, w: 3.8, h: 0.35,
fontSize: 10, bold: true, color: C.white, align: "center", valign: "middle", margin: 0,
});
// Main title
s.addText("Alternatives to Sutures", {
x: 0.5, y: 1.95, w: 8.5, h: 1.2,
fontSize: 44, bold: true, color: C.white, fontFace: "Calibri",
charSpacing: 1,
});
// Subtitle
s.addText("Wound Approximation Methods", {
x: 0.5, y: 3.1, w: 7, h: 0.5,
fontSize: 20, color: C.tealLight, fontFace: "Calibri",
});
// Methods list horizontal
s.addText("Staples · Tissue Adhesives · Adhesive Tapes · Hair Apposition · Clips", {
x: 0.5, y: 3.7, w: 9, h: 0.4,
fontSize: 12, color: C.lightGray, fontFace: "Calibri", italic: true,
});
// Source note
s.addText("Sources: Tintinalli's Emergency Medicine (9e) · Dermatology 5e", {
x: 0.5, y: 5.1, w: 9, h: 0.35,
fontSize: 9, color: C.gray, fontFace: "Calibri",
});
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 2 — Overview Comparison Table
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.cream } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 0.08, fill: { color: C.orange } });
// Section label
s.addShape(pres.ShapeType.rect, { x: 0.4, y: 0.18, w: 2.0, h: 0.3, fill: { color: C.navy } });
s.addText("OVERVIEW", { x: 0.4, y: 0.18, w: 2.0, h: 0.3, fontSize: 9, bold: true, color: C.white, align: "center", valign: "middle", margin: 0 });
s.addText("Methods at a Glance", {
x: 0.4, y: 0.55, w: 9.2, h: 0.55,
fontSize: 26, bold: true, color: C.navy, fontFace: "Calibri",
});
// Table
const tableData = [
[
{ text: "Method", options: { bold: true, color: C.white } },
{ text: "Tensile Strength", options: { bold: true, color: C.white } },
{ text: "Best For", options: { bold: true, color: C.white } },
{ text: "Removal?", options: { bold: true, color: C.white } },
{ text: "Key Limitation", options: { bold: true, color: C.white } },
],
["Skin Staples", "Highest", "Scalp, trunk, extremities under tension", "Yes (7–14 days)", "MRI/CT interference"],
["Tissue Adhesive", "Moderate", "Low-tension, facial, pediatric wounds", "No (sloughs off)", "Avoid high-tension & joints"],
["Adhesive Tapes", "Lowest", "Superficial, well-apposed, low-tension", "No (falls off)", "Cannot use in hair; moisture-sensitive"],
["Hair Apposition", "Moderate", "Scalp lacerations only", "No (unravels ~1 wk)", "Scalp only; hair ≥3 cm needed"],
["MicroMend Clips", "Moderate", "Modest-tension, well-apposed wounds", "No", "Limited evidence vs sutures"],
];
s.addTable(tableData, {
x: 0.4, y: 1.2, w: 9.2, h: 3.9,
fontSize: 10.5,
fontFace: "Calibri",
align: "left",
valign: "middle",
border: { pt: 0.5, color: C.lightGray },
colW: [1.6, 1.5, 2.8, 1.4, 1.9],
rowH: [0.45, 0.6, 0.6, 0.6, 0.6, 0.6],
fill: C.cream,
color: C.darkText,
autoPage: false,
});
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 3 — Skin Staples
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.white } });
// Left colored sidebar
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 0.08, h: 5.625, fill: { color: C.navy } });
// Header band
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 1.05, fill: { color: C.navy } });
// Number badge
s.addShape(pres.ShapeType.ellipse, { x: 0.25, y: 0.18, w: 0.65, h: 0.65, fill: { color: C.orange }, line: { color: C.orange } });
s.addText("1", { x: 0.25, y: 0.18, w: 0.65, h: 0.65, fontSize: 20, bold: true, color: C.white, align: "center", valign: "middle", margin: 0 });
s.addText("SKIN STAPLES", {
x: 1.0, y: 0.12, w: 5, h: 0.4,
fontSize: 22, bold: true, color: C.white, fontFace: "Calibri", charSpacing: 2,
});
s.addText("Fastest closure · Highest tensile strength · Low tissue reactivity", {
