Stargardth disease
Reading File
Finding Sources
Searching PubMed
Stargardt disease ABCA4
Reading File
Reading File
Reading File
Searching PubMed
Stargardt disease treatment gene therapy
Reading File
Reading File
Loading Image
Loading Image
Reading File
Here is a comprehensive overview of Stargardt disease based on authoritative ophthalmology textbooks.
Stargardt Disease (Fundus Flavimaculatus)
Overview
Stargardt disease (SD) — first described by Stargardt in 1909 — is the most common inherited macular dystrophy in both adults and children, and the leading cause of central visual loss in those under 50. Prevalence is approximately 1 in 8,000–10,000 people. Stargardt disease and fundus flavimaculatus (FFM) are regarded as variants of the same condition.
Genetics
Three genetic subtypes are recognized:
| Type | Inheritance | Gene | Notes |
|---|---|---|---|
| STGD1 | Autosomal recessive (AR) | ABCA4 (chromosome 1p) | Most common |
| STGD3 | Autosomal dominant (AD) | ELOVL4 | |
| STGD4 | Autosomal dominant (AD) | PROM1 |
The ABCA4 gene encodes a transporter protein (ABCR) in photoreceptors that normally facilitates recycling of the visual chromophore 11-cis-retinal. Mutations impair this process, causing toxic accumulation of lipofuscin (specifically A2E, a bisretinoid) in the retinal pigment epithelium (RPE), leading to RPE and photoreceptor death.
Pathophysiology
Defective ABCA4 → impaired 11-cis-retinal recycling → lipofuscin accumulation in RPE cells → RPE toxicity and death → progressive photoreceptor (mainly cone) loss → central visual impairment. This selective cone dysfunction makes it, in a sense, the inverse of retinitis pigmentosa.
