define fever the tempertaure thats given in standard books on various areas of body in celscius and farhenheit
fever definition temperature thresholds oral rectal axillary tympanic Celsius Fahrenheit standard medical textbooks
Definition of Fever - Temperature Thresholds by Body Site
What is Fever?
Definition of Fever - By Source/Context
| Source | Fever Definition |
|---|---|
| Goldman-Cecil Medicine | >99°F (37.2°C) at 6 AM, or >100°F (37.8°C) at any time of day |
| Harrison's Principles of Internal Medicine 22e (2025) | Core temperature ≥38.3°C (≥101°F) - most common definition used for FUO studies |
| Harrison's - for neutropenic fever | Single oral temp ≥38.3°C, OR temp ≥38.0°C sustained for ≥1 hour |
| Roberts & Hedges' Clinical Procedures in Emergency | Oral ≥37.8°C (100°F); Rectal ≥38.0°C (100.4°F); IR ear ≥37.6°C (99.6°F) |
| Rosen's Emergency Medicine | 100.4°F threshold (lower threshold considered for frail elderly) |
| Berek & Novak's Gynecology (postoperative) | ≥100.4°F (38°C) on two occasions at least 4 hours apart |
| FUO definition (classic, multiple books) | Temp >38.3°C on several occasions, illness >3 weeks |
Fever Thresholds by Measurement Site
| Body Site | Thermometer Type | Normal Range (°C) | Fever Threshold (°C) | Fever Threshold (°F) |
|---|---|---|---|---|
| Core (PA catheter/esophageal/tympanic thermistor) | Electronic | 36.4 - 37.9 | ≥38.0 | ≥100.4 |
| Oral | Mercury-in-glass, Electronic | 35.5 - 37.7 | ≥37.8 | ≥100.0 |
| Rectal | Mercury-in-glass, Electronic | 36.6 - 37.9 | ≥38.0 | ≥100.4 |
| Ear (tympanic, IR) | Infrared emission | 35.7 - 37.5 | ≥37.6 | ≥99.6 |
Note: Axillary temperature is not listed in this table because it is considered unreliable. Widely accepted clinical guidance (Mayo Clinic, Children's Mercy) uses axillary ≥37.2°C (99°F) as the fever threshold, though it runs ~0.5-1°C lower than rectal.
Site-by-Site Breakdown (Summary)
| Site | Fever (°C) | Fever (°F) | Notes |
|---|---|---|---|
| Rectal | ≥38.0 | ≥100.4 | Gold standard for core temp; most accurate |
| Oral | ≥37.8 | ≥100.0 | ~0.4°C lower than rectal |
| Tympanic (ear, IR) | ≥37.6 | ≥99.6 | Infrared; less accurate before age 6 months |
| Axillary (armpit) | ≥37.2 | ≥99.0 | ~0.8°C lower than rectal; least accurate |
| Temporal artery (forehead) | ≥38.0 | ≥100.4 | Used as proxy for core; similar to rectal |
| Core (esophageal/PA catheter) | ≥38.0 | ≥100.4 | ICU setting; true reference standard |
Special Populations
- Neonates/Infants (Roberts & Hedges): Rectal fever defined as ≥38.0°C in infants <30 days; ≥38.1°C in 1-2 months; ≥38.2°C in 2-3 months
- Neutropenic fever (Harrison's): Single oral ≥38.3°C OR ≥38.0°C sustained ≥1 hour
- FUO (Harrison's, Goldman-Cecil, Frameworks for Internal Medicine): >38.3°C on several occasions, illness >3 weeks, no diagnosis after 1 week of evaluation
- Elderly: May have blunted febrile response; Rosen's notes a lower functional threshold should be considered in frail older adults
Temperature Conversion Reference
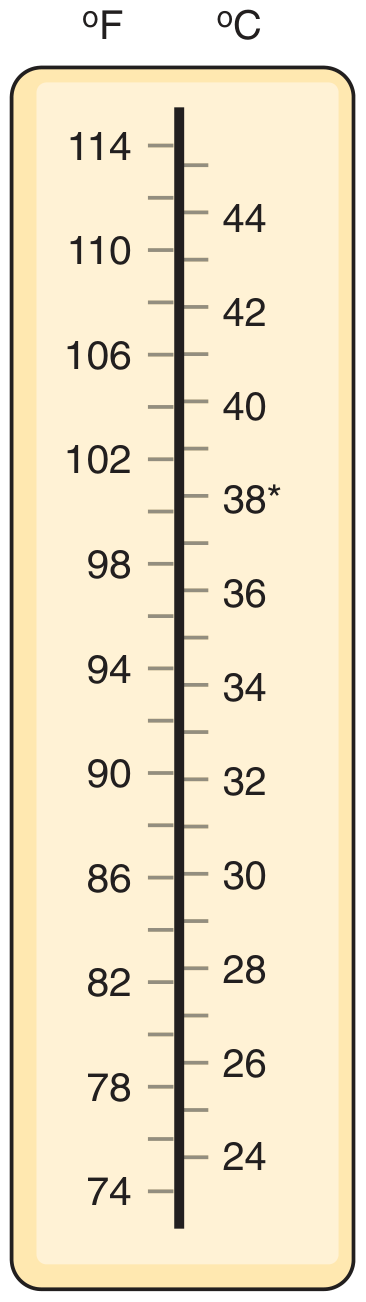
- °C to °F: (°C × 9/5) + 32
- °F to °C: (°F - 32) × 5/9
Key Takeaway
What are the physiological mechanisms behind fever (pyrogens and thermoregulation)?2 yo with fever bleeding gum petechial rash over legs .. give dd hx and exmaination lab findings and mx
12 yo with fever bleeding gum petechial rash over legs .. give dd hx and exmaination lab findings and mx
12 year old fever petechiae bleeding gums differential diagnosis pediatrics meningococcemia leukemia ITP
fever pyrogens thermoregulation mechanism IL-1 IL-6 TNF prostaglandin E2 hypothalamus set point
dengue fever petechiae thrombocytopenia bleeding child diagnosis management guidelines
fever petechiae bleeding gums child 12 year history examination lab management meningococcemia ITP leukemia
Quick Reference - Most Important Points
-
Meningococcemia - fever + spreading petechiae + sepsis signs = give IV Ceftriaxone BEFORE all results. Do NOT wait. This kills in hours.
-
Acute Leukemia (ALL/AML) - gum bleeding + bone pain + pallor + blasts on blood film → urgent oncology referral. AML (M4/M5) specifically causes gum infiltration/bleeding.
-
ITP - isolated thrombocytopenia, usually post-viral, usually afebrile. Treat with IVIG or steroids if platelets <30,000 or mucosal bleeding present.