x: 1.0, y: 0.55, w: 8.5, h: 0.35,
fontSize: 11, color: C.tealLight, fontFace: "Calibri", italic: true,
});
// Image left
if (!imgs[0].error) {
s.addImage({ data: imgs[0].base64, x: 0.25, y: 1.15, w: 4.5, h: 3.9 });
}
// Content right
s.addText([
{ text: "Indications", options: { bold: true, color: C.navy, breakLine: true } },
{ text: "• Linear lacerations through the dermis", options: { breakLine: true } },
{ text: "• Scalp, trunk, extremity wounds under tension", options: { breakLine: true } },
{ text: "• Orthopedic & surgical incisions", options: { breakLine: true, color: C.gray } },
], { x: 5.0, y: 1.15, w: 4.7, h: 1.3, fontSize: 11, fontFace: "Calibri", color: C.darkText });
s.addShape(pres.ShapeType.rect, { x: 5.0, y: 2.5, w: 4.7, h: 0.02, fill: { color: C.lightGray } });
s.addText([
{ text: "Technique Key Points", options: { bold: true, color: C.navy, breakLine: true } },
{ text: "• Evert & appose edges before firing stapler", options: { breakLine: true } },
{ text: "• Align stapler center over wound center", options: { breakLine: true } },
{ text: "• Leave 2–3 mm gap between crossbar & skin", options: { breakLine: true } },
{ text: "• Remove at 7–10 days (face) / 10–14 days (trunk)", options: { breakLine: true } },
], { x: 5.0, y: 2.6, w: 4.7, h: 1.55, fontSize: 11, fontFace: "Calibri", color: C.darkText });
s.addShape(pres.ShapeType.rect, { x: 5.0, y: 4.2, w: 4.7, h: 0.02, fill: { color: C.lightGray } });
s.addShape(pres.ShapeType.rect, { x: 5.0, y: 4.28, w: 4.7, h: 0.55, fill: { color: "FFF3F0" }, line: { color: C.orange, pt: 1 } });
s.addText("⚠ Caution: Avoid staples near MRI/CT-scanned areas. Cosmetically inferior to sutures on the face.", {
x: 5.05, y: 4.3, w: 4.6, h: 0.5,
fontSize: 9.5, color: C.orange, fontFace: "Calibri", italic: true,
});
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 4 — Tissue Adhesives (Glues)
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.cream } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 1.05, fill: { color: C.teal } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 0.07, fill: { color: C.orange } });
s.addShape(pres.ShapeType.ellipse, { x: 0.25, y: 0.18, w: 0.65, h: 0.65, fill: { color: C.orange }, line: { color: C.orange } });
s.addText("2", { x: 0.25, y: 0.18, w: 0.65, h: 0.65, fontSize: 20, bold: true, color: C.white, align: "center", valign: "middle", margin: 0 });
s.addText("TISSUE ADHESIVES", {
x: 1.0, y: 0.12, w: 6, h: 0.4,
fontSize: 22, bold: true, color: C.white, fontFace: "Calibri", charSpacing: 2,
});
s.addText("Cyanoacrylate glues (Dermabond, Histoacryl) · No removal needed · Antimicrobial barrier", {
x: 1.0, y: 0.55, w: 8.7, h: 0.35,
fontSize: 11, color: "C8F0ED", fontFace: "Calibri", italic: true,
});
// Two images
if (!imgs[2].error) s.addImage({ data: imgs[2].base64, x: 0.2, y: 1.12, w: 4.8, h: 2.7 });
if (!imgs[5].error) s.addImage({ data: imgs[5].base64, x: 0.2, y: 3.87, w: 4.8, h: 1.6 });
// Right content
const boxStyle = { fill: { color: C.white }, line: { color: C.tealLight, pt: 1 } };
// Types box
s.addShape(pres.ShapeType.rect, { x: 5.2, y: 1.12, w: 4.5, h: 1.25, ...boxStyle });
s.addText([
{ text: "Types", options: { bold: true, color: C.teal, breakLine: true } },
{ text: "Octyl-cyanoacrylate (Dermabond): stronger, flexible, 2–3 min working time", options: { breakLine: true } },
{ text: "Butyl-cyanoacrylate (Histoacryl): faster set (5–10 s), needs refrigeration", options: { breakLine: true } },
{ text: "Fibrin glue (Tisseel), hydrogel (Duraseal): specialized internal use", options: {} },
