









+16 more
Answers the question laq long type easy very detailed manner using flow chart heading and points where ever required source parks text book and other authentic book
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
THEORIES OF DISEASE CAUSATION, EPIDEMIOLOGICAL TRIAD, WEB OF CAUSATION & NATURAL HISTORY OF DISEASE
Source: Park's Textbook of Preventive and Social Medicine (Park's PSM)
OVERVIEW FLOWCHART - EVOLUTION OF DISEASE CAUSATION CONCEPTS
ANCIENT BELIEFS (Supernatural / Humors / Miasma)
↓
GERM THEORY OF DISEASE (Pasteur, Koch - 1860-1880s)
(Single Agent → Man → Disease)
↓
LIMITATIONS RECOGNIZED
(Not all exposed persons develop disease)
↓
EPIDEMIOLOGICAL TRIAD (Agent + Host + Environment)
↓
BIOMEDICAL MODEL
↓
WEB OF CAUSATION (MacMahon & Pugh - multifactorial)
↓
BEINGS MODEL / MULTIFACTORIAL AETIOLOGY (Modern Concept)
SECTION 1: PRIMITIVE & EARLY THEORIES OF DISEASE CAUSATION
(Park's PSM, p. 43)
For a long time, humans groped in darkness about disease causation. Several theories evolved:
| Theory | Era | Core Concept |
|---|---|---|
| Supernatural Theory | Ancient | Disease is punishment from God / evil spirits |
| Theory of Humors | Greeks & Indians | Imbalance of 4 humors (blood, phlegm, yellow bile, black bile) |
| Theory of Contagion | Middle Ages | Disease spreads by direct contact |
| Miasmatic Theory | Pre-1850 | Disease caused by noxious air / bad vapors ("miasma") |
| Theory of Spontaneous Generation | Pre-Pasteur | Living organisms arise from non-living matter |
SECTION 2: GERM THEORY OF DISEASE
(Park's PSM, p. 43 & p. 415)
Key Milestones:
- 1860 - Louis Pasteur (French bacteriologist, 1822-1895) demonstrated bacteria in air; disproved spontaneous generation
- 1873 - Pasteur advanced the "Germ Theory of Disease"
- 1877 - Robert Koch (1843-1910) proved anthrax was caused by a bacterium
- This was the "Golden Age of Bacteriology" - microbes discovered in rapid succession:
- Gonococcus (1847)
- Typhoid bacillus, Pneumococcus (1880)
- Tubercle bacillus (1882)
- Cholera vibrio (1883)
- Diphtheria bacillus (1884)
Disease Model:
Disease Agent -----→ Man -----→ Disease
(Germ) (Host)
Limitations of Germ Theory:
- One-to-one relationship is an over-simplification
- Not everyone exposed to TB develops tuberculosis
- Not everyone exposed to streptococci develops rheumatic fever
- Cannot explain chronic diseases (where agent is often unknown)
- Cannot account for host resistance, nutrition, immunity, environment
- Conclusion: Modern medicine has moved away from strict adherence to the germ theory
SECTION 3: EPIDEMIOLOGICAL TRIAD
(Park's PSM, p. 44)
Definition:
A broader concept of disease causation that synthesizes the three basic factors: Agent, Host, and Environment.
