Lab diagnostic test of cancer
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Loading Image
Reading File
I now have rich, comprehensive content from the textbooks. Let me compile the full answer.
Laboratory Diagnostic Tests of Cancer
The laboratory diagnosis of cancer involves multiple complementary approaches - from traditional morphologic methods to advanced molecular techniques. Every year this field becomes more complex and personalized, allowing therapy tailored to the molecular characteristics of the individual tumor.
1. Morphologic / Histologic Methods
These are the cornerstone of cancer diagnosis.
A. Biopsy and Histologic Examination (H&E Staining)
- Tissue is removed (excisional biopsy, incisional biopsy, or core needle biopsy), fixed in formalin, sectioned, and stained with hematoxylin and eosin.
- Allows assessment of tumor architecture, cell morphology, and degree of anaplasia (loss of differentiation).
- Frozen section - freshly removed tissue is quick-frozen and sectioned for histology within minutes. Used intraoperatively to assess surgical margins or lymph node status. Standard permanent sections provide superior detail when critical decisions (e.g., amputation) are at stake.
- Clinical data (radiation exposure, fracture history, imaging findings) must accompany specimens - radiation changes can mimic cancer, healing fractures can mimic osteosarcoma.
B. Fine Needle Aspiration (FNA)
- A small-bore needle aspirates cells from palpable or image-guided masses.
- Cells are spread on a slide, stained, and examined cytologically.
- Widely used for breast, thyroid, lymph node, salivary gland, liver, pancreas, and pelvic lymph node lesions.
- Advantages: minimally invasive, rapid, avoids surgery.
- Limitations: small sample, potential sampling error; requires experienced hands.
C. Cytologic Smears (Papanicolaou/Pap Test)
- Exfoliated cells from surfaces or fluids are collected, smeared, fixed, and stained.
- Classic use: cervical carcinoma screening (Pap smear) - the best testament to the value of cytology in cancer control.
- Also used for: urine (bladder cancer), bronchial washings/brushings (lung cancer), sputum, CSF, pleural/peritoneal effusions, endometrial cells.