], { x: 5.3, y: 1.17, w: 4.3, h: 1.15, fontSize: 10.5, fontFace: "Calibri", color: C.darkText });
// Indications box
s.addShape(pres.ShapeType.rect, { x: 5.2, y: 2.45, w: 4.5, h: 1.1, ...boxStyle });
s.addText([
{ text: "Indications", options: { bold: true, color: C.teal, breakLine: true } },
{ text: "• Low-tension wounds • Facial lacerations", options: { breakLine: true } },
{ text: "• Pediatric patients (needle anxiety)", options: { breakLine: true } },
{ text: "• Easily approximated wound edges", options: {} },
], { x: 5.3, y: 2.5, w: 4.3, h: 1.0, fontSize: 10.5, fontFace: "Calibri", color: C.darkText });
// Contraindications box
s.addShape(pres.ShapeType.rect, { x: 5.2, y: 3.63, w: 4.5, h: 1.1, fill: { color: "FFF3F0" }, line: { color: C.orange, pt: 1 } });
s.addText([
{ text: "Contraindications", options: { bold: true, color: C.orange, breakLine: true } },
{ text: "• High-tension wounds / over joints", options: { breakLine: true } },
{ text: "• Hands, mucous membranes, infected wounds", options: { breakLine: true } },
{ text: "• Cannot bathe or swim (brief shower OK)", options: {} },
], { x: 5.3, y: 3.68, w: 4.3, h: 1.0, fontSize: 10.5, fontFace: "Calibri", color: C.darkText });
// Note at bottom
s.addText("Sloughs off in 5–10 days · ~4% higher dehiscence than sutures · Comparable cosmetic outcomes for low-tension wounds", {
x: 0.2, y: 5.35, w: 9.6, h: 0.25,
fontSize: 8, color: C.gray, fontFace: "Calibri", align: "center",
});
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 5 — Adhesive Skin Tapes (Steri-Strips)
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.white } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 1.05, fill: { color: C.navy } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 0.07, fill: { color: C.teal } });
s.addShape(pres.ShapeType.ellipse, { x: 0.25, y: 0.18, w: 0.65, h: 0.65, fill: { color: C.orange }, line: { color: C.orange } });
s.addText("3", { x: 0.25, y: 0.18, w: 0.65, h: 0.65, fontSize: 20, bold: true, color: C.white, align: "center", valign: "middle", margin: 0 });
s.addText("ADHESIVE SKIN TAPES", {
x: 1.0, y: 0.12, w: 6, h: 0.4,
fontSize: 22, bold: true, color: C.white, fontFace: "Calibri", charSpacing: 2,
});
s.addText("Steri-Strips · Lowest infection rate · Least tissue reactivity · Most cost-effective", {
x: 1.0, y: 0.55, w: 8.7, h: 0.35,
fontSize: 11, color: C.tealLight, fontFace: "Calibri", italic: true,
});
// Images
if (!imgs[1].error) s.addImage({ data: imgs[1].base64, x: 0.2, y: 1.12, w: 5.0, h: 3.85 });
if (!imgs[3].error) s.addImage({ data: imgs[3].base64, x: 0.2, y: 5.0, w: 5.0, h: 0.5 });
// Step by step technique
s.addText("Technique", { x: 5.3, y: 1.12, w: 4.4, h: 0.35, fontSize: 14, bold: true, color: C.navy, fontFace: "Calibri" });
const steps = [
["1", "Dry skin thoroughly (critical - moisture = failure)"],
["2", "Apply tincture of benzoin to adjacent skin (not in wound)"],
["3", "Cut tape to length; peel end-tab gently"],
["4", "Secure half-tape to one side, appose edges, secure opposite side"],
["5", "Place strips perpendicular to wound, 2–3 mm apart"],
["6", "Add parallel strips 2.5 cm from wound margins to prevent blistering"],
];
steps.forEach(([num, text], i) => {
const y = 1.55 + i * 0.58;
s.addShape(pres.ShapeType.ellipse, { x: 5.3, y: y + 0.05, w: 0.35, h: 0.35, fill: { color: C.teal }, line: { color: C.teal } });
s.addText(num, { x: 5.3, y: y + 0.05, w: 0.35, h: 0.35, fontSize: 10, bold: true, color: C.white, align: "center", valign: "middle", margin: 0 });
s.addText(text, { x: 5.72, y: y, w: 4.0, h: 0.45, fontSize: 10.5, fontFace: "Calibri", color: C.darkText, valign: "middle" });