-
Dengue - in endemic areas, classic fever + petechiae + thrombocytopenia + hemoconcentration. NS1 antigen test early, IgM later.
define FUO
fever of unknown origin FUO definition criteria Petersdorf Durack classification categories
Fever of Unknown Origin (FUO)
Historical Background
Definition - Evolution Over Time
Original Definition (Petersdorf & Beeson, 1961)
Fever ≥38.3°C (≥101°F) on at least 3 occasions, illness lasting ≥3 weeks, and no diagnosis after 1 week of inpatient evaluation
Revised Definition (Durack & Street, 1991)
3 outpatient visits OR 3 days of inpatient investigation (replacing the mandatory 1-week hospitalization)
Current Definition (Harrison's Principles of Internal Medicine 22e, 2025)
| Criterion | Threshold |
|---|---|
| Temperature | Fever ≥38.3°C (≥101°F) on at least two occasions |
| Duration | Illness lasting at least 3 weeks |
| Immunocompromised state | No known immunocompromised state (these patients are classified separately) |
Important: A minimum qualifying diagnostic workup must be completed before labeling a fever as FUO, to exclude common and self-limiting illnesses.
The Four Categories of FUO (Durack & Street, 1991 - still widely used)
| Category | Setting | Key Features |
|---|---|---|
| 1. Classic FUO | Community/outpatient | Meets the original Petersdorf-Beeson criteria; the most studied form |
| 2. Nosocomial FUO | Hospitalized patients | Fever ≥38.3°C on several days, not present on admission; develops after ≥24-48 hrs of hospitalization |
| 3. Neutropenic (Immune-deficient) FUO | Chemotherapy, transplant, HIV | Fever ≥38.3°C, neutrophil count ≤500/µL; risk of opportunistic infections |
| 4. HIV-associated FUO | HIV/AIDS patients | Fever ≥38.3°C, confirmed HIV, illness >4 weeks as outpatient or >3 days as inpatient |
Causes of Classic FUO - The "Big Four" Categories
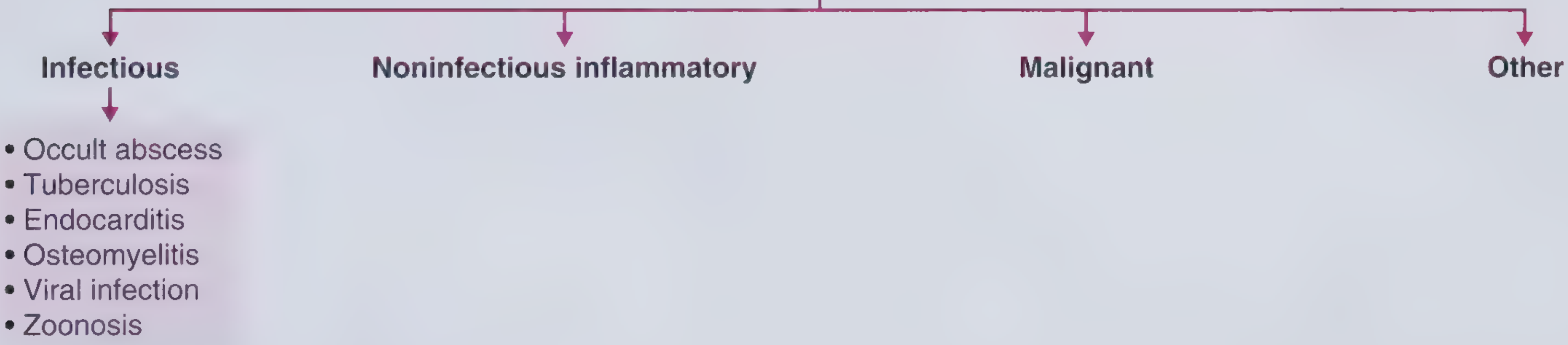
1. Infectious (most common in developing countries)
- Intra-abdominal abscess (liver, spleen, perinephric) - #1 infectious cause in industrialized world
- Tuberculosis (especially extrapulmonary, miliary, hepatic)
- Infective endocarditis (especially culture-negative)
- Osteomyelitis
- Viral: EBV, CMV, HIV (acute seroconversion)
- Zoonoses: brucellosis, cat-scratch disease, Q fever, leptospirosis
- Malaria (travel history)
2. Non-Infectious Inflammatory Diseases (NIIDs) - most common in Western countries
- Adult-onset Still's disease (AOSD) - quotidian fever ≥39°C + salmon-colored rash + arthritis + serum ferritin often >2000 ng/mL; presents as FUO in up to 10% of cases
- Giant Cell Arteritis (GCA) / Polymyalgia Rheumatica - common in >50 yrs
- Systemic Lupus Erythematosus (SLE)
- Rheumatoid arthritis
- Vasculitides: Wegener's (GPA), Polyarteritis nodosa
- Sarcoidosis
- Familial Mediterranean Fever (FMF) - periodic fever, responds to colchicine
- Adult Crohn's disease / IBD
- IgG4-related disease
3. Malignancy
- Lymphomas (Hodgkin and Non-Hodgkin) - most common malignant cause
- Leukemia
- Renal cell carcinoma (classic "internist's tumor" - causes FUO)
- Hepatocellular carcinoma
- Atrial myxoma (tumor-related IL-6 release)
4. Miscellaneous / Other
- Drug fever (any drug can cause it; common: antibiotics, antiepileptics, allopurinol)
- Factitious fever (self-induced)
- Thromboembolic disease (DVT/PE)
- Hyperthyroidism / thyroiditis
- Adrenal insufficiency
- Periodic fever syndromes (autoinflammatory)
- Undiagnosed (in Western cohorts, up to >50% may remain without diagnosis - "the FUO paradox")
Geographic Distribution of FUO Causes (Harrison's 22e Table 22-1)
| Region | Infections (%) | NIIDs (%) | Malignancy (%) | No Diagnosis (%) |
|---|---|---|---|---|
| Western Europe | 15.5 (4-36) | 25 | 11 (3-30) | 39.5 (26-54) |
| Eastern Europe/Turkey | 42 (26-74) | 23 (12-38) | 14 (4-19) | 16 (0-35) |
| Middle East | 66 (42-79) | 15 (7-17) | 7 (1-30) | 8 (2-12) |
| Asia | 42 (3-58) | 19 (7-57) | 13 (6-23) | 17 (0-81) |
The "FUO Paradox"
Approach to FUO - Key Investigations
Tier 1 - Always Do First
- CBC with differential + ESR + CRP
- LFTs, RFTs, LDH, uric acid
- Serum ferritin (>2000 = AOSD; >10,000 = hemophagocytic lymphohistiocytosis)
- Blood cultures x3 (before antibiotics)
- Urine culture
- Chest X-ray
- ANA, RF, ANCA
- HIV serology
- TST (tuberculin) or IGRA (for TB)
- Urine protein, microscopy
Tier 2 - Based on Clues
- CT abdomen/pelvis (occult abscess, lymphoma, RCC)
- Echocardiography (endocarditis)
- 18F-FDG PET-CT - localizes active lesions; correct diagnosis in >50% of FUO cases; particularly useful for vasculitis, sarcoidosis, lymphoma, occult infection
- Bone marrow biopsy (malignancy, TB, leishmaniasis)
- Serology: EBV, CMV, Brucella, Q fever, Bartonella, toxoplasma
- Colonoscopy/capsule endoscopy (Crohn's, lymphoma)
- Temporal artery biopsy (if GCA suspected)
- Skin biopsy (vasculitis)
Treatment
- Hemodynamic instability → empirical antibiotics
- Positive IGRA/TST + extrapulmonary TB pattern → empirical antituberculous therapy (after cultures/PCR sent)
- FMF suspected → colchicine trial
- AOSD or GCA likely (infection/malignancy excluded) → glucocorticoids
Prognosis
- In FUO patients without a final diagnosis after full evaluation, the majority spontaneously become symptom-free
- Mortality risk is highest during the index admission
- Patients with no diagnosis after extensive workup generally have a favorable prognosis
lab investigations for dengue complications and mx
dengue fever complications lab investigations CBC hematocrit NS1 coagulation LFT management WHO 2024
dengue severe complications dengue shock syndrome expanded dengue syndrome organ involvement management 2024
dengue complications lab investigations hematocrit platelet coagulation LFT NS1 tourniquet management fluid shock
