Episcleritis sceleritis conjunctivitis difference ak khurana
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I have rich content. Note: The library has Kanski's Clinical Ophthalmology (10th edition) but not AK Khurana specifically — however, the content from Kanski's is the authoritative ophthalmology reference. Let me now compile a comprehensive comparison.
Episcleritis vs Scleritis vs Conjunctivitis — Differential Comparison
Note: AK Khurana's Comprehensive Ophthalmology is not in this library's collection; the following is drawn from Kanski's Clinical Ophthalmology (10th ed.) and Rosen's Emergency Medicine, which cover this topic authoritatively and align with Khurana's teaching.
Anatomical Basis — Key to Understanding the Difference
Fig. 9.1 (A) Episcleritis — maximal vascular congestion in the superficial episcleral plexus:
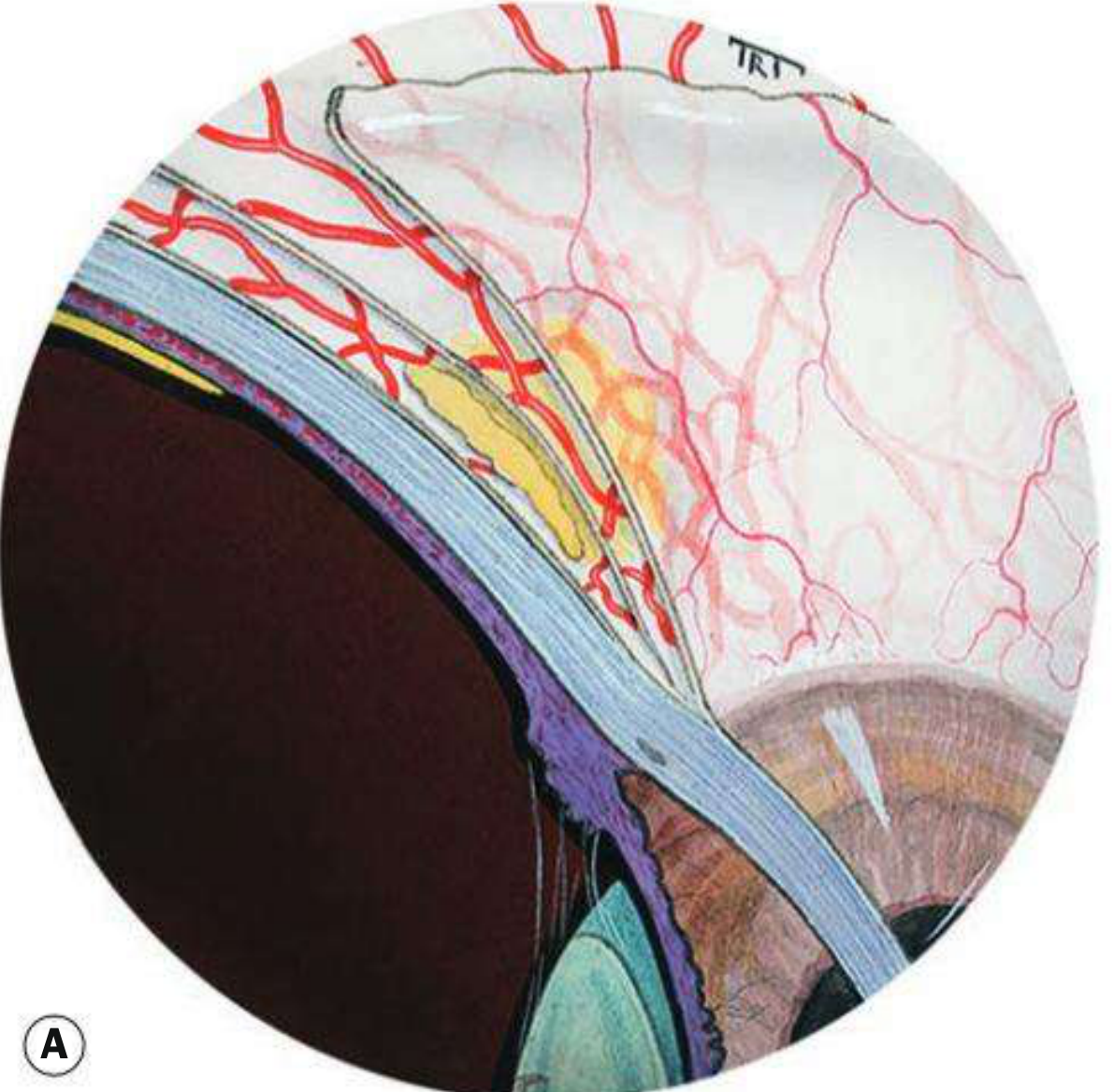
Fig. 9.1 (B) Scleritis — scleral thickening with maximal congestion in the deep vascular plexus:
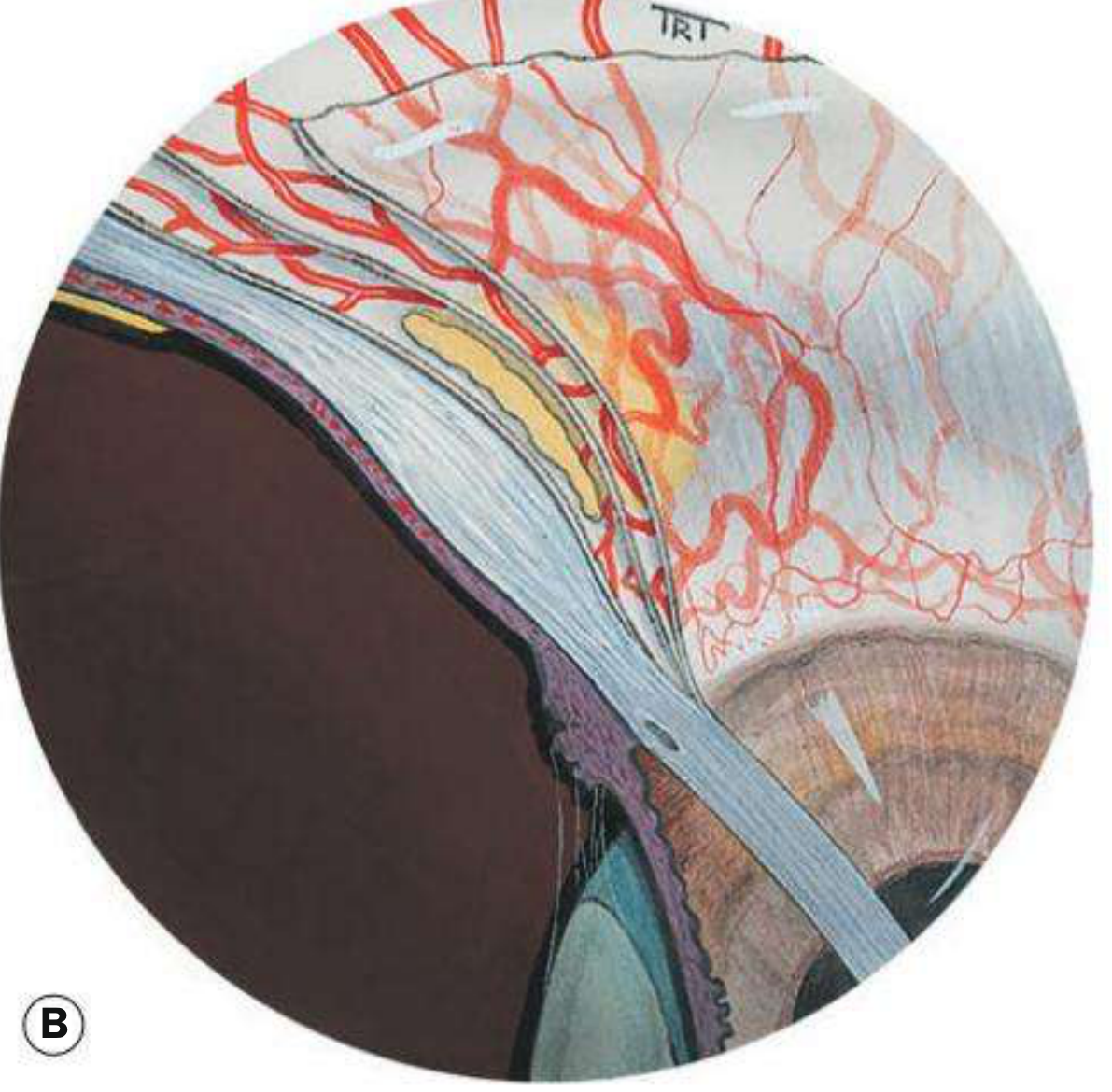
There are three vascular layers anterior to the equator:
- Conjunctival vessels — most superficial; arteries tortuous, veins straight
- Superficial episcleral plexus — straight, radial; congested in episcleritis
- Deep scleral vascular plexus — congested in scleritis; produces the characteristic purplish hue
Comparison Table
| Feature | Conjunctivitis | Episcleritis | Scleritis |
|---|---|---|---|
| Layer involved | Conjunctiva only | Episclera (between conjunctiva & Tenon's capsule) | Full thickness of sclera |
| Colour of redness | Bright red / pink | Salmon-pink to bright red | Deep purple-red/blue-red hue (best seen in daylight) |
| Discharge | Prominent (watery, mucoid, or purulent) | None | None |