});
s.addShape(pres.ShapeType.rect, { x: 5.3, y: 5.1, w: 4.4, h: 0.35, fill: { color: C.cream }, line: { color: C.lightGray, pt: 0.5 } });
s.addText("Also used after suture/staple removal as reinforcement", {
x: 5.35, y: 5.1, w: 4.3, h: 0.35, fontSize: 9.5, color: C.gray, fontFace: "Calibri", italic: true, valign: "middle",
});
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 6 — Hair Apposition Technique (HAT)
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.cream } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 1.05, fill: { color: "1B3A5C" } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 0.07, fill: { color: C.tealLight } });
s.addShape(pres.ShapeType.ellipse, { x: 0.25, y: 0.18, w: 0.65, h: 0.65, fill: { color: C.orange }, line: { color: C.orange } });
s.addText("4", { x: 0.25, y: 0.18, w: 0.65, h: 0.65, fontSize: 20, bold: true, color: C.white, align: "center", valign: "middle", margin: 0 });
s.addText("HAIR APPOSITION TECHNIQUE (HAT)", {
x: 1.0, y: 0.12, w: 8, h: 0.4,
fontSize: 22, bold: true, color: C.white, fontFace: "Calibri", charSpacing: 1,
});
s.addText("Scalp lacerations only · No needles · No removal visit needed · First described 2002 (Singapore RCT)", {
x: 1.0, y: 0.55, w: 8.7, h: 0.35,
fontSize: 11, color: "C8F0ED", fontFace: "Calibri", italic: true,
});
// Illustration image
if (!imgs[4].error) s.addImage({ data: imgs[4].base64, x: 0.2, y: 1.12, w: 5.5, h: 2.3 });
// Steps right side
s.addText("How to perform HAT", { x: 5.9, y: 1.12, w: 3.8, h: 0.35, fontSize: 14, bold: true, color: C.navy, fontFace: "Calibri" });
const hatSteps = [
"Irrigate wound & achieve hemostasis",
"Twist 3–7 hair strands on ONE side into a bundle",
"Twist 3–7 strands on OPPOSITE side into bundle",
"Cross-twist both bundles 360°",
"Apply cyanoacrylate drops to secure",
"Repeat along full laceration length",
];
hatSteps.forEach((step, i) => {
const y = 1.55 + i * 0.48;
s.addShape(pres.ShapeType.rect, { x: 5.9, y: y + 0.07, w: 0.3, h: 0.3, fill: { color: C.teal }, line: { color: C.teal } });
s.addText(`${i + 1}`, { x: 5.9, y: y + 0.07, w: 0.3, h: 0.3, fontSize: 9, bold: true, color: C.white, align: "center", valign: "middle", margin: 0 });
s.addText(step, { x: 6.27, y: y, w: 3.5, h: 0.44, fontSize: 10.5, fontFace: "Calibri", color: C.darkText, valign: "middle" });
});
// Contraindications bottom
s.addShape(pres.ShapeType.rect, { x: 0.2, y: 3.5, w: 5.5, h: 1.85, fill: { color: C.white }, line: { color: C.lightGray, pt: 0.5 } });
s.addText("Contraindications", { x: 0.35, y: 3.55, w: 4, h: 0.35, fontSize: 12, bold: true, color: C.orange, fontFace: "Calibri" });
s.addText([
{ text: "• Lacerations > 10 cm ", options: { breakLine: true } },
{ text: "• Grossly contaminated wounds ", options: { breakLine: true } },
{ text: "• Uncontrolled bleeding ", options: { breakLine: true } },
{ text: "• Wound gaping under tension ", options: { breakLine: true } },
{ text: "• Adjacent hair < 3 cm in length ", options: {} },
], { x: 0.35, y: 3.95, w: 5.2, h: 1.35, fontSize: 10.5, fontFace: "Calibri", color: C.darkText });
s.addShape(pres.ShapeType.rect, { x: 5.9, y: 4.55, w: 3.8, h: 0.75, fill: { color: "E6F7F6" }, line: { color: C.teal, pt: 1 } });
s.addText("Adhesive unravels in ~1 week.\nNo routine return visit needed.", {
x: 5.95, y: 4.57, w: 3.7, h: 0.7, fontSize: 10.5, fontFace: "Calibri", color: C.teal, italic: true, valign: "middle",
});
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 7 — Wound Closure Clips & Emerging Methods