Dengue - Complications, Lab Investigations, and Management
WHO 2009 Classification of Dengue Severity
DENGUE
├── 1. Dengue WITHOUT warning signs
├── 2. Dengue WITH warning signs ← Watch carefully
└── 3. SEVERE DENGUE ← Emergency
Warning Signs (appear near defervescence, days 3-7):
- Abdominal pain or tenderness
- Persistent vomiting
- Clinical fluid accumulation (ascites, pleural effusion)
- Mucosal bleeding (gums, nose, vaginal)
- Lethargy / restlessness
- Liver enlargement >2 cm
- Rising hematocrit with rapid fall in platelet count (lab warning sign)
Phases of Dengue and When Complications Occur
| Phase | Duration | Key Events |
|---|---|---|
| Febrile | Days 1-7 | High fever, myalgia, rash, leukopenia, early thrombocytopenia |
| Critical | Days 3-7 (24-48 hrs of plasma leakage) | Plasma leakage, hemoconcentration, shock, bleeding - most complications here |
| Recovery | Days 7-10 | Fluid reabsorption, bradycardia, diuresis, pruritic rash ("islands of white in a sea of red") |
Complications of Dengue
1. Dengue Hemorrhagic Fever (DHF)
- Fever lasting 2-7 days
- Hemorrhagic tendency (positive tourniquet test OR spontaneous bleeding)
- Thrombocytopenia (platelets ≤100,000/µL)
- Evidence of plasma leakage: hematocrit rise ≥20% from baseline, pleural effusion, ascites
2. Dengue Shock Syndrome (DSS)
3. Severe Dengue (WHO 2009)
- Severe plasma leakage → shock or respiratory distress
- Severe bleeding (clinician-assessed)
- Severe organ involvement:
- Liver: AST or ALT ≥1000 IU/L
- CNS: Impaired consciousness
- Heart and other organs
4. Expanded Dengue Syndrome (EDS)
| Organ System | Manifestations |
|---|---|
| Cardiac | Myocarditis, pericarditis, bradyarrhythmias (sinus bradycardia, AV block), tachyarrhythmias, pericardial effusion |
| Hepatic | Acute liver failure, acalculous cholecystitis, acute pancreatitis, fulminant hepatic failure (rare) |
| Renal | Acute kidney injury (AKI) |
| Neurological | Encephalitis, meningoencephalitis, post-dengue ADEM, Guillain-Barré syndrome |
| Respiratory | ARDS, pneumonitis, pulmonary hemorrhage |
| Hematological | Hemophagocytic lymphohistiocytosis (HLH) |
| Musculoskeletal | Rhabdomyolysis |
| GI | GI bleeding, intestinal perforation |
Laboratory Investigations
Diagnostic Tests for Dengue (Confirm the Infection)
| Test | Window | Notes |
|---|---|---|
| NS1 Antigen (ELISA or rapid) | Days 1-5 of fever (up to day 7-10) | Best early test; sensitivity 80-100%; do NOT do after day 5 |
| RT-PCR | Days 1-5 | Gold standard; detects viral RNA; available in reference labs |
| Dengue IgM (EIA) | From day 3-5, peaks at 2 weeks | 99% positive by day 10; cross-reacts with Zika/flaviviruses |
| Dengue IgG | Present in secondary infection from day 1; lifelong after primary | 4-fold rise between acute (<5 days) and convalescent (>15 days) confirms recent infection |
| Combined NS1 + IgM on single specimen (days 1-10) | Identifies ≥90% of primary and secondary dengue cases |
- Days 1-5: NS1 antigen (+ PCR if available)
- Days 5-7: NS1 may be negative; IgM may not yet be positive → use IgG
- After day 5: IgM antibody
- Convalescence: IgG paired sera (fourfold rise confirms)
Monitoring Labs (for Complications and Disease Severity)
Mandatory in ALL admitted patients:
| Investigation | What It Detects | Key Thresholds |
|---|---|---|
| CBC with differential | Leukopenia, thrombocytopenia, hemoconcentration | Platelets <100,000 = DHF risk; <10,000 = severe bleeding risk |
| Hematocrit (HCT) - serial every 6-8 hrs | Plasma leakage (hemoconcentration) | ≥20% rise from baseline = significant plasma leakage; falling HCT = occult bleeding or fluid overload |
| Platelet count - serial | Thrombocytopenia trend | Watch for rapid fall concurrent with HCT rise (warning sign) |
| Liver function tests (AST, ALT, bilirubin, albumin) | Hepatitis, acute liver failure | AST/ALT ≥1000 = severe dengue; AST often rises more than ALT in dengue |
| Coagulation profile (PT, aPTT, INR, fibrinogen) | DIC, coagulopathy | Prolonged PT/aPTT + low fibrinogen = DIC |
| Blood glucose | Hypoglycemia (hepatic failure) | Critical to monitor in severe dengue |
| Serum electrolytes (Na, K, Cl) | Hyponatremia (plasma leakage), dyselectrolytemia | Hyponatremia common |
| Blood urea + creatinine | AKI (EDS) | Rising creatinine = renal involvement |
| Blood gas + lactate | Metabolic acidosis, tissue hypoperfusion in shock | Lactate >2 = shock marker |
| Urine output | Fluid balance, renal perfusion | Target ≥0.5 mL/kg/hr |
Tourniquet Test (Rumple-Leede):
- Inflate BP cuff to midpoint between systolic and diastolic for 15 minutes
- >20 petechiae in a 2.5 cm circle = positive (capillary fragility)
- Key clinical bedside test for dengue hemorrhagic tendency
Additional Labs Based on Complication
| Complication | Additional Tests |
|---|---|
| Suspected DIC | D-dimers, fibrin degradation products (FDP), fibrinogen |
| Severe hepatitis / liver failure | PT/INR, albumin, ammonia, hepatic encephalopathy screen |
| AKI | Creatinine, BUN, urinalysis, urine electrolytes, urine output chart |
| Myocarditis | ECG, troponin I/T, CK-MB, echocardiography |
| Neurological involvement | CT head (exclude hemorrhage), CSF analysis (encephalitis), EEG |
| Hemophagocytic Lymphohistiocytosis (HLH) | Serum ferritin (>3000 IU/L significant), LDH, triglycerides, CRP, bone marrow biopsy; calculate H-Score |
| Rhabdomyolysis | CK (creatine kinase), urine myoglobin, creatinine |
| ARDS / respiratory | Chest X-ray (bilateral infiltrates), arterial blood gas, SpO2 |
| Pancreatitis | Serum amylase, lipase, abdominal ultrasound |
| Group and match | If transfusion anticipated (bleeding or Hb <7 g/dL) |
Imaging
| Investigation | Purpose |
|---|---|
| Chest X-ray | Pleural effusion (right-sided first), pulmonary infiltrates (ARDS) |
