Tell me about peptic ulcer
Reading File
Finding Sources
Searching PubMed
"peptic ulcer"[MeSH Terms] AND ("Helicobacter pylori" OR "treatment")
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have all the material needed for a thorough, well-illustrated answer. Here it is:
Peptic Ulcer Disease (PUD)
Definition
A peptic ulcer is a break in the mucosal lining of the gastrointestinal tract where it is exposed to acid and pepsin. Despite the name, acid is the essential factor - in its complete absence, peptic ulcers do not form, and nearly all can be healed with proton pump inhibitors (PPIs) that render a patient virtually achlorhydric. - Bailey and Love's Short Practice of Surgery, 28th ed.
Epidemiology
- More than 4 million individuals in the United States are treated for PUD each year
- Lifetime risk: ~10% for males, ~4% for females
- Duodenal ulcers are more common than gastric ulcers
- The peak incidence has shifted to older age groups in Western countries
- Still common in Eastern Europe and rising in resource-poor nations
- Robbins & Kumar Basic Pathology
Sites
| Location | Key Detail |
|---|---|
| First part of duodenum | Most common overall |
| Gastric antrum / lesser curve | Especially at the incisura angularis |
| Prepyloric / pyloric channel | Behave like duodenal ulcers |
| Esophagus | Acid reflux (GERD) or ectopic gastric mucosa |
| Meckel's diverticulum | Ectopic gastric epithelium |
| Stomal ulcers | After gastroenterostomy / Billroth II gastrectomy |