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.white } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 1.05, fill: { color: C.navy } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 0.07, fill: { color: C.orange } });
s.addShape(pres.ShapeType.ellipse, { x: 0.25, y: 0.18, w: 0.65, h: 0.65, fill: { color: C.tealLight }, line: { color: C.tealLight } });
s.addText("5", { x: 0.25, y: 0.18, w: 0.65, h: 0.65, fontSize: 20, bold: true, color: C.white, align: "center", valign: "middle", margin: 0 });
s.addText("CLIPS & EMERGING METHODS", {
x: 1.0, y: 0.12, w: 7, h: 0.4,
fontSize: 22, bold: true, color: C.white, fontFace: "Calibri", charSpacing: 2,
});
s.addText("MicroMend device · Laser welding · Photochemical welding", {
x: 1.0, y: 0.55, w: 8.7, h: 0.35,
fontSize: 11, color: C.tealLight, fontFace: "Calibri", italic: true,
});
// MicroMend box
s.addShape(pres.ShapeType.rect, { x: 0.3, y: 1.15, w: 4.3, h: 2.6, fill: { color: C.cream }, line: { color: C.lightGray, pt: 1 } });
s.addShape(pres.ShapeType.rect, { x: 0.3, y: 1.15, w: 4.3, h: 0.45, fill: { color: C.teal } });
s.addText("MicroMend Wound Closure Device", { x: 0.35, y: 1.15, w: 4.2, h: 0.45, fontSize: 13, bold: true, color: C.white, valign: "middle" });
s.addText([
{ text: "• Metal microclips embedded in adhesive bandage", options: { breakLine: true } },
{ text: "• OTC available for consumer use", options: { breakLine: true } },
{ text: "• For well-apposed wounds under modest tension", options: { breakLine: true } },
{ text: "• No anesthesia required", options: { breakLine: true } },
{ text: "• Useful where sutures are impractical", options: {} },
], { x: 0.45, y: 1.68, w: 4.05, h: 2.0, fontSize: 11, fontFace: "Calibri", color: C.darkText });
// Laser welding box
s.addShape(pres.ShapeType.rect, { x: 4.85, y: 1.15, w: 4.85, h: 1.2, fill: { color: C.cream }, line: { color: C.lightGray, pt: 1 } });
s.addShape(pres.ShapeType.rect, { x: 4.85, y: 1.15, w: 4.85, h: 0.45, fill: { color: "1B3A5C" } });
s.addText("Laser Welding", { x: 4.9, y: 1.15, w: 4.75, h: 0.45, fontSize: 13, bold: true, color: C.white, valign: "middle" });
s.addText([
{ text: "• Nd:YAG or CO₂ laser fuses wound edges thermally", options: { breakLine: true } },
{ text: "• Currently experimental · Infrequent clinical use", options: {} },
], { x: 4.95, y: 1.68, w: 4.65, h: 0.6, fontSize: 11, fontFace: "Calibri", color: C.darkText });
// Photochemical welding box
s.addShape(pres.ShapeType.rect, { x: 4.85, y: 2.45, w: 4.85, h: 1.3, fill: { color: C.cream }, line: { color: C.lightGray, pt: 1 } });
s.addShape(pres.ShapeType.rect, { x: 4.85, y: 2.45, w: 4.85, h: 0.45, fill: { color: "1B3A5C" } });
s.addText("Photochemical Welding", { x: 4.9, y: 2.45, w: 4.75, h: 0.45, fontSize: 13, bold: true, color: C.white, valign: "middle" });
s.addText([
{ text: "• Rose Bengal dye + green light → crosslinks collagen", options: { breakLine: true } },
{ text: "• No heat damage, minimal scarring potential", options: { breakLine: true } },
{ text: "• Experimental stage only", options: {} },
], { x: 4.95, y: 2.98, w: 4.65, h: 0.7, fontSize: 11, fontFace: "Calibri", color: C.darkText });
// Bottom divider
s.addShape(pres.ShapeType.rect, { x: 0.3, y: 3.9, w: 9.4, h: 0.04, fill: { color: C.lightGray } });
s.addText("Key principle: Emerging techniques aim to minimize scarring and foreign body response while maintaining wound tensile strength.", {
x: 0.3, y: 4.0, w: 9.4, h: 0.6,
fontSize: 11, fontFace: "Calibri", color: C.gray, italic: true,
});
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 8 — Decision Guide