| Ultrasound abdomen | Ascites, pleural effusion (most sensitive), gallbladder wall thickening (dengue), hepatosplenomegaly |
| Echocardiography | Pericardial effusion, myocarditis, ejection fraction |
| CT head | Intracranial hemorrhage (in severe thrombocytopenia or neurological dengue) |
Management
WHO Group A - Home Management (Dengue without warning signs, clinically stable)
- Oral fluids (ORS, coconut water, juice) - maintain adequate hydration
- Paracetamol 15 mg/kg/dose (max 4 doses/day) for fever and pain
- AVOID: Aspirin, ibuprofen, NSAIDs (increase bleeding risk; aspirin = Reye syndrome in children)
- Instructions: return immediately if warning signs develop
WHO Group B - Hospital Admission
Without Warning Signs:
- Oral fluids if tolerated
- IV fluids if not tolerating orally: 0.9% NaCl or Ringer's Lactate at maintenance rate for 24-48 hrs
- Serial CBC, HCT monitoring
WITH Warning Signs (Dengue + Warning Signs):
- Baseline HCT before fluids
- IV isotonic fluids (0.9% NaCl or Ringer's Lactate):
- 5-7 mL/kg/hr x 1-2 hrs → then 3-5 mL/kg/hr x 2-4 hrs → then 2-3 mL/kg/hr until oral intake adequate
- Monitor HCT every 2-4 hrs; adjust fluid rate based on HCT trends
- Monitor urine output (target 0.5 mL/kg/hr, check every 6-8 hrs)
- Daily platelet count
WHO Group C - Emergency (Severe Dengue / DSS)
Dengue Shock Syndrome - Compensated Shock:
- Immediate IV isotonic crystalloid bolus: 10-20 mL/kg over 15-30 mins
- Reassess clinically after each bolus (HR, BP, capillary refill, HCT)
- If improved: reduce to 10 mL/kg/hr, then step down as above
- If HCT rises despite fluids → use colloids (dextran-40 or gelatin solutions 10-20 mL/kg)
Uncompensated Shock (hypotension):
- Rapid bolus 20 mL/kg crystalloid over 15-30 mins
- If poor response → colloid bolus
- If refractory → Norepinephrine (vasopressor of choice per ISCCM 2024); avoid excessive fluids in capillary leak
- ICU monitoring: HCT, urine output hourly, blood gas, lactate
Transfusion Thresholds in Dengue
| Situation | Action |
|---|---|
| Platelets <10,000 without bleeding | Observe; prophylactic transfusion generally NOT recommended |
| Platelets <10,000 with active bleeding | Platelet transfusion |
| Active significant bleeding (GI, CNS, vaginal) | Packed red cells, FFP, platelets as needed |
| Hb <7 g/dL (with hemodynamic instability) | Packed red cells transfusion |
| Falling HCT + unstable → suspect occult bleeding | Cross-match, transfuse if significant drop |
| DIC | FFP (10-15 mL/kg), cryoprecipitate (for fibrinogen), platelets |
Note: Platelet transfusions are often rapidly destroyed; transfuse only for active bleeding or pre-procedure - not for platelet count alone.
Management of Specific Complications
| Complication | Management |
|---|---|
| Acute Liver Failure | Avoid hepatotoxic drugs; correct coagulopathy (FFP); lactulose for encephalopathy; liver transplant referral in fulminant failure |
| AKI | IV fluid optimization; renal replacement therapy (dialysis) if oliguric/anuric despite resuscitation |
| Myocarditis | Cardiac monitoring, anti-arrhythmics if needed, inotropic support; avoid aggressive fluids |
| Neurological (encephalitis) | Airway protection, seizure control, anti-cerebral edema measures (mannitol, hyperventilation); IVIg for dengue GBS |
| Post-dengue ADEM | Pulsed IV methylprednisolone |
| HLH | Dexamethasone + etoposide (based on H-Score); bone marrow transplant in refractory cases |
| ARDS | Lung-protective ventilation (tidal volume 6 mL/kg, PEEP optimization); avoid fluid overload |
| Rhabdomyolysis | Aggressive IV fluids to maintain urine output >1-3 mL/kg/hr; urine alkalinization |
| Pleural effusion (respiratory distress) | Therapeutic thoracocentesis only if causing ventilatory compromise; avoid routine drainage |
What NOT to Do in Dengue
- No aspirin / NSAIDs (bleeding risk + Reye syndrome in children)
- No prophylactic platelet transfusion for count alone without bleeding
- No steroids routinely (no proven benefit; may increase GI bleeding)
- No antibiotics unless secondary bacterial infection confirmed
- Avoid fluid overload - both hypovolemia AND over-hydration are dangerous; use HCT to guide
Summary Monitoring Schedule
| Parameter | Frequency |
|---|---|
| HCT | Every 6-8 hrs (stable) / every 2-4 hrs (warning signs) / hourly (shock) |
| Platelet count | Daily (mild) / 6-8 hrly (critical phase) |
| Urine output | Every 6-8 hrs (stable) / hourly (shock) |
| Vital signs | Every 4 hrs (stable) / continuous (ICU) |
| Blood glucose | Every 6-8 hrs (severe dengue) |
| Creatinine, LFTs | Daily (warning signs/severe) |
| Blood gas + lactate | As needed in shock |
typhoid mx regime
typhoid fever treatment guidelines 2024 antibiotic regimen fluoroquinolone ceftriaxone azithromycin MDR XDR
typhoid treatment regimen doses duration uncomplicated complicated MDR XDR ceftriaxone azithromycin carbapenem
Typhoid Fever - Management Regimen
Understanding Resistance Patterns First (CRITICAL for drug choice)
| Type | Definition | Resistant to | Treat with |
|---|---|---|---|
| Susceptible | Fully sensitive | - | Fluoroquinolones (first choice) |
| MDR (Multi-Drug Resistant) | Since 1980s | Ampicillin + Chloramphenicol + TMP-SMX | Fluoroquinolones, Ceftriaxone, Azithromycin |
| DSC/FQ-R (Decreased fluoroquinolone susceptibility / Fluoroquinolone-Resistant) | Since 1990s, common in South Asia | MDR drugs + Fluoroquinolones | Ceftriaxone, Azithromycin |
| XDR (Extensively Drug Resistant) | Since 2016, Pakistan outbreak | All above + Ceftriaxone | Azithromycin (uncomplicated) / Carbapenem (severe) |
Key point from Red Book 2021: Most typhoid diagnosed in the US and UK is now fluoroquinolone non-susceptible. Do NOT use fluoroquinolones empirically for travelers from South Asia (India, Pakistan, Bangladesh, Nepal).