Diagram - The Epidemiological Triad:
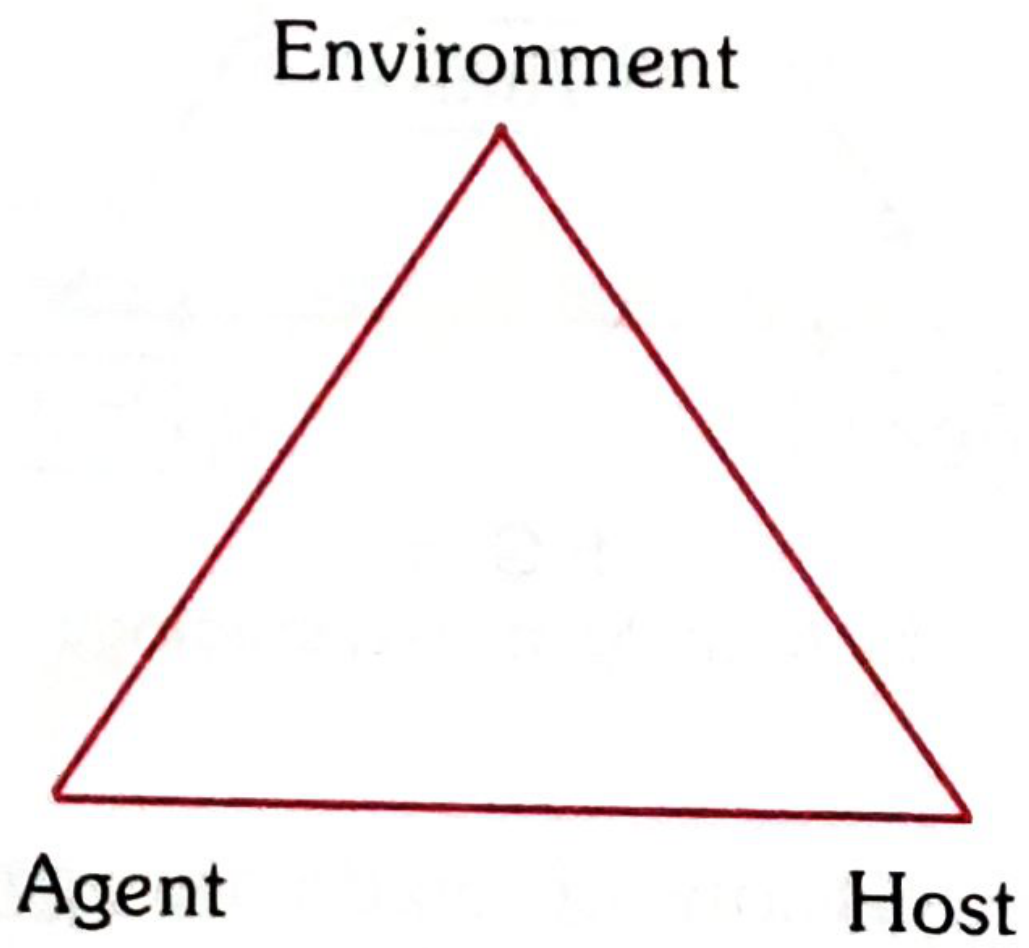
Fig. 4 - Epidemiological Triad (Park's Textbook of Preventive and Social Medicine)
The Triangle of Epidemiology:
"The agent is the cause of disease; the host is an organism that harbours the disease; the environment is those surroundings and conditions external to the human that cause or allow disease transmission; and time accounts for incubation periods, life expectancy of the host or pathogen, and duration of the illness." - Park's PSM
A. AGENT FACTORS
Definition: A substance, living or non-living, or a force, tangible or intangible, the excessive presence or relative lack of which may initiate or perpetuate a disease process.
Classification of Disease Agents:
DISEASE AGENTS
|
┌────────┬────────┬────────┬────────┬────────┬────────┐
↓ ↓ ↓ ↓ ↓ ↓ ↓
Biological Nutrient Physical Chemical Mechanical Social Absence/
Agents Agents Agents Agents Agents Agents Excess of
factors
1. Biological Agents - Viruses, Rickettsiae, Fungi, Bacteria, Protozoa, Metazoa
- Key properties:
- Infectivity - Ability to invade and multiply in host
- Pathogenicity - Ability to induce clinically apparent illness
- Virulence - Proportion of clinical cases with severe manifestations
2. Nutrient Agents - Proteins, fats, carbohydrates, vitamins, minerals, water
- Excess OR deficiency causes disease
- Examples: PEM (Protein Energy Malnutrition), anaemia, goitre, obesity
3. Physical Agents - Excessive heat, cold, humidity, pressure, radiation, electricity, sound
4. Chemical Agents
- Endogenous: Produced inside body - urea (uraemia), bilirubin (jaundice), ketones, uric acid (gout)
- Exogenous: Allergens, metals, fumes, dust, gases, insecticides - acquired by inhalation, ingestion, or inoculation
5. Mechanical Agents - Chronic friction, crushing, tearing, sprains, dislocations
6. Absence/Insufficiency/Excess of a Factor Necessary for Health
- Chemical: hormones (insulin, oestrogens, enzymes)
- Nutrient factors
- Lack of structure (e.g., thymus)
- Chromosomal factors (mongolism, Turner's syndrome)
- Immunological factors (agammaglobulinaemia)
7. Social Agents - Poverty, smoking, alcohol/drug abuse, unhealthy lifestyles, social isolation, maternal deprivation
B. HOST FACTORS (Intrinsic)
"In epidemiological terminology, the human host is referred to as 'soil' and the disease agent as 'seed'." - Park's PSM
Classification of Host Factors:
| Category | Examples |
|---|---|
| Demographic | Age, sex, ethnicity |
| Biological | Genetic factors, blood groups, enzymes, cholesterol levels, immunological factors, physiological function |
| Social & Economic | Socio-economic status, education, occupation, stress, marital status, housing |
| Lifestyle | Personality traits, living habits, nutrition, physical exercise, alcohol, drugs, smoking |
C. ENVIRONMENTAL FACTORS (Extrinsic)
Three categories:
1. Physical Environment - Air, water, soil, climate, geography, noise, radiation
2. Biological Environment - Reservoirs of infection, vectors (mosquitoes, flies), food, flora/fauna
3. Social Environment - Culture, customs, religion, socioeconomic status, healthcare systems, population density
Dynamic Interaction of the Triad:
ENVIRONMENT
(Extrinsic factors)
↑
|
AGENT ←---→ HOST
(Disease (Intrinsic
cause) factors)
↓
DISEASE
- If AGENT is strong + HOST is susceptible + ENVIRONMENT is favourable → DISEASE occurs
- If HOST immunity is high → No disease (even with agent present)
- If ENVIRONMENT is unfavourable for agent → Disease does not spread
SECTION 4: WEB OF CAUSATION
(Park's PSM, p. 45 - MacMahon & Pugh, "Epidemiologic Principles and Methods")
Definition:
A model of disease causation that considers all predisposing factors of any type and their complex interrelationship with each other.