| Pain | Gritty / foreign body sensation | Mild discomfort to grittiness; up to 50% painless | Severe, boring, deep pain radiating to temple, brow, jaw; nocturnal, wakes patient; poor response to analgesia |
| Tenderness | None | Mild, if any | Globe tenderness on palpation |
| Nodule | None | Present in nodular type (moveable over sclera) | Present in nodular type (immovable, elevated on slit-lamp) |
| Visual acuity | Normal | Normal | May be reduced |
| Photophobia | May be present | Occasional | Common |
| Chemosis | Common | Rare | Can occur |
| Anterior uveitis | No | Very rare | Can occur as complication |
| Phenylephrine 10% test | Blanches vessels | Blanches superficial episcleral vessels | Does NOT blanch deep plexus vessels |
| Phenylephrine 2.5% test | Blanches conjunctival & superficial episcleral | Blanches | Does not blanch deep plexus |
| Slit-lamp beam | No displacement | Deep beam not displaced above scleral surface | Deep beam elevated (anterior scleral surface raised) |
| Systemic associations | Usually infectious; no major systemic disease | Minority: RA, gout, IBD, HZV, rosacea | Strongly associated: RA, Wegener's (GPA), polyarteritis nodosa, SLE, IBD, ankylosing spondylitis |
| Course | Self-limiting (days) | Self-limiting; lasts days to 3 weeks; recurrent | Chronic, mean ~6 years; can progress to necrotizing |
| Visual threat | Rare (corneal complications) | No | Yes — can cause scleral necrosis, uveitis, cataract, glaucoma, vision loss |
| Treatment | Topical antibiotics / antivirals; antihistamines | Cool compresses; topical steroid or NSAID; oral NSAID occasionally | Oral NSAIDs → oral corticosteroids → immunosuppressants (methotrexate, azathioprine) → biologics (adalimumab, infliximab) |
Episcleritis in Detail

Types:
- Simple episcleritis (75%): Sectoral or diffuse redness; peaks at 24 hrs, fades over days; frequently bilateral (>50%); recurrent in 60%