Ulcers typically occur at the junction between two different epithelial types - in the epithelium least resistant to acid damage. - Bailey and Love
Etiology and Pathogenesis
The core mechanism is an imbalance between mucosal damaging forces and protective defenses.
The Two Main Causes
1. Helicobacter pylori infection
- Responsible for >70% of PUD cases globally
- Only 5-10% of infected individuals actually develop ulcers, suggesting host factors and strain variation matter
- Causes chronic gastritis as a background to ulcer development
2. NSAID use
- In the United States, NSAID use is now becoming the most common cause of gastric ulcers as H. pylori infection rates fall
- Low-dose aspirin use in the aging population is a major contributor
- NSAIDs suppress prostaglandin synthesis, impairing mucosal defense
Other Contributing Factors
| Factor | Mechanism |
|---|---|
| Cigarette smoking | Reduces mucosal blood flow, increases relapse rate |
| Zollinger-Ellison syndrome | Gastrin-secreting tumor → massive acid secretion → multiple ulcers in stomach/duodenum/jejunum |
| Hyperparathyroidism | Hypercalcemia stimulates gastrin → increased acid |
| Chronic renal failure | Similar hypercalcemia-driven mechanism |
| High-dose corticosteroids | Suppress prostaglandin synthesis, impair healing |
| Alcohol-related cirrhosis, COPD | Associated increased risk |
Robbins & Kumar Basic Pathology; Bailey and Love
Pathology
Duodenal Ulcers
- Most ulcers occur in the first part of the duodenum
- A chronic ulcer penetrates through the mucosa into the muscle coat, causing fibrosis