Key Features:
- Proposed by Brian MacMahon and Thomas Pugh in their book "Epidemiologic Principles and Methods"
- Ideally suited for chronic disease where the disease agent is often NOT known
- Disease is an outcome of interaction of multiple factors
- Does NOT imply all causes must be removed to control disease
- Sometimes elimination of just one important link may be sufficient to control disease
- Relative importance of factors expressed as "relative risk"
Classic Example - Web of Causation for Myocardial Infarction:
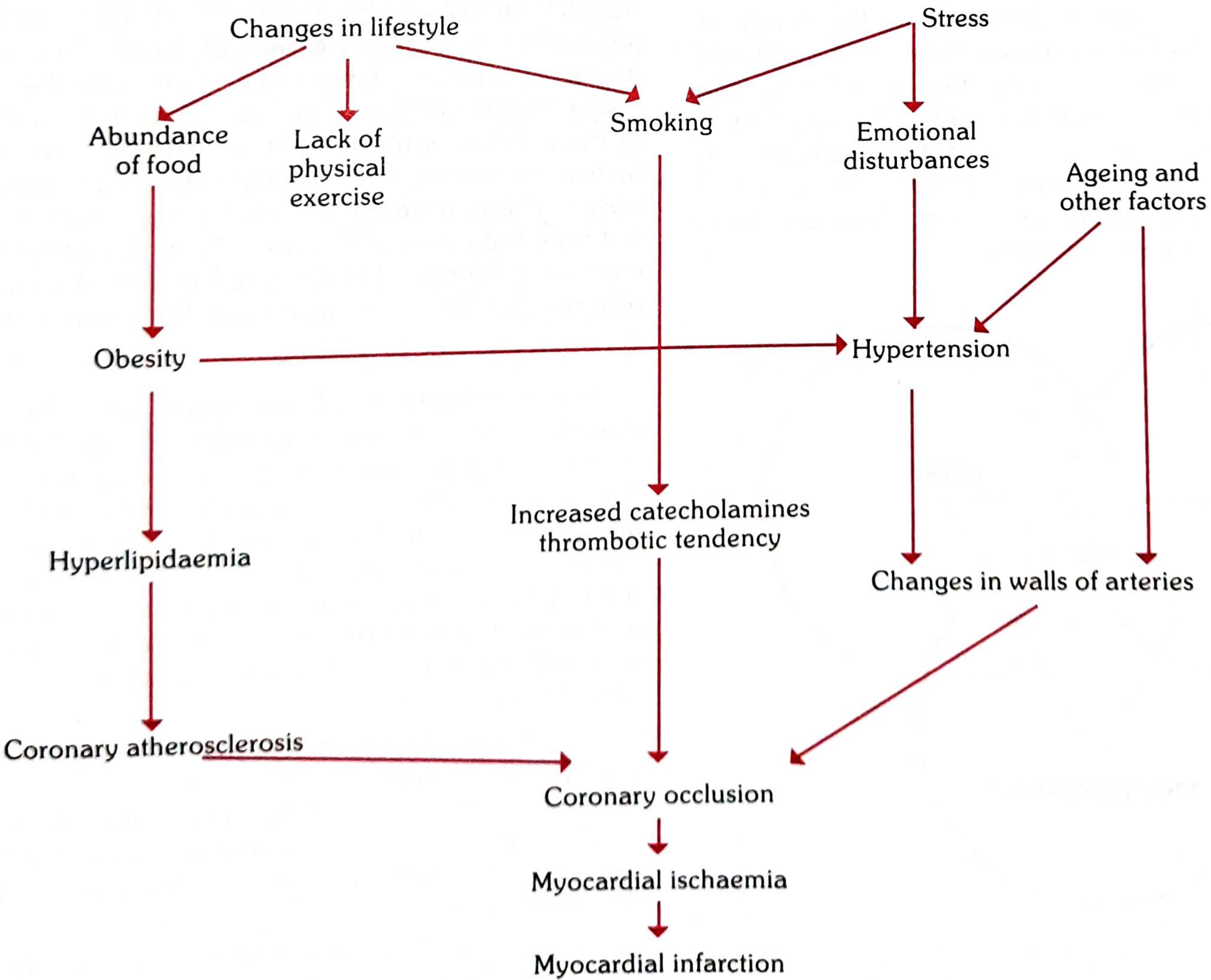
Fig. 7 - Web of Causation for Myocardial Infarction (Park's PSM)
Reading the Web:
Changes in Lifestyle + Stress
↓ ↓
Abundance of food Emotional disturbances
Lack of exercise Smoking
↓ ↓
Obesity --------→ Hypertension ←-- Ageing
↓ ↓
Hyperlipidaemia Changes in artery walls
↓ ↓
Coronary atherosclerosis + Increased catecholamines
↓
Coronary Occlusion
↓
Myocardial Ischaemia
↓
MYOCARDIAL INFARCTION
Significance of Web of Causation:
- Provides a model showing a variety of possible interventions
- Breaking even ONE link in the web can prevent disease
- Forms the basis of multifactorial causation in modern epidemiology
- Explains why chronic diseases cannot be attributed to a single agent
SECTION 5: BEINGS MODEL (Multifactorial Aetiology)
(Based on community medicine syllabus - standard textbook concept)
What is the BEINGS Model?
