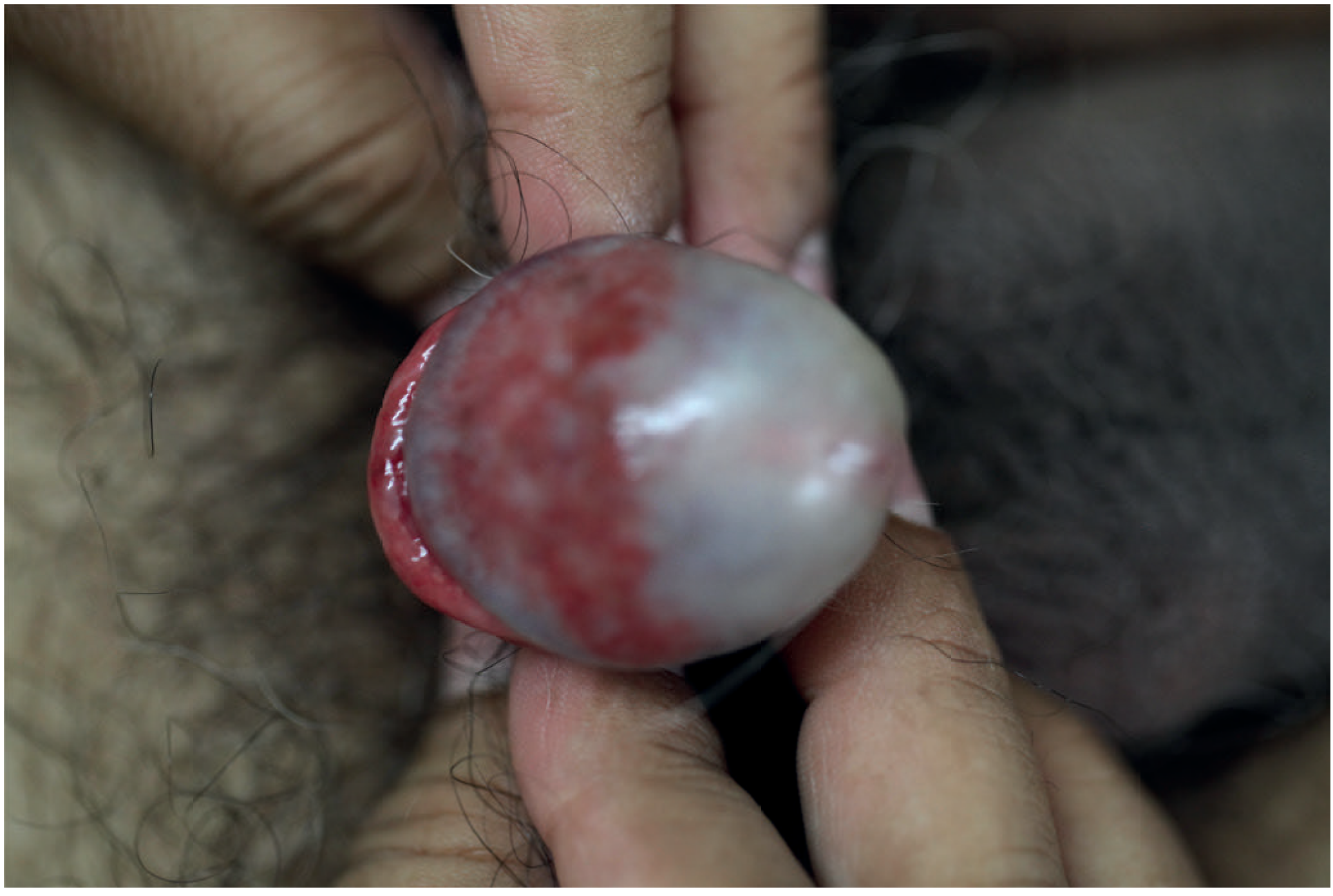
Pus at tip of penis in a 3 year old
Reading File
Finding Sources
Finding Sources
Searching the Web
balanitis child 3 year old pus penis treatment management pediatric
Finding Sources
Reading Web Page
https://pedemmorsels.com/pediatric-balanitis-and-balanoposth…
Finding Sources
Reading Web Page
https://emedicine.medscape.com/article/777026-treatment
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I have everything needed for a thorough answer.
Pus at the Tip of the Penis in a 3-Year-Old - Clinical Overview
Most likely diagnosis: Balanoposthitis (inflammation of the glans + foreskin), with purulent discharge indicating a bacterial infection.
Definition
Balanitis = inflammation of the glans penis.
Balanoposthitis = inflammation of both the glans AND the overlying prepuce (foreskin). The term balanoposthitis is used when both surfaces are involved - which is the typical picture when pus is seen at the tip.