- Nodular episcleritis (25%): More prolonged; node is tender, salmon-pink, moveable over sclera; no slit-lamp elevation of deep beam
Key point: Topical phenylephrine 2.5% constricts conjunctival and superficial episcleral vessels → redness blanches in episcleritis.
Scleritis in Detail
Classification (Immune-mediated / Non-infectious):
| Anterior | Posterior |
|---|---|
| Non-necrotizing: Diffuse, Nodular | Less common |
| Necrotizing with inflammation: Vaso-occlusive, Granulomatous, Surgically induced | |
| Scleromalacia perforans (necrotizing without inflammation) |
Scleromalacia perforans — occurs in long-standing RA; painless progressive scleral necrosis; no active inflammation; treatment is largely unsatisfactory.
Necrotizing scleritis is the most dangerous form — severe pain, bilateral in 60%, can destroy the eye without systemic immunotherapy.
The Phenylephrine Blanching Test (Khurana's Key Differentiator)
| Test | Conjunctivitis | Episcleritis | Scleritis |
|---|---|---|---|
| 2.5% phenylephrine | Blanches (constricts conjunctival + superficial episcleral) | Blanches | No blanching of deep plexus |
| 10% phenylephrine | Blanches all superficial vessels | Blanches | No blanching |
This is the bedside test taught by Khurana: in scleritis the deep plexus is involved and does not blanch with phenylephrine, confirming the deeper pathology.
Quick Memory Aid
Conjunctivitis → Clear discharge, Conjunctival layer, Comfort mostly intact
Episcleritis → Episcleral layer, no discharge, Easily blanches, Excellent prognosis
Scleritis → Severe pain, Systemic disease, Scleral layer, Sight-threatening
— Kanski's Clinical Ophthalmology, 10th ed. (Ch. 9: Episclera and Sclera); Rosen's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.