BEINGS is a mnemonic that classifies the multiple factors contributing to disease causation in the context of multifactorial aetiology.
BEINGS = Biological, Environmental, Immunological, Nutritional, Genetic, Social/Services
| Letter | Factor | Examples |
|---|---|---|
| B | Biological factors | Age, sex, species, developmental stage |
| E | Environmental factors | Physical, chemical, biological environment |
| I | Immunological factors | Immunity (natural/acquired), herd immunity |
| N | Nutritional factors | Malnutrition, vitamin deficiency, over-nutrition |
| G | Genetic factors | Hereditary diseases, chromosomal disorders |
| S | Social factors / Services | Socioeconomic status, health services, lifestyle |
BEINGS Model - Flowchart:
DISEASE CAUSATION
↑
┌──────┬──────┬──────┼──────┬──────┬──────┐
↓ ↓ ↓ ↓ ↓ ↓ ↓
Bio- Envi- Immun- Nutri- Genet- Social/
logical ronm'l olog'l ional ic Services
factors factors factors factors factors factors
Types of Causal Factors in Disease:
| Type of Factor | Definition | Example |
|---|---|---|
| Predisposing | Creates susceptibility | Malnutrition predisposes to TB |
| Enabling | Facilitates disease occurrence | Poor housing enables TB spread |
| Precipitating | Triggers onset of disease | Exposure to TB bacillus |
| Reinforcing | Perpetuates disease | Repeated exposure, poverty |
| Risk factors | Associated with disease (not necessarily causal) | Smoking and lung cancer |
SECTION 6: NATURAL HISTORY OF DISEASE