Empirical Treatment - Based on Travel History (Before Sensitivity Results)
| Travel Origin | Uncomplicated | Complicated/Severe |
|---|---|---|
| Pakistan / Iraq / no travel | Azithromycin | Carbapenem (meropenem) |
| Rest of South Asia (India, Bangladesh, Nepal) | Ceftriaxone OR Azithromycin | Ceftriaxone IV |
| Other countries (Africa, SE Asia, Caribbean, Latin America) | Ceftriaxone OR Azithromycin | Ceftriaxone IV |
| Fully susceptible (low-resistance area) | Ciprofloxacin | Ciprofloxacin IV |
Treatment Regimens by Susceptibility Profile
1. UNCOMPLICATED ENTERIC FEVER
Susceptible to Fluoroquinolones
| Drug | Adults (dose) | Children (dose) | Duration |
|---|---|---|---|
| Ciprofloxacin (oral, 1st choice) | 500-750 mg PO 12-hourly | 20 mg/kg/day PO in 2 divided doses | 7 days |
| Ofloxacin | 400 mg PO 12-hourly | - | 7 days |
NOT Susceptible to Fluoroquinolones (MDR / DSC)
| Drug | Adults (dose) | Children (dose) | Duration |
|---|---|---|---|
| Azithromycin (oral, preferred for outpatient MDR) | 500 mg/day PO | 20 mg/kg/day PO (max 1 g/day) | 7 days |
| Ceftriaxone IV/IM | 1-2 g IV every 12-24 hrs | 50-75 mg/kg/day IV in 2 doses | 10-14 days |
| Cefixime (oral 3rd gen) | 20 mg/kg/day PO in 2 doses | 20 mg/kg/day PO in 2 doses | 10-14 days |
Note: Relapse rates are lower with azithromycin than with fluoroquinolones or ceftriaxone (Red Book 2021).
XDR Typhoid (Pakistan-origin, resistant to ceftriaxone + fluoroquinolones)
| Drug | Adults | Children | Duration |
|---|---|---|---|
| Azithromycin (oral, uncomplicated XDR) | 500 mg/day PO | 20 mg/kg/day PO | 7 days |
| If no improvement or severe → add/switch to Meropenem | 1 g IV every 8 hrs | 20 mg/kg IV 8-hourly (max 1 g) | 10-14 days |
2. SEVERE / COMPLICATED ENTERIC FEVER (requires hospitalization, IV therapy)
Susceptible to Fluoroquinolones
| Drug | Adults | Children | Duration |
|---|---|---|---|
| Ciprofloxacin IV | 400 mg IV every 8-hourly | 10 mg/kg/dose IV every 8 hrs (max 400 mg/dose) | 10-14 days |
| Step down to oral when improving | 500-750 mg PO 12-hrly | 20 mg/kg/day PO | Complete 10-14 days total |
NOT Susceptible to Fluoroquinolones (MDR/FQ-R)
| Drug | Adults | Children | Duration |
|---|---|---|---|
| Ceftriaxone IV (drug of choice) | 2 g IV every 12-24 hrs | 75 mg/kg/day IV (max 4 g/day) | 10-14 days |
| Alternative: Cefotaxime | 2 g IV every 8 hrs | 40-80 mg/kg/day IV in 2-3 doses | 10-14 days |
| Step down to oral when improving | Azithromycin PO | Azithromycin PO | Complete course |
XDR Severe Disease
| Drug | Adults | Children (≥3 months) | Duration |
|---|---|---|---|
| Meropenem IV (drug of choice for severe XDR) | 1 g IV every 8 hrs | 20 mg/kg IV every 8 hrs (max 1 g) | 10-14 days |
| If no improvement → add Azithromycin | 500 mg/day | 20 mg/kg/day | Concurrently |
3. OLD "FIRST-LINE" DRUGS (only if proven susceptibility on culture)
| Drug | Adults dose | Duration | Notes |
|---|---|---|---|
| Chloramphenicol | 50 mg/kg/day PO or IV in 4 doses | 7-14 days | Still effective if susceptible; risk of aplastic anemia |
| Ampicillin | 25 mg/kg IV every 6 hrs | 14 days | Only if susceptible |
| TMP-SMX | 4/20 mg/kg IV or PO every 12 hrs | 14 days | Widespread resistance; only use if susceptible |
These three form the classic MDR triad - resistance to all three defines MDR typhoid.
Treatment Duration Summary
| Antibiotic | Uncomplicated | Severe/Complicated |
|---|---|---|
| Fluoroquinolone (oral/IV) | 7 days | 10-14 days |
| Azithromycin (oral) | 7 days | Not primary agent (use IV antibiotics) |
| Ceftriaxone/Cefotaxime (IV) | 10-14 days | 10-14 days |
| Meropenem (IV) | - | 10-14 days |
| Chloramphenicol / Ampicillin / TMP-SMX (if susceptible) | 14 days | 14 days |
Adjunctive Treatment
Corticosteroids (for severe toxemia ONLY)
- Indication: Delirium, obtundation, stupor, coma, or shock
- Regimen (Goldman-Cecil, Red Book 2021):
- Dexamethasone 3 mg/kg IV initial dose
- Then 1 mg/kg IV every 6 hours for 48 hours total
- Caution: Can mask signs of intestinal perforation - do NOT continue beyond 48 hours
Supportive Care
- IV fluids: 0.9% NaCl for dehydration, correct electrolytes and acid-base disturbances
- Antipyretics: Paracetamol only (avoid aspirin/NSAIDs - salicylates should be avoided)
- Nutritional support: soft, easily digestible diet (avoid high-residue food - risk of perforation)
- Blood transfusion if intestinal hemorrhage causes significant anemia
Management of Complications
| Complication | Management |
|---|---|
| Intestinal hemorrhage | IV fluids, blood transfusion; continue antibiotics; surgical opinion if severe |
| Intestinal perforation | Urgent laparotomy (primary repair or resection) + broaden antibiotics to cover bowel flora (add metronidazole + amikacin/piperacillin-tazobactam to ceftriaxone) |
| Typhoid hepatitis | Continue antibiotics; avoid hepatotoxic drugs; supportive |
| Typhoid meningitis | Ceftriaxone IV (good CNS penetration) x 14 days |
| Relapse | Repeat a full course with the same effective antibiotic (same susceptibility); azithromycin has lowest relapse rate |
Chronic Carrier State
- Defined as: stool/urine positive for S. Typhi >12 months after acute infection
- At-risk: gallbladder disease (bile provides reservoir), ~1-4% of untreated patients
- Treatment:
- Ciprofloxacin 750 mg PO twice daily x 28 days (if susceptible) - concentrated in bile
- Or Norfloxacin 400 mg twice daily x 28 days
- If fluoroquinolone resistant: azithromycin (limited data)
- Cholecystectomy + antibiotics if medical therapy fails (gallstones act as biofilm scaffold)
Prevention
| Vaccine | Type | Age | Schedule | Efficacy |
|---|---|---|---|---|
| Ty21a (Vivotif) | Live attenuated oral | ≥6 years | 4 capsules on days 1, 3, 5, 7; booster every 5 years | ~50% at 3 years |
| Vi CPS (Typhim Vi) | Purified polysaccharide IM | ≥2 years | Single dose IM; booster every 2 years | ~55% at 3 years |
| Typhoid Conjugate Vaccines (Typbar-TCV, TYPHIBEV) | Vi-polysaccharide conjugated | ≥6 months | Single IM dose; protection up to 7 years | 79-95% (WHO preferred) |
TCV (conjugate) is now the WHO-preferred vaccine and is recommended for countries with high incidence, especially for children <2 years (unconjugated Vi CPS not effective in this age group).