Clinical Features
Symptoms
- Gradual central vision loss, typically onset in childhood or adolescence (ages 6–20), occasionally later
- Difficulty reading is a common complaint
- Importantly, early visual decline is often out of proportion to fundoscopic findings — patients, particularly children, may be incorrectly labeled as malingerers
- A quarter of childhood-onset STGD1 cases have no visible retinal lesions at presentation; OCT clarifies the diagnosis
Fundoscopic Signs (progressive)
- Normal-appearing fundus or non-specific foveal granularity/mottling
- Yellow-white pisciform (fish-shaped) flecks at the level of the RPE — may be confined to the posterior pole or extend to the mid-periphery
- "Snail-slime" maculopathy or "beaten-bronze/beaten-metal" paramacular appearance
- Atrophic macular degeneration — may have a bull's-eye configuration or geographic atrophy
- Occasionally: macular neovascularization (rare)
Fundus Photo — Characteristic Flecks
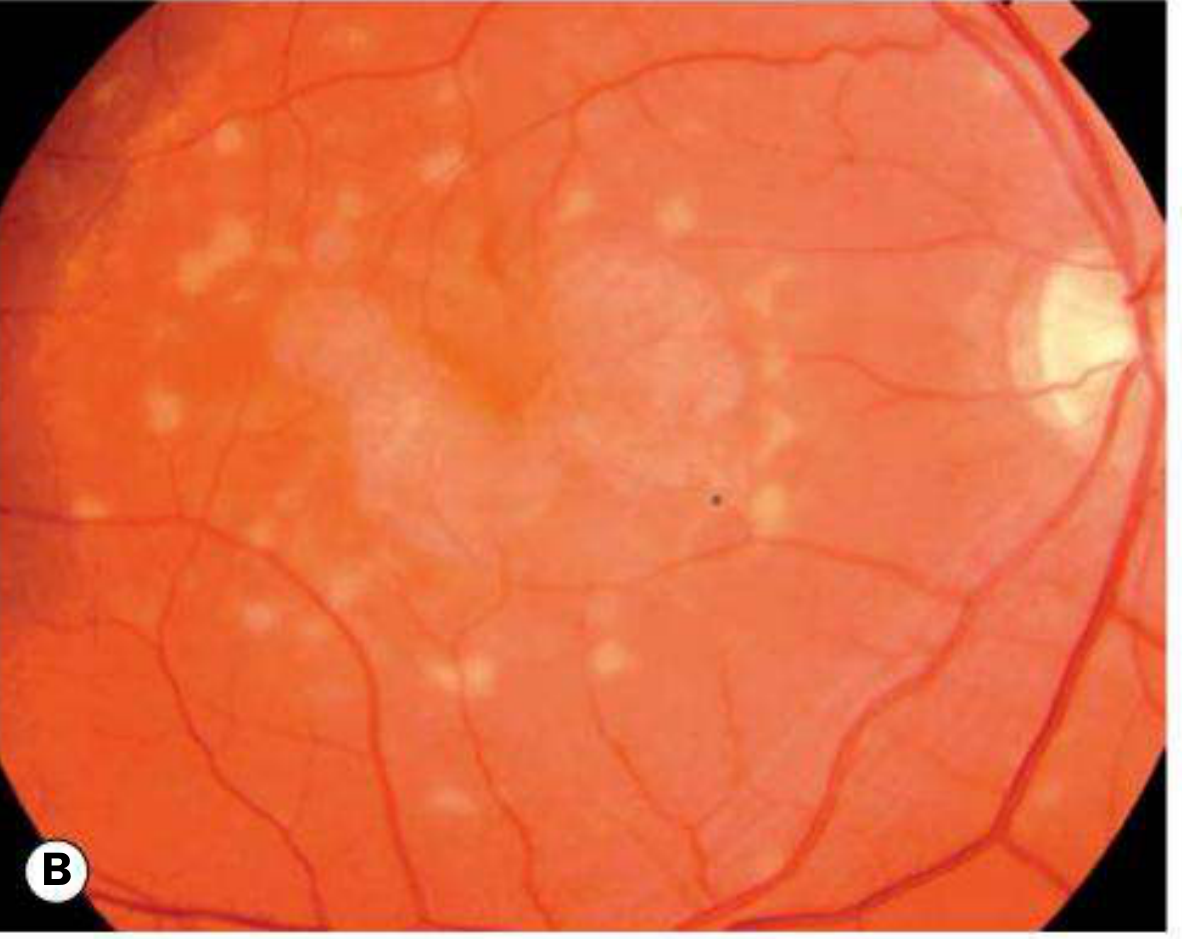
Fundus appearance showing scattered yellow-white flecks at the RPE level
Investigations
| Test | Finding |
|---|---|
| Fluorescein Angiography (FA) | Classic "dark choroid" / "silent choroid" — choroidal fluorescence is masked by lipofuscin in the RPE. Flecks show early hypofluorescence (blockage) and late hyperfluorescence (staining) |