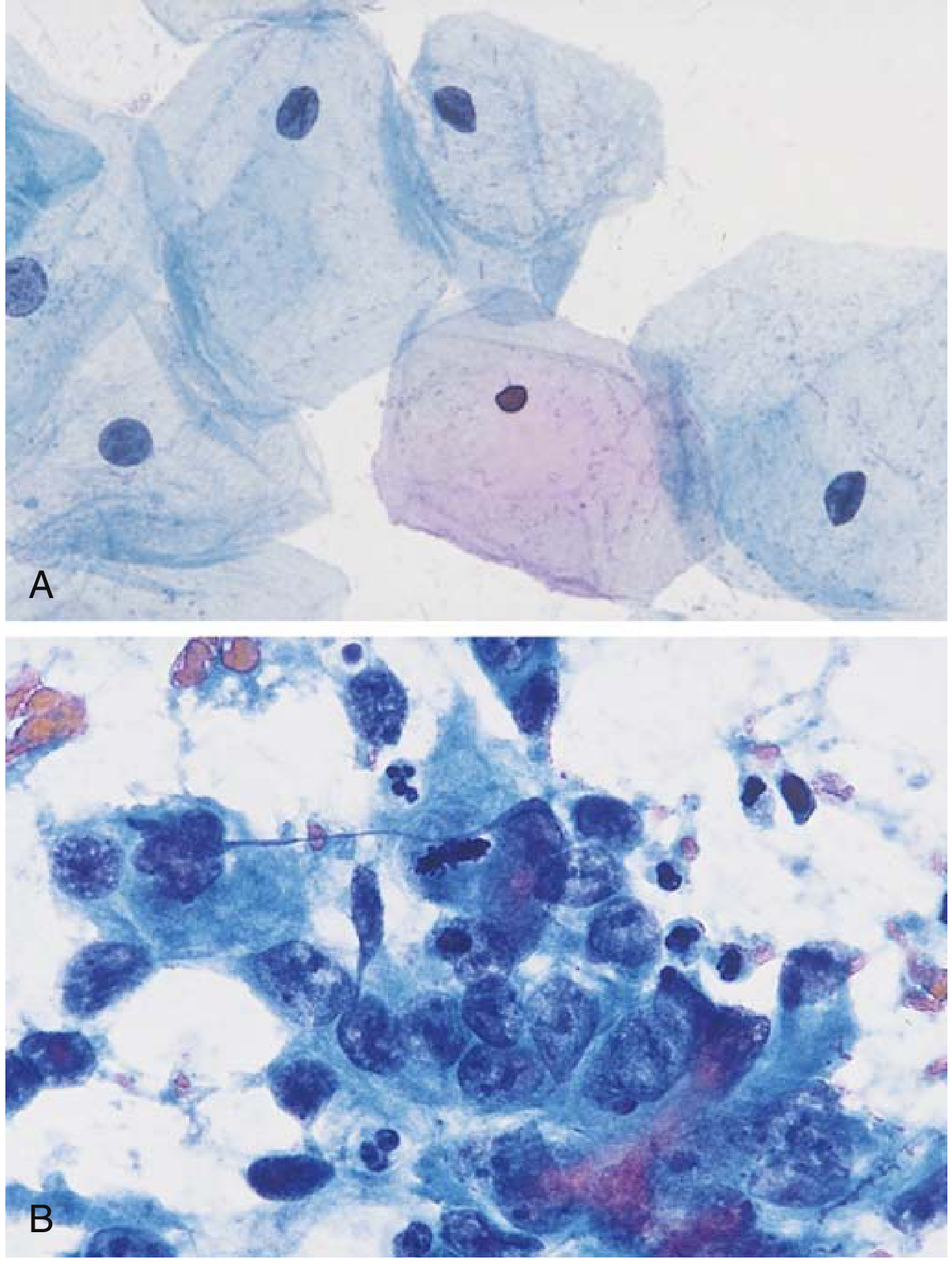
- Cancer cells show features of anaplasia: nuclear pleomorphism, increased N:C ratio, irregular chromatin, prominent nucleoli, abnormal mitoses.
Below: Normal (A) vs. malignant (B) Papanicolaou smear - note the dramatic nuclear enlargement, hyperchromasia, and irregular cell shapes in the malignant sample:
2. Immunohistochemistry (IHC)
IHC uses monoclonal antibodies against specific antigens on tissue sections. It is a powerful adjunct to routine H&E staining.
Key uses:
| Application | Example |
|---|---|
| Categorize undifferentiated (anaplastic) tumors | Cytokeratin → carcinoma; CD45 → lymphoma; SOX10 → melanoma; Desmin → muscle tumors |
| Identify primary site of metastatic tumors | PSA → prostate origin; Thyroglobulin → thyroid origin |
| Therapeutic targets and prognosis | HER2/ERBB2 in breast cancer (directs trastuzumab therapy); ER/PR in breast cancer (directs antiestrogen therapy); ALK in lung cancer/lymphoma (directs ALK inhibitors) |
| Identify pathogens | EBV, HPV by in-situ hybridization alongside IHC |
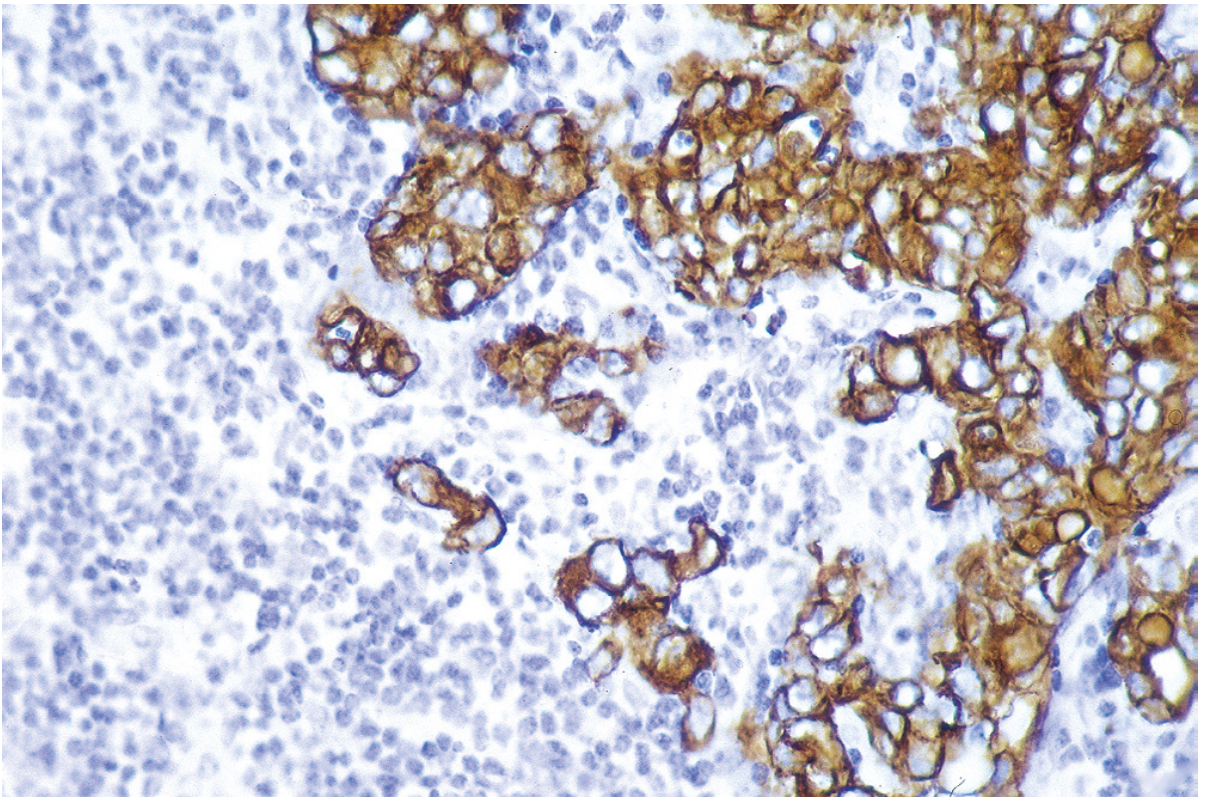
Below: Anti-cytokeratin immunoperoxidase stain - brown-stained clusters are carcinoma cells amid blue lymphocytes, confirming epithelial (carcinoma) origin:
3. Tumor Markers (Serum / Biochemical Tests)
Tumor markers are substances present in abnormally high concentrations in blood, urine, or other body fluids in cancer patients. They are produced by tumor cells directly or by the body in response to the tumor.
Important: Biochemical tumor markers lack the sensitivity and specificity for definitive cancer diagnosis on their own. Their main value is in monitoring response to therapy and detecting recurrence. With successful tumor resection, markers disappear; their reappearance almost always signals recurrence.
Major Tumor Markers
| Category | Marker | Associated Cancer | Notes |
|---|---|---|---|
| Hormones | hCG (human chorionic gonadotropin) | Trophoblastic tumors, non-seminomatous testicular tumors | Also elevated in normal pregnancy |
| Calcitonin | Medullary carcinoma of thyroid | Screening in MEN2 families | |
