Hyponatremia correction using hypertonic saline
Reading File
Finding Sources
Searching PubMed
"hyponatremia"[MeSH Terms] AND "hypertonic saline"[MeSH Terms]
Finding Sources
Searching PubMed
"hyponatremia"[MeSH Terms] AND "hypertonic saline"
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive data from multiple authoritative sources. Let me compile the full answer.
Hyponatremia Correction Using Hypertonic Saline
Indications for Hypertonic Saline (3% NaCl)
Hypertonic saline is indicated in two main scenarios:
- Acute symptomatic hyponatremia — Na⁺ < 120 mEq/L with neurologic symptoms (seizures, coma, reduced consciousness, vomiting, cardiorespiratory compromise)
- Severe but asymptomatic hyponatremia — Na⁺ ≤ 110 mEq/L regardless of symptoms
The guiding principle: symptoms matter more than the absolute sodium level. Both the European guidelines and U.S. expert consensus recommend 3% saline for life-threatening hyponatremia regardless of whether onset is acute or chronic when seizures or impending brainstem herniation are present. — Tintinalli's Emergency Medicine, p. 578
Pathophysiology: Why Careful Correction Matters
When neurons are exposed to a hypo-osmolar environment, they shed intracellular sodium and potassium to reduce their own osmolality and prevent cerebral edema. If serum sodium is corrected too rapidly, water shifts out of neurons into the hyperosmolar extracellular space, causing diffuse demyelination — osmotic demyelination syndrome (ODS), also called central pontine myelinolysis (CPM). — Rosen's Emergency Medicine, p. 2448
ODS manifests 2–3 days after rapid correction as behavioral changes, cranial nerve palsies, and progressive weakness culminating in quadriplegia and locked-in syndrome. T2-weighted MRI shows hyperintense pontine lesions (may be absent for up to 2 weeks). — Comprehensive Clinical Nephrology, p. 772
Risk factors for ODS:
- Severe chronic hyponatremia (Na⁺ < 120 mmol/L, duration > 48 h)
- Pre-existing hypokalemia, malnutrition, alcohol use disorder
- Liver transplantation (incidence 13–29%)
Protocol: Acute Symptomatic Hyponatremia (Seizures / Coma)
(Tintinalli Table 17-7; Comprehensive Clinical Nephrology)
| Step | Action |
|---|---|
| 1 | Confirm indication: seizures, coma, or impending brainstem herniation |
| 2 | Infuse 100–150 mL of 3% NaCl IV over 15–20 minutes |
| 3 | Check serum [Na⁺] after each bolus |
| 4 | Stop when symptoms improve or [Na⁺] rises by 4–6 mEq/L |
| 5 | May repeat up to 3 total doses (max ~450 mL 3% NaCl) |
| 6 | Maintain IV line with 0.9% NaCl; limit total rise to ≤8–12 mEq/L in 24 h; ≤18 mEq/L in 48 h |
For very severe cases (ongoing seizures, obtundation): 3% NaCl can be infused at 4–6 mL/kg/hr with monitoring of neurologic and pulmonary status, electrolytes every 2 hours. — Comprehensive Clinical Nephrology, p. 801
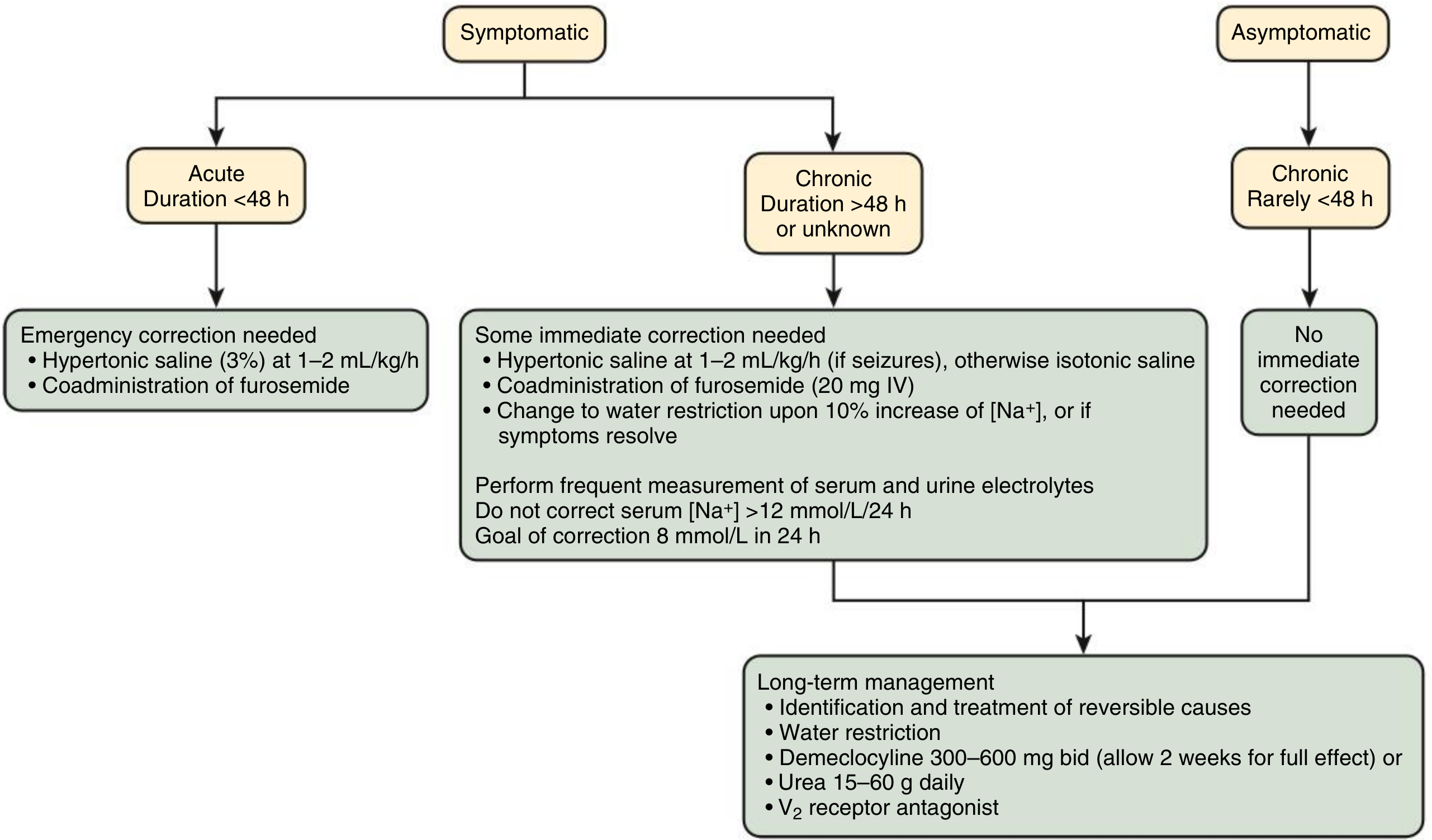
Protocol: Chronic / Unknown-Duration Hyponatremia With Symptoms
- Start 3% NaCl at 1–2 mL/kg/hr if seizures are present; switch to isotonic saline otherwise
- Co-administer furosemide 20 mg IV to enhance free water excretion
- Target a rise of 4–6 mEq/L within the first 4–6 hours — sufficient to reverse neurologic sequelae
- Switch to water restriction once [Na⁺] rises 10% or symptoms resolve