| Fundus Autofluorescence (FAF) | Key diagnostic test — hyperautofluorescent flecks with macular hypoautofluorescence; hypoAF zones indicate RPE atrophy |
| OCT | Photoreceptor disorganization, outer retinal and RPE atrophy; may be abnormal even with a normal-looking fundus |
| ERG | Photopic (cone) ERG normal to subnormal early; may become abnormal late. Scotopic usually normal |
| EOG | Subnormal, especially in advanced disease |
| Visual fields | Central scotomata; peripheral fields typically normal |
| Genetic testing | ABCA4 sequencing confirms diagnosis in most cases |
FAF image — Stargardt disease
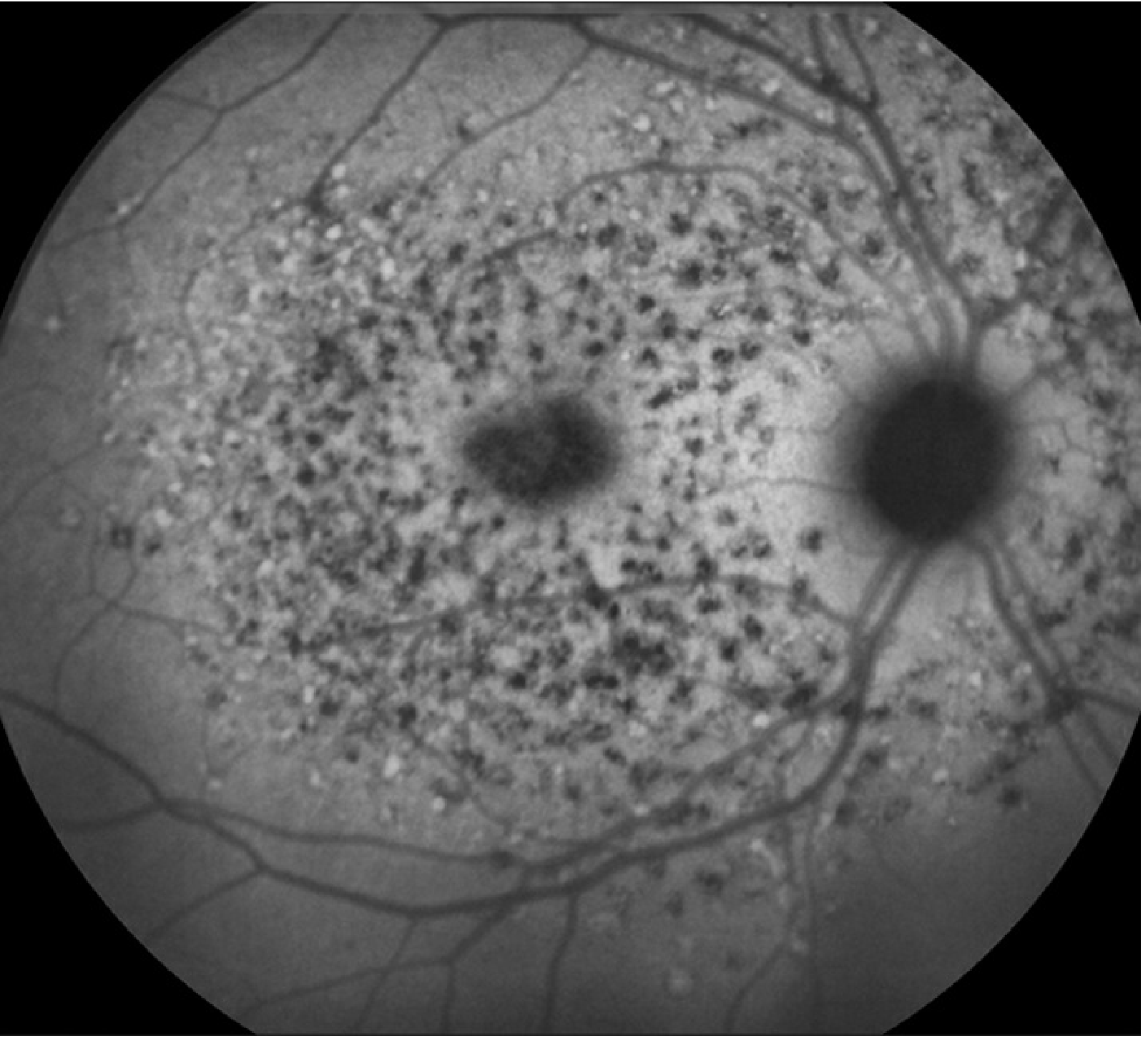
FAF showing the characteristic pattern: hyperautofluorescent flecks throughout the posterior pole with central hypoautofluorescence indicating RPE atrophy
Differential Diagnosis
- Fundus albipunctatus — stationary night blindness with discrete white dots; ERG normalizes after dark adaptation
- Retinitis punctata albescens — similar appearance but progressive; abnormal ERG
- Drusen — typically older patients; all lesions hyperfluorescent on FA
- Cone/cone-rod dystrophy — significant color vision deficit; characteristic ERG
- Chloroquine/hydroxychloroquine maculopathy — medication history
- Bull's-eye maculopathy (Batten disease, Spielmeyer-Vogt) — associated dementia/seizures
- Nonphysiologic visual loss — normal ERG, EOG, OCT
Prognosis
Poor. Once visual acuity drops below 6/12 (20/40), it tends to deteriorate rapidly. The peripheral retina is usually spared initially but can become dystrophic in late-stage disease.