- Scarring can produce pyloric stenosis
- Anterior duodenal ulcers tend to perforate
- Posterior duodenal ulcers tend to bleed - sometimes by eroding the gastroduodenal artery
- "Kissing ulcers" = both anterior and posterior ulcers present simultaneously
Endoscopic image - Duodenal ulcer:
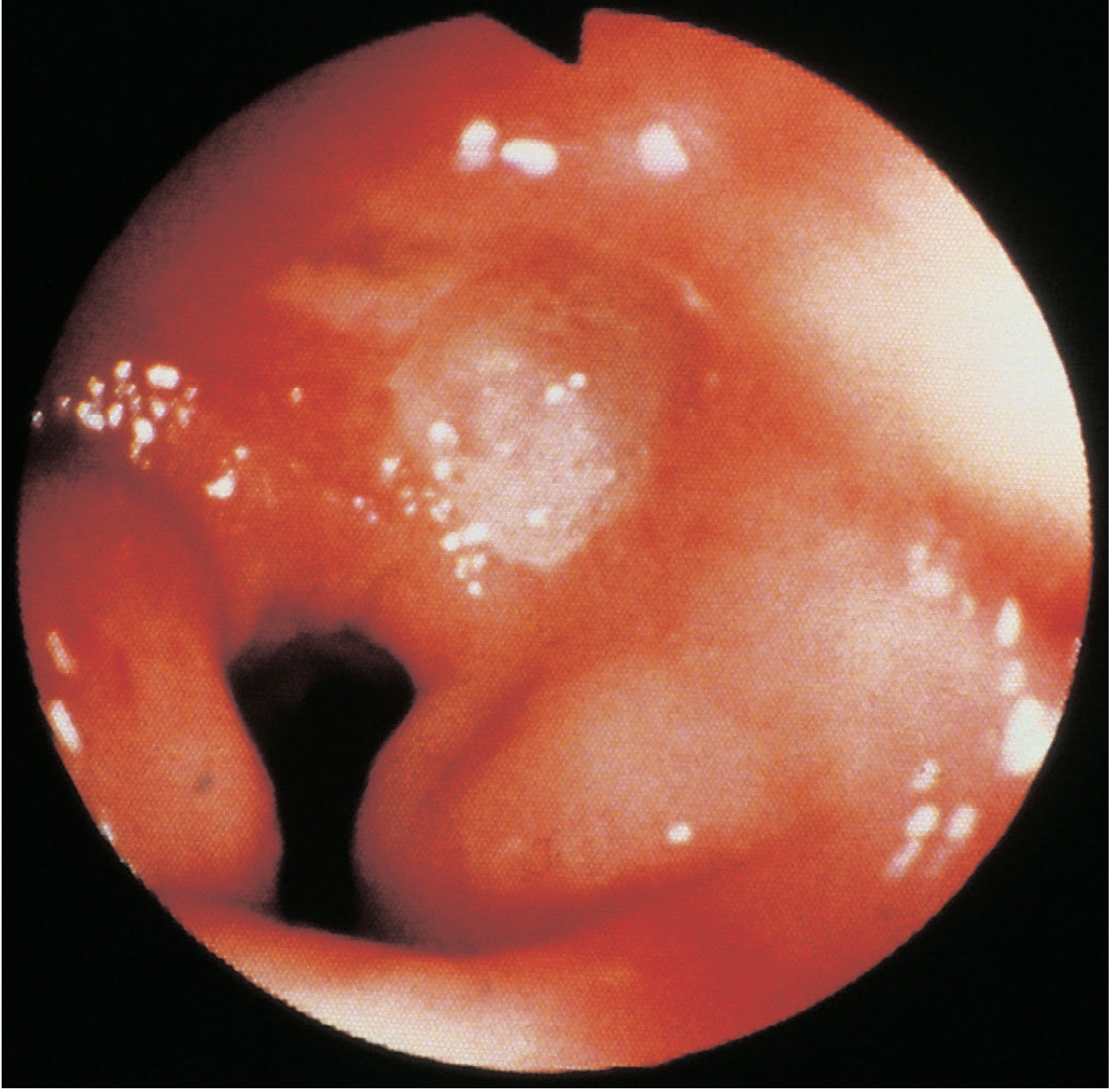
Figure: Duodenal ulcer at gastroduodenoscopy - Bailey and Love, p. 1179
Gastric Ulcers
- Tend to be larger than duodenal ulcers
- Most common on the lesser curve (especially incisura angularis)
- Fibrosis can cause an "hourglass" deformity of the stomach
- Chronic ulcers may erode posteriorly into the pancreas, splenic artery, or rarely the transverse colon
- Important: Unlike duodenal ulcers, gastric ulcers carry a risk of malignancy - every gastric ulcer must be regarded as potentially malignant until proven otherwise with multiple biopsies (up to 10)
- PPIs can heal ulceration associated with gastric cancer but do not treat the malignancy
Endoscopic image - Benign gastric ulcer at the incisura:
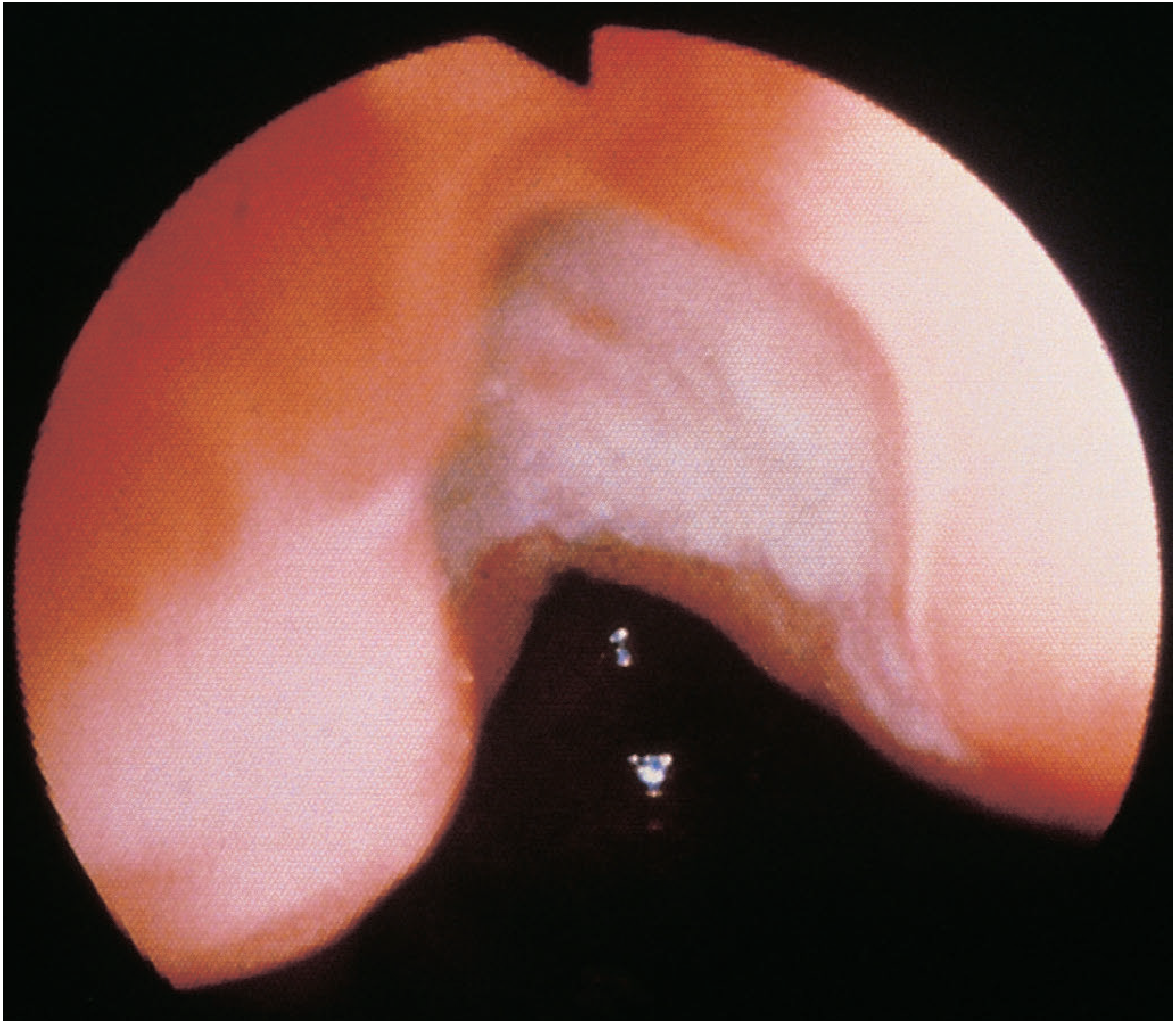
Figure: Benign gastric ulcer at incisura angularis - Bailey and Love, p. 1180
Histopathology
- Ulcer base is covered with granulation tissue
- Evidence of endarteritis obliterans may be present
- Healing ulcers show epithelial downgrowth that can be misinterpreted as invasion - careful pathological interpretation is needed
Clinical Features
Gastric and duodenal ulcer symptoms cannot be reliably distinguished from each other on clinical grounds alone.