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.cream } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 0.07, fill: { color: C.teal } });
// Header
s.addShape(pres.ShapeType.rect, { x: 0.3, y: 0.15, w: 2.2, h: 0.32, fill: { color: C.navy } });
s.addText("DECISION GUIDE", { x: 0.3, y: 0.15, w: 2.2, h: 0.32, fontSize: 9, bold: true, color: C.white, align: "center", valign: "middle", margin: 0 });
s.addText("How to Choose the Right Method", {
x: 0.3, y: 0.52, w: 9.4, h: 0.55,
fontSize: 26, bold: true, color: C.navy, fontFace: "Calibri",
});
const decisions = [
{ clin: "High-tension wound", method: "Deep sutures + epidermal closure of choice", color: C.orange },
{ clin: "Low-tension facial / cosmetic area", method: "Tissue adhesive or fine sutures", color: C.teal },
{ clin: "Scalp with sufficient hair (≥3 cm)", method: "Hair Apposition Technique (HAT)", color: C.teal },
{ clin: "Scalp / trunk / extremity linear", method: "Skin staples (fastest)", color: C.navy },
{ clin: "Very superficial, well-apposed wound", method: "Adhesive tapes (Steri-Strips)", color: C.tealLight },
{ clin: "Keloid-prone patient", method: "Minimize foreign material → tapes or adhesive", color: "1B3A5C" },
{ clin: "Child / needle-phobic patient", method: "Tissue adhesive", color: C.teal },
{ clin: "After suture/staple removal", method: "Adhesive tape reinforcement", color: C.tealLight },
];
const colW = [4.3, 4.9];
decisions.forEach((d, i) => {
const row = i % 4;
const col = Math.floor(i / 4);
const x = 0.3 + col * 4.85;
const y = 1.18 + row * 1.05;
s.addShape(pres.ShapeType.rect, { x, y, w: colW[col], h: 0.95, fill: { color: C.white }, line: { color: C.lightGray, pt: 0.5 } });
s.addShape(pres.ShapeType.rect, { x, y, w: 0.07, h: 0.95, fill: { color: d.color } });
s.addText("CLINICAL SCENARIO", { x: x + 0.18, y: y + 0.05, w: colW[col] - 0.25, h: 0.2, fontSize: 7, bold: true, color: C.gray, fontFace: "Calibri" });
s.addText(d.clin, { x: x + 0.18, y: y + 0.22, w: colW[col] - 0.25, h: 0.28, fontSize: 10.5, bold: true, color: C.darkText, fontFace: "Calibri" });
s.addShape(pres.ShapeType.rect, { x: x + 0.18, y: y + 0.52, w: colW[col] - 0.25, h: 0.02, fill: { color: C.lightGray } });
s.addText(`→ ${d.method}`, { x: x + 0.18, y: y + 0.56, w: colW[col] - 0.25, h: 0.3, fontSize: 10, color: d.color, fontFace: "Calibri", bold: true });
});
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 9 — Summary / Closing
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.navy } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 0.07, fill: { color: C.orange } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 5.55, w: 10, h: 0.075, fill: { color: C.teal } });
// Decorative circles
s.addShape(pres.ShapeType.ellipse, { x: 7.5, y: -1, w: 4.5, h: 4.5, fill: { color: C.teal, transparency: 85 }, line: { color: C.teal, transparency: 80 } });
s.addShape(pres.ShapeType.ellipse, { x: -1.5, y: 3.5, w: 4.0, h: 4.0, fill: { color: C.tealLight, transparency: 85 }, line: { color: C.tealLight, transparency: 80 } });
s.addText("KEY TAKEAWAYS", {
x: 1.0, y: 0.35, w: 8, h: 0.4,
fontSize: 11, bold: true, color: C.orange, fontFace: "Calibri", charSpacing: 4,
});
const takeaways = [
{ icon: "✦", point: "No single closure method suits all wounds — match the method to the wound tension, location, and patient." },
{ icon: "✦", point: "Tissue adhesives and tapes are preferred for low-tension, facial, and pediatric wounds for comfort and speed." },
{ icon: "✦", point: "Staples offer the fastest, strongest closure for scalp, trunk, and extremity linear lacerations." },