Management
Current (Symptomatic)
- Avoid vitamin A supplementation — accelerates lipofuscin accumulation
- UV-blocking sunglasses — protect against light-induced RPE damage
- Low-vision aids and rehabilitation
- Genetic counseling
Emerging Therapies (Clinical Trials)
Active research areas include:
- Gene therapy — lentiviral vector delivery of ABCA4 (StarGen trial); recent large-animal studies using dual AAV intein vectors show safety and efficacy (Ferla et al., Sci Adv 2025)
- Stem cell therapy — RPE cell replacement
- Pharmacotherapy — reducing lipofuscin/A2E accumulation (e.g., visual cycle modulators)
- Metformin (oral) — under investigation for neuroprotective effects
- Base editing — high-efficiency genome editing approaches demonstrated in primate retina (Muller et al., Nat Med 2025)
Associations
Stargardt disease may be associated with:
- Epilepsy
- Refsum syndrome
- Kearns-Sayre syndrome
- Bassen-Kornzweig syndrome
- Sjögren-Larsson syndrome
- Spinocerebellar and other cerebellar degenerations
Sources: Kanski's Clinical Ophthalmology 10th Ed., p. 654–656 | Wills Eye Manual, p. 893–897 | Adams & Victor's Principles of Neurology 12th Ed.
⚠️ Recent evidence note (2025): Gene therapy using dual AAV intein vectors for STGD1 has shown safety and efficacy in large animal models (PMID: 40138422), and base editing approaches in primate retina are advancing rapidly (PMID: 39779923). These may update current clinical management guidelines in coming years.
Intra ocular foreign body management
Finding Sources
Searching PubMed
intraocular foreign body management outcomes