Quick Reference Decision Algorithm
Typhoid suspected
↓
Send: Blood cultures x3, stool/urine culture, Widal (low sensitivity), CBC, LFTs
↓
Travel history?
↓ ↓
Pakistan / Iraq / Other endemic area
No travel ↓
↓ Ceftriaxone IV (severe)
Uncomplicated: OR Azithromycin (mild)
Azithromycin 7 days
Severe:
Meropenem IV 10-14 days
↓
Culture & Sensitivity results available?
↓
Tailor therapy to susceptibility
↓
Temperature normal ≥2-3 days → step down to oral, complete course
↓
Monitor for relapse (especially within 4 weeks)
Key Exam Points
- MDR = resistant to ampicillin + chloramphenicol + TMP-SMX → treat with ceftriaxone or azithromycin
- XDR = MDR + resistant to fluoroquinolones + ceftriaxone → treat with meropenem ± azithromycin
- Do NOT use fluoroquinolones empirically for travelers from South Asia
- Dexamethasone only for delirium/coma/shock - 3 mg/kg then 1 mg/kg q6h x 48 hrs
- Perforation = laparotomy + broad-spectrum cover
- Chronic carrier treatment = ciprofloxacin x 28 days (or cholecystectomy if failed)
- Azithromycin has the lowest relapse rate of all regimens
confirmation of HIV in a new born
HIV confirmation newborn infant diagnosis virological testing PCR DNA RNA guidelines 2024
HIV newborn infant confirmation testing schedule DNA PCR RNA antibody maternal transfer 18 months
Confirmation of HIV in a Newborn
Why Standard Antibody Tests CANNOT Be Used in Infants < 18 Months
- A positive HIV antibody test in a newborn or infant < 18 months only confirms maternal HIV infection - it does NOT confirm infant infection
- A negative antibody test also does not confirm the infant is uninfected during this window
- Therefore, antibody tests (including 4th-generation Ag/Ab assays) must NOT be used to diagnose or exclude HIV in infants < 18 months
Guideline (US HHS 2024, AII recommendation): Virologic assays (HIV RNA or HIV DNA nucleic acid tests [NATs]) that directly detect HIV must be used to diagnose HIV in infants and children aged <18 months with perinatal HIV exposure.
Tests Used for Diagnosis in Newborns/Infants < 18 Months
1. HIV DNA PCR (Most widely used)
- Detects intracellular HIV viral DNA in peripheral blood mononuclear cells (PBMCs)
- Does NOT depend on active viral replication
- Specificity: 99.8% at birth; 100% at 1, 3, and 6 months
- Sensitivity by age:
| Age | Sensitivity (HIV DNA PCR) |
|---|---|
| Birth (< 48 hrs) | 20-55% (detects only in utero infection) |
| 2-4 weeks | >90% |
| 3-6 months | 100% |
- Can be performed on dried blood spots (DBS) - useful in resource-limited settings
2. HIV RNA PCR (Quantitative / Qualitative)
- Detects extracellular viral RNA in plasma
- Equally recommended alongside HIV DNA PCR (AII)
- Specificity: 100% at birth, 1, 3, and 6 months
- Same sensitivity profile as DNA PCR
- Also gives baseline viral load (useful for treatment decisions)
- Preferred for detecting non-subtype B HIV (Group O, HIV from Africa/SE Asia) - important for immigrants
3. HIV RNA Qualitative Assay (APTIMA HIV-1 RNA Qualitative Assay)
- FDA-approved alternative diagnostic test for infants
- Can be used when initial DNA PCR is positive (for confirmation)
4. HIV p24 Antigen Test
- Detects viral capsid protein
- NOT recommended for newborn diagnosis in the US - sensitivity and specificity inferior to NATs in the first months of life
- Used in resource-limited settings where PCR unavailable
5. HIV Antibody Test (ELISA / 4th gen Ag/Ab)
- NOT used for diagnosis in < 18 months (maternal antibody interference)
- Used only after 18 months to confirm loss of maternal antibodies (seroreversion = infant is uninfected)
Testing Schedule: Virologic (NAT) Testing
Official Schedule from Red Book 2021 (AAP) / HHS 2024 Guidelines
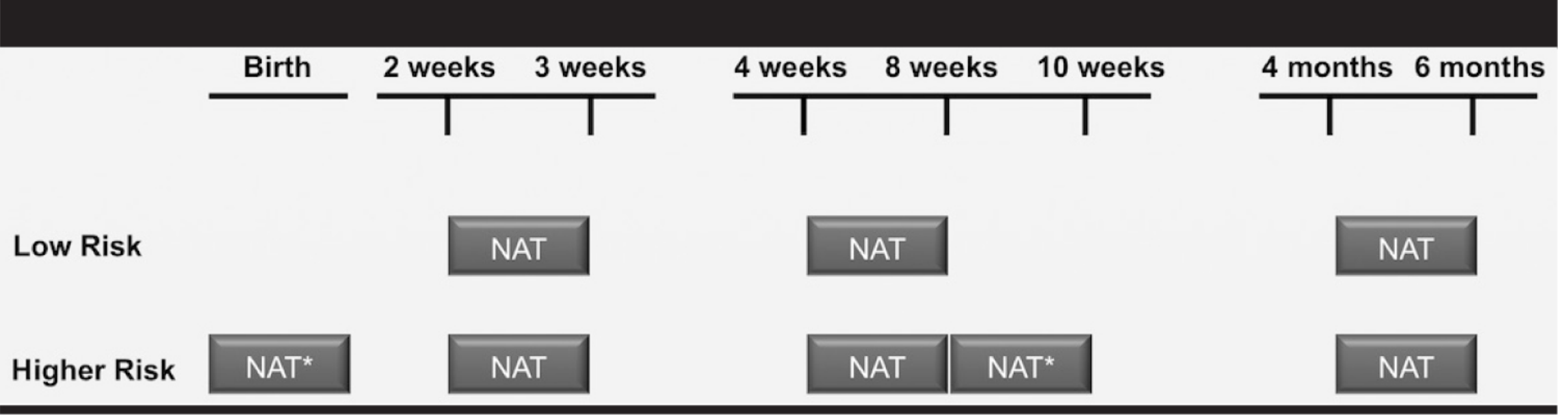
| Risk Category | Testing Timepoints |
|---|---|
| Low Risk | 2-3 weeks → 4-6 weeks → 4-6 months |
| Higher Risk | Birth → 2-3 weeks → 4-6 weeks → 8 weeks → 10 weeks (after ARV cessation) → 4-6 months |
- Had no prenatal care
- Received no antepartum/intrapartum ARVs
- Only received intrapartum ARVs
- Started ART late (late 2nd or 3rd trimester)
- Had acute HIV infection during pregnancy
- Had detectable viral load near delivery
Higher-risk infants: additional test at birth AND at 8-10 weeks (2-4 weeks after stopping ARV prophylaxis)
Interpreting Results: Positive vs. Negative
Confirming HIV INFECTION (Positive Diagnosis)
- Two separate positive virologic tests (HIV DNA PCR or RNA PCR) from two different blood samples at different time points
A single positive result is presumptive - always repeat immediately on a new sample before labelling infant as infected (false positives can occur with both RNA and DNA assays)
- Perform HIV RNA quantitative load (baseline viral load)