{ icon: "✦", point: "HAT is an elegant needle-free option for scalp lacerations with adequate hair length." },
{ icon: "✦", point: "Cosmetic outcome depends more on technique and patient healing than on the device chosen." },
];
takeaways.forEach((t, i) => {
s.addText([
{ text: `${t.icon} `, options: { color: C.orange, bold: true } },
{ text: t.point, options: { color: C.white } },
], {
x: 0.8, y: 0.9 + i * 0.82, w: 8.5, h: 0.7,
fontSize: 12.5, fontFace: "Calibri",
});
});
s.addShape(pres.ShapeType.rect, { x: 0.8, y: 5.0, w: 8.5, h: 0.04, fill: { color: C.teal, transparency: 60 } });
s.addText("Sources: Tintinalli's Emergency Medicine (9e) · Dermatology 2-Volume Set (5e) · Roberts and Hedges' Clinical Procedures in Emergency Medicine", {
x: 0.8, y: 5.1, w: 8.5, h: 0.35,
fontSize: 8.5, color: C.gray, fontFace: "Calibri", align: "center",
});
}
// ── Write file ────────────────────────────────────────────────────────────────
pres.writeFile({ fileName: "/home/daytona/workspace/wound-closure-ppt/Wound_Closure_Alternatives.pptx" })
.then(() => console.log("DONE: /home/daytona/workspace/wound-closure-ppt/Wound_Closure_Alternatives.pptx"))
.catch(e => { console.error("ERROR:", e); process.exit(1); });
cd /home/daytona/workspace/wound-closure-ppt && node build.js 2>&1
cd /home/daytona/workspace/wound-closure-ppt && node -e " const { execSync } = require('child_process'); const fs = require('fs'); const urls = [ 'https://storage.googleapis.com/dl.dentistrykey.com/clinical/MethodsofWoundClosure/8_3s20B978032335478300035X.jpg', 'https://veteriankey.com/wp-content/uploads/2016/09/B9781455706068000355_f035-pb004-9781455706068.jpg', 'https://veteriankey.com/wp-content/uploads/2016/09/B9781455706068000355_f035-pb006-9781455706068.jpg', 'https://cdn.orris.care/cdss_images/01692b368a392562168921406c9756c6284bd0c45393c5d7889a01c92ee309a0.png', 'https://cdn.orris.care/cdss_images/e65906a7d12e790804a5c9387d60f16402d958e0d7d269f9ad549568d13d1c1c.png', 'https://cdn.orris.care/cdss_images/7096b4f51a5832ba5af708481ebfbc01b87cd849886dee4ae5faed6056916a44.png', ]; const results = []; for(const url of urls) { try { const raw = execSync(\`node /home/daytona/skills/shared/scripts/fetch_images.js \"\${url}\"\`, { maxBuffer: 20*1024*1024 }).toString(); const arr = JSON.parse(raw); results.push(arr[0]); } catch(e) { results.push({ url, base64: null, error: e.message }); } } fs.writeFileSync('images.json', JSON.stringify(results)); console.log('Saved', results.length, 'images, errors:', results.filter(r=>r.error).length); " 2>&1
~/wound-closure-ppt/build.js
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/wound-closure-ppt/build.js'
~/wound-closure-ppt/build.js
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/wound-closure-ppt/build.js'
cd /home/daytona/workspace/wound-closure-ppt && node build.js 2>&1
ls -lh /home/daytona/workspace/wound-closure-ppt/Wound_Closure_Alternatives.pptx
Wound Closure Alternatives
Presentation · PPTX
| Slide | Content |
|---|---|
| 1 | Title slide |
| 2 | Overview comparison table (all 5 methods side-by-side) |
| 3 | Skin Staples - technique steps + clinical image |
| 4 | Tissue Adhesives - types, indications, contraindications + technique images |
| 5 | Adhesive Skin Tapes (Steri-Strips) - 6-step technique + clinical images |
| 6 | Hair Apposition (HAT) - steps, contraindications + illustration |
| 7 | Wound Closure Clips & Emerging Methods (MicroMend, laser welding, photochemical welding) |
| 8 | Clinical Decision Guide (8 scenarios mapped to methods) |
| 9 | Key Takeaways summary |