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Here is a comprehensive clinical overview of intraocular foreign body (IOFB) management.
Intraocular Foreign Body (IOFB) — Management
Introduction
An IOFB may damage the eye by:
- Mechanical injury — cataract formation from capsular injury, vitreous liquefaction, retinal hemorrhages and tears
- Infection — stones and organic matter carry a high risk; endophthalmitis develops in ~1 in 10 cases of penetrating trauma with retained IOFB
- Toxic effects — iron causes siderosis; copper causes chalcosis
IOFBs may lodge anywhere: anterior chamber, lens, vitreous, or retina.
Types of Foreign Bodies
| Category | Reactivity | Examples |
|---|---|---|
| Severely reactive | Violent endophthalmitis-like reaction | Pure copper (>85%), vegetable/organic matter |
| Moderately reactive | Significant inflammation | Iron, steel, tin (magnetic); nickel |
| Mildly reactive | Mild inflammation | Aluminum, mercury, zinc, vegetable matter |
| Inert | Minimal/no reaction | Glass, lead, gold, silver, carbon, coal, platinum, rubber, stone, porcelain, gypsum, brass/bronze |
⚠️ Even "inert" foreign bodies can be toxic due to coatings or chemical additives. Most BBs and gunshot pellets are 80–90% lead with 10–20% iron.
Clinical Presentation
Symptoms
- Eye pain, decreased vision — or may be completely asymptomatic
- Classic history: hammering metal on metal, power tool use, explosion, shrapnel, high-velocity projectile
Signs
- Visible corneal or scleral perforation site
- Hole in the iris (iris transillumination defect — TID)
- Focal lens opacity or embedded FB in lens
- Vitreous hemorrhage
- Microcystic (epithelial) edema of the peripheral cornea — clue to a hidden AC angle foreign body