- Perform HIV genotype (resistance testing to guide ART choice)
- Initiate ART as soon as possible
Excluding HIV INFECTION (Negative Diagnosis - Non-Breastfeeding)
| Condition | Criteria |
|---|---|
| Age | ≥ 4-6 months |
| Tests | Two negative NAT results from samples at least 1 month apart (both after age 1 month) |
| Breastfeeding | Not breastfeeding (or breastfeeding stopped ≥6 weeks before testing) |
| Clinical | No HIV clinical symptoms |
- DNA PCR negative at ≥1 month AND at ≥4 months = HIV infection excluded (non-breastfed)
For Breastfed Infants
- Breastfeeding continues to pose transmission risk throughout the breastfeeding period
- Testing must be repeated 6 weeks after complete cessation of breastfeeding
- Cannot exclude HIV infection until 6 weeks post-weaning testing is negative
Final Confirmation at 18 Months (Antibody Seroreversion)
- All HIV-exposed infants (even those with negative PCRs) should have HIV antibody test at 18 months
- If antibody negative at 18 months: confirms HIV-uninfected (maternal antibodies have cleared)
- If antibody positive at 18 months: perform NAT to confirm true infection (rare - residual maternal antibodies can occasionally persist slightly longer)
Summary Algorithm
Newborn of HIV-positive mother
↓
DO NOT use HIV antibody test (maternal IgG interference)
↓
Use HIV DNA PCR or HIV RNA PCR (NAT)
↓
Higher risk → test at birth, 2-3 weeks, 4-6 weeks, 8 weeks, 4-6 months
Low risk → test at 2-3 weeks, 4-6 weeks, 4-6 months
↓
ANY POSITIVE RESULT?
YES ↓ NO ↓
Repeat immediately on Continue scheduled testing
new blood sample (2 negatives ≥1 month apart
↓ after age 1 month = excluded)
SECOND POSITIVE? ↓
YES → HIV CONFIRMED HIV antibody test at 18 months
↓ (confirms seroreversion)
HIV RNA viral load
HIV genotype (resistance)
Start ART urgently
Key Points Summary Table
| Feature | Detail |
|---|---|
| Why not antibody test? | Maternal IgG crosses placenta, persists 12-18 months |
| Preferred test | HIV DNA PCR or HIV RNA PCR (NAT) |
| Sensitivity at birth | 20-55% (only detects in utero infection) |
| Sensitivity at 1-2 months | >96% |
| Sensitivity at 3-6 months | 100% |
| Confirmatory rule | 2 positive NATs on separate samples = HIV confirmed |
| Exclusion rule | 2 negative NATs ≥1 month apart, both after age 1 month, not breastfeeding = excluded |
| Final serological check | HIV antibody at 18 months (expects negative = seroreversion) |
| Breastfeeding caveat | Test 6 weeks after cessation; breastfeeding transmits HIV |
| Non-subtype B / African HIV | Use RNA NAT or total nucleic acid test (DNA PCR may miss) |
| After confirmation | Viral load + genotype + ART initiation ASAP |
counselling regarding breast feeding in HIV postive mother
HIV positive mother breastfeeding counselling WHO CDC guidelines 2024 ART viral suppression transmission risk
HIV breastfeeding counselling resource rich resource limited settings WHO recommendation ART viral suppression formula feeding risk transmission
WHO 2022 2023 breastfeeding HIV guidelines resource limited settings AFASS criteria replacement feeding recommendation
Breastfeeding Counselling in HIV-Positive Mothers
The Core Dilemma
How HIV Transmits via Breast Milk
- HIV (both cell-free RNA and cell-associated virus) is present in breast milk
- Transmission can occur with each feed throughout the entire breastfeeding period
- Risk is highest in early months, and is continuous throughout breastfeeding
- Exclusive breastfeeding carries a lower risk than mixed feeding (adding water, formula, or solids alongside breast milk increases gut permeability and transmission risk)
Risk Factors for Higher HIV Transmission via Breast Milk
| Factor | Risk |
|---|---|
| Detectable HIV RNA in breast milk | High |
| Mastitis / cracked nipples / breast abscess | High (disrupts mucosal barrier) |
| Low maternal CD4 count | High |
| Maternal vitamin A deficiency | Higher |
| High maternal plasma viral load | Directly proportional |
| Mixed feeding (vs. exclusive breastfeeding) | Higher than exclusive |
| Oral lesions / sores in infant | Higher risk of mucosal entry |
Quantifying the Risk
- Untreated mother: 15-35% overall mother-to-child transmission risk; breastfeeding accounts for an additional 15-20% of infant HIV infections
- Mother on ART with undetectable viral load (<50 copies/mL): breastfeeding transmission risk <1% (but not zero)
- Plasma viral load <1000 copies/mL: transmission very unlikely
- Plasma viral load <50 copies/mL: transmission extremely unlikely
Important caveat: Low-level detectable HIV virus (<100 copies/mL) has been found in breast milk even when plasma viral load is undetectable - clinical significance for transmission is unknown but cannot be dismissed.