| Catecholamines / vanillylmandelic acid (VMA) | Pheochromocytoma, neuroblastoma | Urine VMA/HVA | |
| ACTH, PTHrP, ADH | Various (ectopic hormone syndromes) | Paraneoplastic | |
| Oncofetal Antigens | AFP (alpha-fetoprotein) | Hepatocellular carcinoma, yolk sac tumors, embryonal carcinoma | Elevated in liver disease, pregnancy |
| CEA (carcinoembryonic antigen) | Colon, pancreas, lung, stomach, breast cancer | Elevated in smokers, IBD, cirrhosis | |
| Lineage-Specific Proteins | PSA (prostate-specific antigen) | Prostate cancer | Also elevated in BPH, prostatitis |
| PSMA | Prostate cancer | PET imaging target | |
| Immunoglobulins (M protein) | Multiple myeloma, Waldenström macroglobulinemia | Serum + urine electrophoresis | |
| Mucins / Glycoproteins | CA-125 | Ovarian cancer, fallopian tube, colon | Elevated in endometriosis, PID |
| CA-19-9 | Pancreatic cancer, GI/hepatobiliary tumors | Not Lewis antigen-negative individuals | |
| CA-15-3 | Breast cancer | Monitoring metastatic disease | |
| Enzymes | LDH (lactate dehydrogenase) | Lymphoma, testicular tumors, many cancers | Non-specific; staging marker |
| ALP (alkaline phosphatase) | Bone/liver metastases, osteosarcoma | ||
| Acid phosphatase | Prostate cancer (historical) | Superseded by PSA | |
| NSE (neuron-specific enolase) | Small cell lung cancer, neuroblastoma | ||
| Cell-free DNA | EGFR mutations in serum | Lung cancer | Liquid biopsy |
| TP53, APC, RAS mutations in stool/serum | Colon cancer |
4. Flow Cytometry
- Rapidly and quantitatively measures multiple cell characteristics simultaneously using fluorescently labeled antibodies.
- Requires viable cells in suspension.
- Primarily used for hematologic malignancies: B-cell and T-cell lymphomas, leukemias (CLL, AML, ALL).
- Multiple antigens (CD markers) assessed simultaneously on individual cells - this is an advantage over IHC.
- Identifies cell lineage, differentiation stage, and aberrant antigen expression patterns that define specific leukemia/lymphoma subtypes.
- Also used for DNA ploidy analysis (aneuploidy suggests malignancy) and S-phase fraction (proliferative index).