- Long-standing iron IOFBs: anisocoria, heterochromia iridis, anterior subcapsular cataract, pigmentary retinopathy, optic atrophy (siderosis)
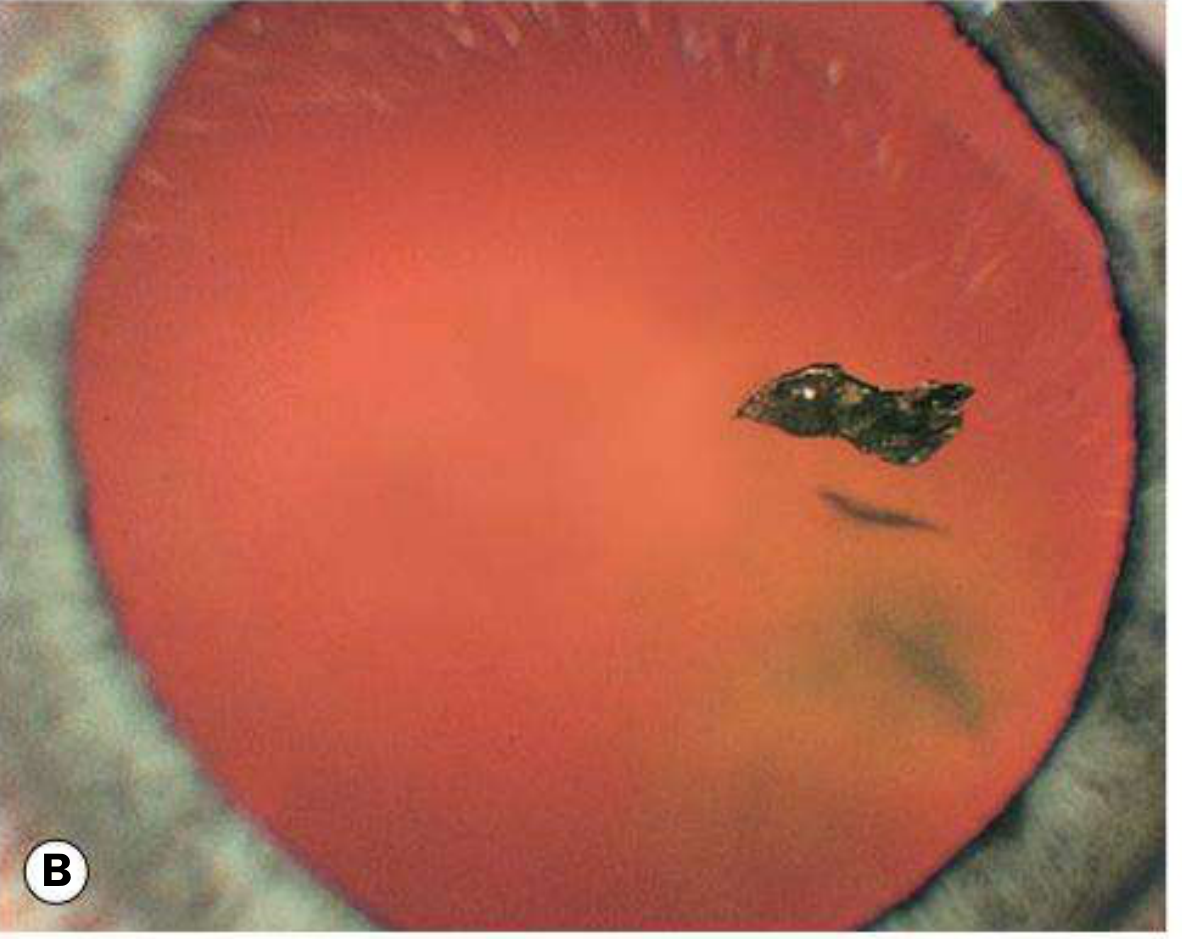
Clinical image — IOFB in vitreous
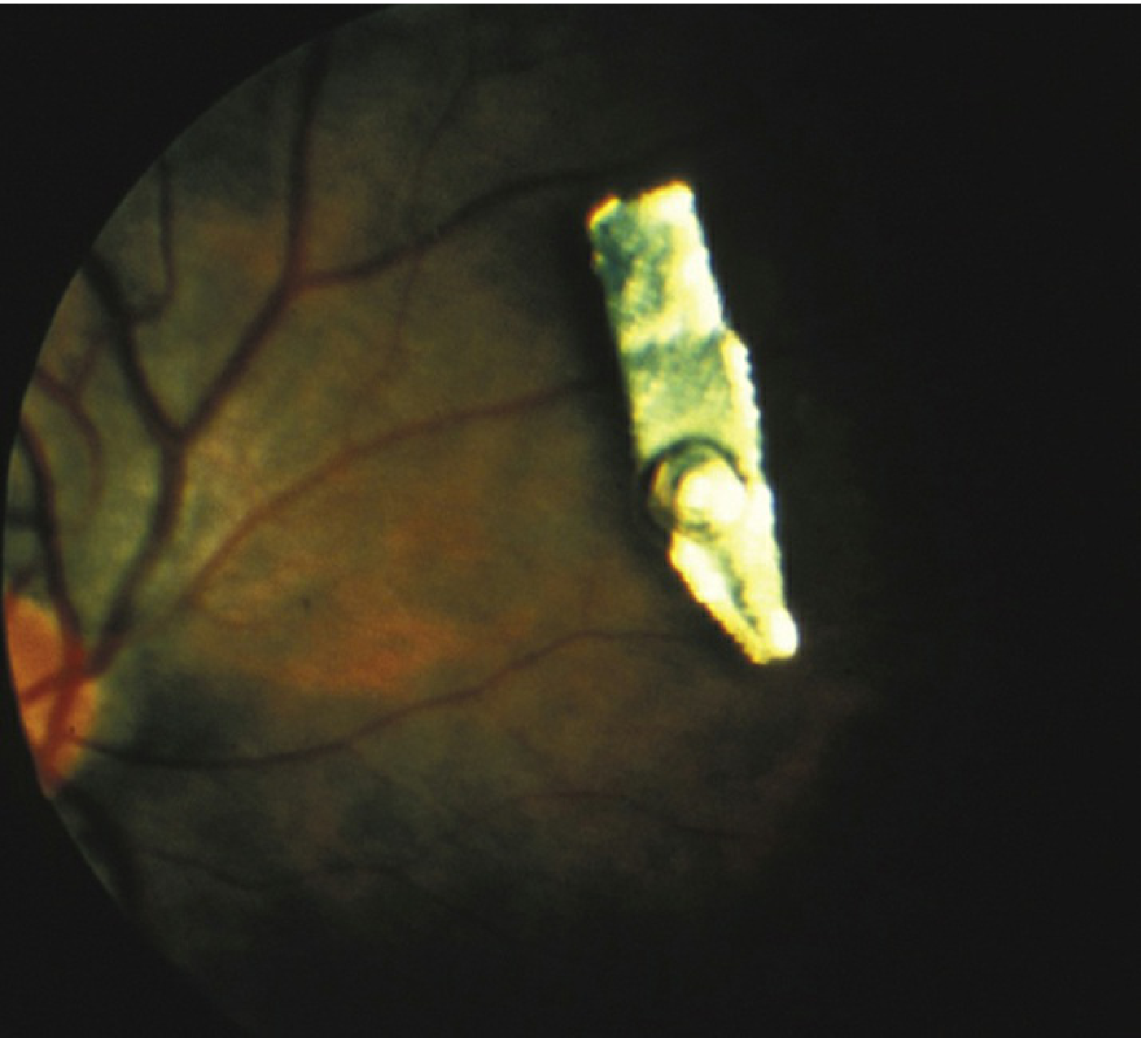
Metallic IOFB visible in the vitreous cavity on fundoscopy
Clinical image — IOFB with vitreous hemorrhage
IOFB in the posterior segment with associated hemorrhage
Workup / Diagnosis
History
- Nature and composition of the foreign body
- Time of last meal (for surgical planning)
- Mechanism — hammering, power tools, fireworks, gunshot
Examination
- Visual acuity in all patients
- Slit-lamp — inspect AC, iris (TID), lens (disruption/cataract/embedded FB)
- IOP measurement
- Careful gonioscopy if no wound leak detected and globe appears intact
- Dilated fundus exam with indirect ophthalmoscopy
- Apply topical fluorescein to identify entry wounds
Minimize pressure on the eye at all times.
Imaging
| Modality | Role |
|---|---|
| CT scan (axial + coronal, ≤1 mm sections) | First-line — gold standard for metallic IOFBs; superior sensitivity and specificity to plain X-ray and ultrasound |
| B-scan ultrasound | Useful when CT is unavailable or for posterior localization; defer if anterior rupture suspected |
| UBM (Ultrasound Biomicroscopy) | Inspect AC angle or sulcus for hidden FB |
| MRI | CONTRAINDICATED in any suspected metallic (ferrous) IOFB — risk of movement and further injury |
| Plain X-ray | Inferior to CT; may be used as screening tool |
Wood, glass, and plastic may be difficult to visualize on CT — always mention suspicion of nonmetallic IOFB to the radiologist.