Part 1: RESOURCE-RICH SETTINGS (USA, UK, Canada, Europe, Australia)
Official Position (US HHS Panel 2024, CDC 2024, AAP 2024)
If Mother is NOT on ART or NOT Virally Suppressed
- Formula feeding or pasteurized donor human milk from a milk bank should be used
- Provide formula feeding support (preparation, barriers, financial assistance)
If Mother IS on ART with Sustained Undetectable Viral Load
| Body | Stance |
|---|---|
| CDC (2024) | Acknowledges <1% risk; patient-centered counselling; supports shared decision-making |
| US HHS Panel (2024) | Counsel about all three options: formula, donor milk, or breastfeeding; support whatever decision is made |
| AAP (2024) | Avoidance of breastfeeding is the ONLY 0% risk option; BUT pediatricians should offer "family-centered, non-judgmental, harm reduction approach" to support mothers on ART with sustained viral suppression (<50 copies/mL) who choose to breastfeed |
| Harrison's 22e (2025) | In developed countries, breast-feeding by an HIV-positive mother is contraindicated since alternative adequate nutrition is readily available |
| Creasy & Resnik Maternal-Fetal Medicine | HIV-positive mother listed under "Mothers should NOT breastfeed" (CDC 2018 criteria) |
What to tell the mother in a resource-rich setting:
- Formula feeding or pasteurized donor human milk completely eliminates the risk of HIV transmission through feeding
- If you are on ART with an undetectable viral load, the risk of transmitting HIV through breastfeeding is <1%, but not zero
- If you choose to breastfeed, you will need:
- Strict ART adherence throughout breastfeeding
- Regular viral load monitoring (every 1-3 months during breastfeeding)
- Infant HIV testing with NAT during and after breastfeeding period
- Infant ARV prophylaxis (specific regimen depends on risk level)
- To stop breastfeeding immediately if viral load becomes detectable
- Testing 6 weeks after cessation of breastfeeding
- If you choose not to breastfeed, you will be supported fully with formula preparation and feeding support
- Mixed feeding (breast + formula) is not recommended as it may increase transmission risk compared to exclusive breastfeeding
Part 2: RESOURCE-LIMITED SETTINGS (Sub-Saharan Africa, South/Southeast Asia, Latin America)
The WHO Position (WHO 2023)
- Formula feeding requires safe water, clean utensils, regular supply - often unavailable
- Formula-fed HIV-exposed infants in resource-limited settings have significantly higher mortality from diarrhoea and pneumonia
- Not breastfeeding signals HIV status and leads to stigma, discrimination, and social harm
WHO Recommendation:
"Mothers living with HIV should breastfeed for at least 12 months and may continue for up to 24 months or beyond (similar to the general population) while being fully supported for ART adherence."
AFASS Criteria - Before Recommending Replacement Feeding in Resource-Limited Settings
| AFASS | Criteria | Question to Ask |
|---|---|---|
| Acceptable | No social or cultural barrier to not breastfeeding | "Will there be a problem with family/community if you don't breastfeed?" |
| Feasible | Mother/family can prepare and give formula correctly | "Can you prepare feeds every 3 hours, day and night?" |
| Affordable | Can sustain cost for 6+ months without compromising nutrition | "Can you buy enough formula consistently?" |
| Sustainable | Continuous uninterrupted supply available | "Is formula reliably available in your area?" |
| Safe | Access to clean water + ability to sterilize utensils | "Do you have access to clean, safe water? Can you sterilize utensils?" |
WHO Breastfeeding Guidance in Resource-Limited Settings:
- Exclusively breastfeed for first 6 months (no water, formula, or solids)
- Continue breastfeeding with complementary foods from 6 months onwards
- Breastfeed for at least 12 months - can continue to 24 months (while on ART)
- Continue maternal ART throughout breastfeeding period (not just during pregnancy)
- Weaning should be gradual (over several weeks) - abrupt weaning risks mastitis and increased transmission; sudden weaning also puts infant at risk of malnutrition
- After weaning: test infant 6 weeks post-cessation
Counselling Framework - Practical Points for ALL Settings
When to Begin Counselling
- Before conception (if patient known HIV-positive and planning pregnancy)
- As early as possible in pregnancy (first antenatal visit)
- Reviewed throughout pregnancy
- Again after delivery (update plan, re-discuss, confirm readiness)
Key Counselling Messages
| Message | Detail |
|---|---|
| ART is essential | Start and maintain ART - this is the single most important intervention to protect the infant |
| Viral suppression = key | Mother must achieve and maintain undetectable viral load |
| Exclusive breastfeeding is safer than mixed | If breastfeeding in resource-limited setting, give ONLY breast milk for first 6 months |
| Mastitis must be treated promptly | Seek treatment immediately - mastitis increases HIV transmission risk; continue breastfeeding from unaffected side if needed |
| Cracked/bleeding nipples | Consider temporarily stopping breastfeeding from affected breast; express and discard milk from that side |
| No premastication of food | Mothers with HIV should never pre-chew food for their infant (HIV in saliva + mucosal exposure to infant) |
| Infant ARV prophylaxis | Infant receives ARVs for 4-6 weeks (or longer if breastfeeding) |
| Infant testing | Regular HIV NAT testing of infant throughout and after breastfeeding |
| Partner notification | Ensure partner knows status; test partner |
| No breast milk donation | Mother with HIV must not donate breast milk to a milk bank |
| Pasteurized donor milk | In resource-rich settings, pasteurized donor human milk from a bank is a safe alternative to formula |
Stopping Breastfeeding - Guidance
When to Stop Immediately (Resource-Rich Settings):
- Maternal viral load becomes detectable during breastfeeding
- Mastitis not responding to treatment
- Bleeding/cracked nipples not resolving
- Mother decides to stop ART
How to Wean (Gradual Weaning Recommended):
- Reduce frequency gradually (e.g., once every 4-6 hours, then once daily, then stop) over several days to weeks
- During transition: use cup feeding with formula or expressed heat-treated milk
- Do not abruptly stop (risk of mastitis → increases transmission risk during transition)
- After cessation: test infant with HIV NAT at 6 weeks post-weaning
Summary Comparison Table
| Aspect | Resource-Rich Setting | Resource-Limited Setting |
|---|---|---|
| Primary recommendation | Avoid breastfeeding (formula or donor milk) | Breastfeed exclusively for 6 months with ART |
| If ART + viral suppression | Counselling + shared decision-making; can support if mother chooses | Continue breastfeeding up to 24 months with ART |
| If no ART or not suppressed | Formula/donor milk ONLY | Try to achieve ART; use AFASS to guide |
| Key protective factor | Formula/pasteurized donor milk | Maternal ART + exclusive breastfeeding |
| Risk reduction with ART | <1% transmission risk | <1-2% transmission risk |
| Duration | Avoid entirely (ideally) | 12-24 months with ART |
| Mixed feeding | Not recommended | Never - increases risk |
| Infant prophylaxis | 4-6 weeks ARV | Extended ARV prophylaxis during breastfeeding |
| Post-weaning test | 6 weeks after stopping | 6 weeks after stopping |
| Guideline bodies | CDC, HHS, AAP, Harrison's | WHO, UNICEF, UNAIDS |
Non-Judgmental, Patient-Centered Approach (2024 Emphasis)
- Shared decision-making - the mother's informed choice is respected
- Non-judgmental counselling - no stigma for choosing either option
- Cultural sensitivity - especially around stigma in communities where not breastfeeding "reveals" HIV status
- Health equity lens - barriers to breastfeeding and formula feeding must both be addressed
- Support regardless of choice - if she breastfeeds, support safe breastfeeding; if she formula feeds, support preparation and access