5. Molecular Diagnostic Methods
Molecular techniques are now standard in many cancer centers.
A. Polymerase Chain Reaction (PCR)
- Lymphoma/leukemia diagnosis: Each B/T cell has unique antigen receptor gene rearrangements. PCR detects clonal (neoplastic) vs. polyclonal (reactive) lymphocyte populations.
- Specific translocations: BCR-ABL transcripts confirm CML diagnosis; JAK2 V617F mutations confirm polycythemia vera.
- Minimal residual disease (MRD) detection: Ultra-sensitive PCR detects residual BCR-ABL transcripts after CML treatment, guiding therapy decisions.
B. Fluorescence In Situ Hybridization (FISH)
- Detects specific chromosomal translocations, deletions, and amplifications.
- Examples:
- t(11;22) in Ewing sarcoma
- t(14;18) in follicular lymphoma
- HER2 (ERBB2) gene amplification in breast cancer (guides trastuzumab therapy)
- MYCN amplification in neuroblastoma (poor prognosis)
- ALK rearrangements in lung adenocarcinoma and anaplastic large cell lymphoma
C. DNA Sequencing / Next Generation Sequencing (NGS)
- Sequencing of cancer genomes is now routine in many centers.
- Identifies point mutations in cancer driver genes: TP53, KRAS, BRAF, EGFR, PIK3CA, etc.
- Predicts prognosis (TP53 mutation → poor outcome in many cancers).
- Identifies druggable targets: EGFR mutations (erlotinib/gefitinib), BRAF V600E (vemurafenib), etc.
D. Liquid Biopsy
- Detection of circulating tumor DNA (ctDNA) or circulating tumor cells (CTCs) in peripheral blood.
- Non-invasive; useful for monitoring treatment response and detecting early resistance.
- EGFR T790M mutation in plasma - guides second-line therapy in NSCLC.
- Stool DNA testing (APC, KRAS, RAS mutations + occult blood) - FDA-approved for colorectal cancer screening (Cologuard).
E. Microarray / Gene Expression Profiling
- Measures expression of thousands of genes simultaneously.
- Used for prognosis: Oncotype DX (21-gene assay) in breast cancer predicts recurrence risk and guides chemotherapy decisions; MammaPrint (70-gene signature).
- Identifies molecular subtypes of lymphoma (GCB vs. activated B-cell DLBCL).
6. Grading and Staging (Laboratory-Assisted)
- Grading (I-IV) assesses degree of differentiation and mitotic activity - done histologically.
- Staging (TNM system) assesses extent of spread - uses histology of biopsies (sentinel lymph node biopsy) and molecular markers.
7. Special Stains and Cytochemistry
| Stain | Purpose |
|---|---|
| PAS (Periodic acid-Schiff) | Glycogen-rich tumors (clear cell RCC, Ewing sarcoma) |
| Sudan black / Myeloperoxidase | AML diagnosis (myeloid lineage) |
| Oil red O | Liposarcoma, lipoblasts |
| Reticulin stain | Hepatocellular carcinoma vs. metastatic carcinoma |
| Congo red | Amyloid in plasma cell tumors |
8. Microbiology / Serology in Cancer Diagnosis
- HPV testing (PCR / hybrid capture): cervical cancer screening alongside Pap smear.
- H. pylori testing: gastric cancer / MALT lymphoma.
- EBV serology/PCR: EBV-associated Burkitt lymphoma, nasopharyngeal carcinoma, post-transplant lymphoproliferative disorder.
- HBV/HCV serology: hepatocellular carcinoma risk.
Summary: Which Test for Which Purpose
| Purpose | Best Test |
|---|---|
| Initial tissue diagnosis | Biopsy + H&E histology |
| Undifferentiated tumor classification | IHC panel |
| Cervical cancer screening | Pap smear + HPV testing |
| Monitoring therapy response / recurrence | Tumor markers (CEA, PSA, AFP, CA-125, etc.) |
| Hematologic malignancy immunophenotyping | Flow cytometry |
| Translocation-based leukemia/lymphoma diagnosis | PCR / FISH |
| Therapeutic target identification | NGS / IHC (HER2, ALK, EGFR, PD-L1) |
| Minimal residual disease | PCR (BCR-ABL) |
| Non-invasive cancer monitoring | Liquid biopsy (ctDNA) |
Sources: Robbins, Cotran & Kumar - Pathologic Basis of Disease (Table 7.12, pp. 309-318) | Robbins & Kumar Basic Pathology (pp. 257-261) | Tietz Textbook of Laboratory Medicine, 7th Ed. (Ch. 33, p. 1011)
This is a shared conversation. Sign in to Orris to start your own chat.