Immediate Emergency Management
- NPO (nothing by mouth) — hospitalize and keep nil by mouth until surgical repair
- Rigid protective shield over the eye — do NOT patch (patching increases pressure)
- Do NOT apply pressure to the globe — further examination deferred to the operating room if perforation is obvious
- Tetanus prophylaxis as indicated
- Systemic broad-spectrum antibiotics (gram-positive + gram-negative coverage):
- Vancomycin 1 g IV q12h + Ceftazidime 1 g IV q12h, OR
- Ciprofloxacin 400 mg IV q12h, OR
- Moxifloxacin 400 mg IV daily
- ⚠️ Fluoroquinolones contraindicated in children and pregnant women
- Cycloplegia (e.g., atropine 1% b.i.d.) for posterior-segment IOFBs
- Emergent ophthalmology consultation
Surgical Removal
Indications
- All acute IOFBs — urgent removal reduces risk of endophthalmitis and proliferative vitreoretinopathy (PVR)
- Copper or contaminated foreign bodies — especially urgent
- Chronic IOFB — remove if causing severe recurrent inflammation, in the visual axis, or causing siderosis
- Inert, intraorbital FBs (not intraocular) may sometimes be left if removal causes more damage than presence
Surgical Techniques
| Technique | Indication |
|---|---|
| Magnetic extraction | Ferrous IOFBs — sclerotomy adjacent to FB, magnet applied, cryotherapy to retinal break |
| Forceps via PPV (pars plana vitrectomy) | Non-magnetic IOFBs and magnetic FBs not safely removable by magnet; FB removed through pars plana or limbus depending on location |
Antibiotic Prophylaxis for Endophthalmitis
- Oral: Ciprofloxacin 750 mg twice daily or Moxifloxacin 400 mg once daily
- Topical antibiotic + steroid + cycloplegia for open globe
- Prophylactic intravitreal antibiotics — especially in high-risk cases (agricultural injuries, soil/vegetable contamination)
- Culture the removed IOFB
Endophthalmitis risk: ~10% with retained IOFB after penetrating trauma. Pathogens: Staphylococcus spp. and Bacillus spp. account for ~90% of culture-positive cases.
Complications of Retained IOFBs
Siderosis (Iron/Steel)
- Iron dissociates and deposits in RPE, lens epithelium, iris and ciliary body epithelium
- Signs: Anterior capsular cataract with radially distributed iron deposits, heterochromia iridis (reddish-brown iris staining), pigmentary retinopathy → geographic RPE atrophy, trabecular damage → glaucoma
- ERG: Progressive attenuation of the b-wave
- A missed ferrous IOFB → late visual loss from siderosis
Chalcosis (Copper alloy — low copper content)
- Dissociated copper deposits intraocularly — resembles Wilson disease picture
- Signs: Kayser-Fleischer ring, anterior "sunflower" cataract, golden retinal plaques
- Visual function may be preserved (copper is less retinotoxic than iron)
- Pure copper (>85%) → violent endophthalmitis-like reaction → phthisis bulbi
Proliferative Vitreoretinopathy (PVR)
- A major risk of delayed IOFB removal
Follow-Up
- Close inpatient observation for signs of inflammation or infection
- Post-op imaging (CT, B-scan, or UBM) if uncertainty about complete removal
- Serial ERGs if IOFB is left in place — to detect early siderosis (b-wave attenuation)
- Long-term periodic follow-up for years — watch for delayed inflammatory reactions in both eyes (sympathetic ophthalmia risk)
Anesthesia Note (for Emergency Physicians)
When rapid sequence intubation is needed: rocuronium preferred over succinylcholine in open-globe injury (theoretical IOP rise with succinylcholine may extrude ocular contents), though compelling evidence of harm is lacking.
Sources: Kanski's Clinical Ophthalmology 10th Ed., p. 942–943 | Wills Eye Manual, p. 142–145 | Rosen's Emergency Medicine, p. 884–885
📌 Recent review (2024): A review in Frontiers in Ophthalmology on advances in IOFB management is available (PMID: 39285858) for updated surgical and prognostic considerations.
This is a shared conversation. Sign in to Orris to start your own chat.