Why Does It Happen in a 3-Year-Old?
At age 3, physiologic phimosis (non-retractile foreskin) is still very common - approximately 50% of boys still have it at age 1, and 89% resolve by age 3, meaning a proportion still have it beyond 3. The non-retractile foreskin traps smegma and moisture, creating a warm, moist environment for bacterial overgrowth.
Key causes in this age group:
| Category | Examples |
|---|---|
| Most common | Poor hygiene, accumulated sebaceous secretions |
| Bacterial | Staph. aureus, Strep. pyogenes, anaerobes, gram-negatives |
| Fungal | Candida albicans (less common in this age, more if on antibiotics or in diapers) |
| Chemical/Contact | Soap, detergent, bubble bath irritants |
| Associated condition | Physiologic phimosis (traps secretions) |
- Campbell-Walsh-Wein Urology: "In children, bacterial infections are the predominant cause."
- Rosen's Emergency Medicine: "The majority of cases are due to poor hygiene, with accumulated sebaceous material leading to bacterial or fungal overgrowth."
Clinical Presentation
- Redness and swelling of the glans and foreskin
- Purulent (pus) discharge from the preputial opening - the primary complaint here
- Pain and tenderness
- Dysuria (crying on urination, holding urine)
- Occasionally fever if secondary cellulitis develops
- "Ballooning" of foreskin on urination if phimosis is present
Diagnosis
The diagnosis is clinical - based on history and physical exam. No routine investigations needed unless:
- Dysuria present → urinalysis and urine culture (to rule out UTI)
- Recurrent episodes → glucose level (rule out diabetes, rare in this age)
- Discharge is profuse or there are extragenital findings → consider STI screen (important - see red flag below)
⚠️ IMPORTANT RED FLAG: Child Sexual Abuse
Pus/discharge from the penis of a 3-year-old must prompt consideration of sexual abuse. While the vast majority of cases are due to poor hygiene and physiologic phimosis, STI pathogens (Neisseria gonorrhoeae, Chlamydia trachomatis) in a prepubertal child are strong indicators of abuse. A thorough, sensitive history must be taken. If STI is identified or abuse is suspected, mandatory reporting and child protection services referral is required.
Management
Step 1 - Hygiene education (first-line for all cases)
- Gentle warm water soaks (sitz baths) 2-3x daily
- Do NOT forcibly retract the foreskin - causes trauma
- Keep area clean and dry; loose-fitting clothing
Step 2 - Topical treatment (for mild-moderate cases)
- Topical bacitracin - for bacterial coverage
- Topical nystatin or clotrimazole - for fungal coverage
- Hydrocortisone 0.5% cream twice daily - to reduce inflammation
Per Rosen's Emergency Medicine: "Treatment should include coverage for both bacterial and fungal overgrowth, with topical bacitracin and topical nystatin (or clotrimazole), respectively. Inflammation can be managed with 0.5% hydrocortisone cream twice daily."
Step 3 - Oral antibiotics (if cellulitis present)
- Cephalexin 25-50 mg/kg/day in divided doses for 7 days - for overlying mild cellulitis
- If cellulitis is moderate-to-severe or systemic signs → admit for IV antibiotics
Step 4 - Topical steroid for phimosis (age >3 years)
- Betamethasone 0.05% cream, gentle application twice daily for 4-8 weeks
- Helps resolve physiologic phimosis and allows better hygiene
- Note: Medscape states this applies to children older than 3 years specifically
When to Admit / Refer
| Indication | Action |
|---|---|
| Unable to urinate | Admit + urgent urology consult |
| Fever / systemic illness | Admit for IV antibiotics + urology |
| Moderate-severe cellulitis | Admit |
| Concern for sexual abuse | Immediate safeguarding referral |
| Recurrent episodes (3+ times) | Elective urology referral for circumcision consideration |
Prognosis and Follow-Up
Most cases resolve within 3-7 days with adequate treatment. The parents should be counseled that:
- Circumcision is NOT indicated as a preventive measure at age 3 (per Medscape/AAP guidance)
- If episodes recur, a urology referral is warranted - circumcision may be curative in recurrent balanoposthitis with phimosis
- Forced foreskin retraction should be strictly avoided as it causes scarring
Sources:
- Rosen's Emergency Medicine, 10th ed. (Balanoposthitis chapter)
- Bailey & Love's Short Practice of Surgery, 28th ed., p. 9988
- Campbell-Walsh-Wein Urology, 3-Volume Set, p. 1691
- Medscape Balanitis Treatment & Management - 2025 update
This is a shared conversation. Sign in to Orris to start your own chat.