- Do NOT exceed 8 mEq/L in 24 h (high-risk patients); 12 mEq/L in 24 h is the absolute maximum
A continuous infusion starting at 0.25–0.3 mL/kg/hr provides the greatest margin of safety for stable patients, titrating based on labs. — Washington Manual, p. 2474
Management Algorithm
Correction Rate Limits (Summary Table)
| Setting | Maximum correction |
|---|---|
| Acute symptomatic (any duration) — initial target | 4–6 mEq/L in first 6 h |
| Any patient — first 24 h | ≤ 8–12 mEq/L |
| High-risk patients (hypokalemia, malnutrition, EtOH) | ≤ 6–8 mEq/L in 24 h |
| 48-hour ceiling | ≤ 15–18 mEq/L |
Adrogue–Madias Formula (Estimating Infusion Rate)
Used to estimate the expected [Na⁺] change per liter of infusate:
ΔNa⁺ = (Infusate [Na⁺] − Serum [Na⁺]) ÷ (Total Body Water + 1)
- 3% NaCl contains 513 mEq/L sodium
- TBW = 0.6 × weight (men), 0.5 × weight (women), 0.45 × weight (elderly)
Caution: This formula does not account for ongoing free water losses or dynamic changes in ADH. Labs must be rechecked every 2 hours regardless of formula estimates. — Comprehensive Clinical Nephrology, p. 817
Preventing Overcorrection: DDAVP Clamp
Desmopressin acetate (DDAVP) can be given to prevent overcorrection in patients with a potentially reversible cause of ADH suppression (e.g., volume depletion, hypothyroidism). Once ADH levels fall with volume restoration, free water diuresis can cause a dangerously rapid rise in [Na⁺]. Prophylactic DDAVP "clamps" aquaporin-2 channels to prevent this. — Washington Manual, p. 2480
Characteristics of Hypertonic Saline
| Infusate | [Na⁺] (mEq/L) | Tonicity |
|---|---|---|
| 0.9% NaCl | 154 | Isotonic |
| 3% NaCl | 513 | Hypertonic |
| 7.5% NaCl | ~1,283 | Hypertonic |
Cause-Specific Considerations
- Hypovolemic hyponatremia: Isotonic saline restores volume → drops ADH → free water diuresis. Hypertonic saline may be needed if seizing.
- SIADH: Fluid restriction is first-line; hypertonic saline reserved for severe neurologic symptoms.
- Hypervolemic hyponatremia (CHF, cirrhosis): Hypertonic saline used very cautiously due to fluid overload risk; vasopressin antagonists (vaptans) may be considered.
- Psychogenic polydipsia/MDMA toxicity: Treatment is same as SIADH — fluid restriction ± hypertonic saline if seizing; isotonic saline can worsen hyponatremia by inadvertently raising ADH. — Rosen's Emergency Medicine
- Exercise-associated hyponatremia: Hypertonic saline is the treatment of choice in severe cases.
Key Pitfalls
- Overcorrection → ODS: the most feared complication. Symptoms appear 2–3 days later, not immediately.
- Normal saline in SIADH: Can worsen hyponatremia because the kidney excretes dilute urine, retaining free water.
- Delaying treatment in acute symptomatic hyponatremia: The risk of uncorrected cerebral edema greatly exceeds the risk of ODS in the acute setting.
- Relying solely on formulas: No equation accounts for dynamic changes in water balance. Frequent lab monitoring is mandatory.
Sources: Tintinalli's Emergency Medicine (17-7, 17-8) | Comprehensive Clinical Nephrology, 7th ed. (pp. 772–820) | Washington Manual of Medical Therapeutics (pp. 2459–2480) | Rosen's Emergency Medicine | Harrison's Principles of Internal Medicine, 22e (p. 2392)
This is a shared conversation. Sign in to Orris to start your own chat.