Symptoms
- Epigastric pain - gnawing in character, sometimes radiating to the back; classically intermittent with symptom-free periods
- Eating may relieve discomfort (especially duodenal ulcers)
- Periodicity - symptoms disappear for weeks or months, then return; may correspond to spontaneous healing and re-ulceration
- Vomiting - not prominent unless pyloric stenosis has developed
- Weight change - weight loss common with gastric ulcers; sometimes weight gain
- Bleeding - chronic bleeding may present with microcytic (iron-deficiency) anemia; acute bleeding presents with hematemesis and/or melena
Clinical Examination
- Epigastric tenderness on palpation
- Otherwise unremarkable unless complications (e.g., gastric outlet obstruction) have developed
Investigations / Diagnosis
Gastroduodenoscopy (Upper GI Endoscopy)
- Investigation of choice
- In the stomach: all abnormal lesions must be biopsied; multiple biopsies (up to 10) from a suspected benign gastric ulcer are essential to exclude malignancy
- Antral biopsies + CLO (Campylobacter-like organism) test for H. pylori
- Full inspection including incisura, lesser curve, pylorus, and duodenum
Testing for H. pylori
| Test | Notes |
|---|---|
| Urea breath test | Non-invasive, good for diagnosis and confirming eradication |
| Stool antigen test | Useful non-invasive option |
| Rapid urease (CLO) test | Done at endoscopy on antral biopsy |
| Serology | Detects past or current infection; cannot confirm eradication |
| Histology | Gold standard - from biopsy specimen |
Complications
The four major complications of PUD are:
- Hemorrhage - Most common complication; bleeding peptic ulcer accounts for the majority of upper GI bleeds; posterior duodenal ulcers can erode the gastroduodenal artery
- Perforation - Anterior duodenal ulcers most commonly perforate; presents with sudden severe abdominal pain and peritonitis; management is primarily surgical
- Penetration - Ulcer erodes into adjacent organ (pancreas, splenic artery, transverse colon) without free perforation
- Gastric outlet obstruction (pyloric stenosis) - From fibrosis and scarring; presents with vomiting, especially of undigested food
The Rockall score is used to stratify rebleeding and mortality risk in upper GI bleeding (scores 0-8+, with score ≥8 carrying >41% mortality). - Sleisenger and Fordtran's GI and Liver Disease
Treatment
Medical Treatment (Mainstay)
The vast majority of uncomplicated peptic ulcers are treated medically. Elective surgery for uncomplicated PUD is now very rarely performed.
Step 1 - Acid suppression:
- PPIs (e.g., omeprazole, lansoprazole) are the most effective agents - can render a patient achlorhydric
- H2-receptor antagonists (e.g., ranitidine) were historically used; superseded by PPIs but still have a role
- Lifestyle modification: cessation of smoking (reduces relapse), avoid NSAIDs if possible
Step 2 - H. pylori eradication (when infection is present):
| Scenario | Recommended Regimen |
|---|---|
| No penicillin allergy, no macrolide exposure, local clarithromycin resistance <15% | Clarithromycin triple therapy: PPI + clarithromycin + amoxicillin x 14 days |
| Risk factors for macrolide resistance (prior macrolide use, resistance >15%) | Bismuth quadruple therapy: PPI + bismuth + tetracycline + metronidazole x 10-14 days |
| Penicillin allergy, no prior macrolide exposure | Bismuth quadruple therapy OR PPI + clarithromycin + metronidazole |
| Penicillin allergy + macrolide resistance risk | Bismuth quadruple therapy |
- Quadruple therapy achieves >90% eradication rates
- Clarithromycin worldwide resistance ranges from 20-35% - local resistance data should guide therapy choice
- After treatment, confirm eradication with urea breath test or stool antigen test
Source: ACG Clinical Guideline 2017 (Chey et al.) as cited in Sabiston Textbook of Surgery
NSAID-Associated Ulcers
- Discontinue NSAID if possible
- If NSAID must be continued: co-prescribe a PPI; consider switching to a selective COX-2 inhibitor
- Test and treat for H. pylori (eradication reduces ulcer recurrence even in NSAID users)
Surgical Treatment
- Reserved for complications: perforation (surgical repair/omental patch), uncontrolled hemorrhage (endoscopic failure), gastric outlet obstruction, and suspected malignancy
- Historically included vagotomy and antrectomy to reduce acid - rarely done now
Recent Evidence
Recent meta-analyses (2024-2025) show that vonoprazan (a potassium-competitive acid blocker, P-CAB) is at least as effective as PPIs for healing gastric and duodenal ulcers and may offer advantages in H. pylori eradication regimens - see Vonoprazan vs. PPIs for peptic ulcer (Dig Dis Sci 2024, PMID 39294424) and a network meta-analysis comparing P-CABs and PPIs (Clin Transl Gastroenterol 2024, PMID 39412166). These newer agents may become more prominent in guidelines.
Summary: Key Points
- PUD results from failure of mucosal defenses against acid/pepsin, most often driven by H. pylori or NSAIDs
- Duodenal ulcers are more common; gastric ulcers require biopsy to exclude malignancy
- Classic symptom: intermittent gnawing epigastric pain; symptoms of both types are clinically indistinguishable
- Complications: hemorrhage, perforation, penetration, obstruction
- Treatment: PPI + H. pylori eradication (triple or bismuth quadruple therapy depending on resistance risk)
- Surgery is now reserved for complications; elective surgical treatment is rare
Sources: Robbins & Kumar Basic Pathology | Bailey and Love's Short Practice of Surgery 28th ed. | Sabiston Textbook of Surgery | Rosen's Emergency Medicine | Sleisenger & Fordtran's GI and Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.