(Park's PSM, p. 46 - adapted from Leavell & Clark)
Definition:
"The way in which a disease evolves over time from the earliest stage of its prepathogenesis phase to its termination as recovery, disability or death, in the absence of treatment or prevention." - Park's PSM
Diagram - Natural History of Disease (Leavell & Clark Model):
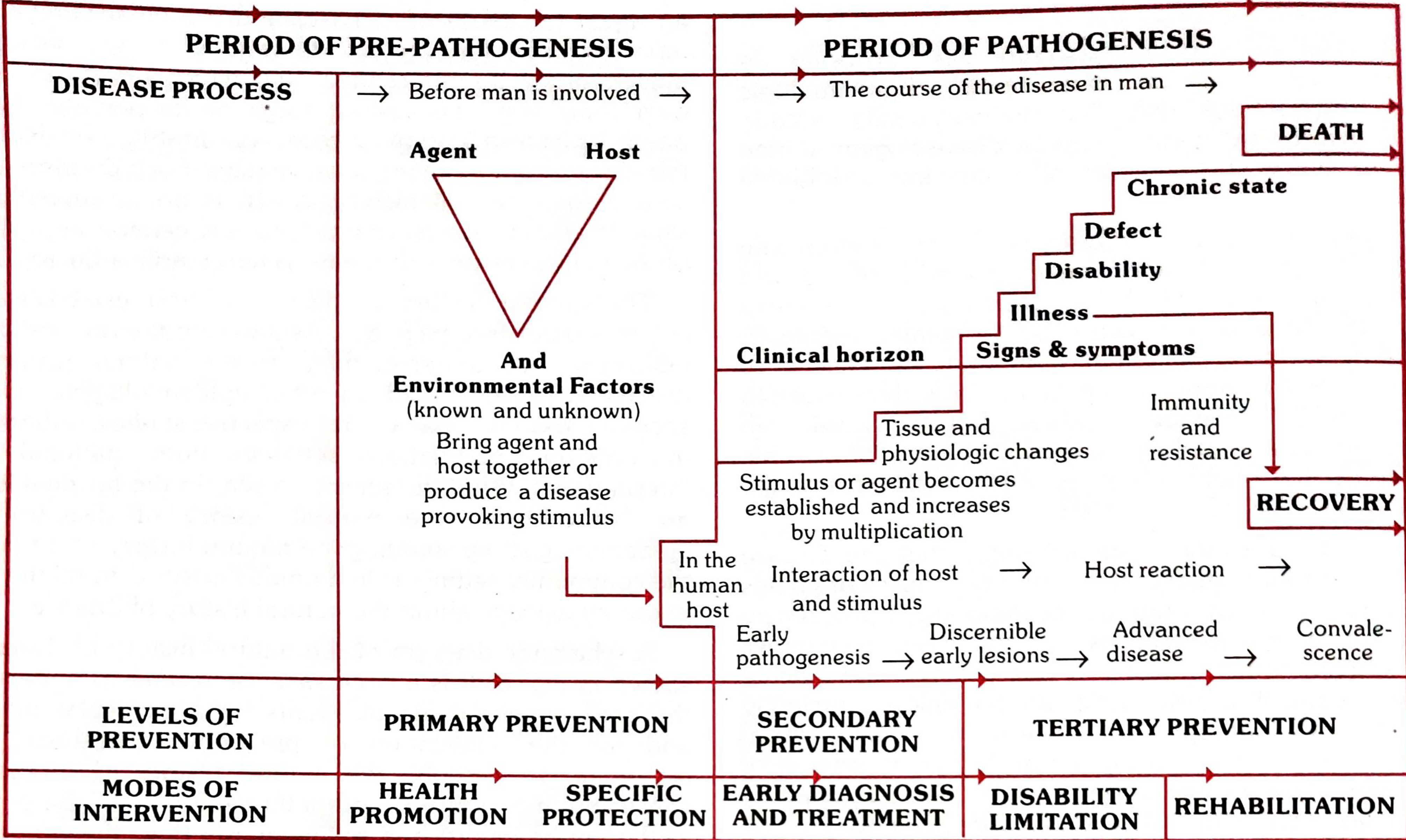
Fig. 8 - Natural History of Disease with Levels of Prevention (Leavell & Clark / Park's PSM)
TWO PHASES OF NATURAL HISTORY OF DISEASE:
NATURAL HISTORY OF DISEASE
|
┌─────┴─────┐
↓ ↓
PHASE 1: PHASE 2:
Pre- Pathogenesis
pathogenesis Phase
Phase (Process in Man)
(Process in
Environment)
PHASE 1: PREPATHOGENESIS PHASE
Definition: The period preliminary to the onset of disease in man. The disease agent has not yet entered man, but factors favouring its interaction with the human host are already existing in the environment.
- Also called: "Man in the midst of disease" or "Man exposed to risk of disease"
- Potentially, all humans are in the prepathogenesis phase of many diseases (both communicable and non-communicable)
- The Epidemiological Triad (Agent + Host + Environment) operates during this phase
Key Point: Mere presence of agent, host and favourable environmental factors is NOT sufficient to start disease. What is required is an INTERACTION of these three factors.
PHASE 2: PATHOGENESIS PHASE
Definition: Begins with the entry of the disease agent into the susceptible human host.
Sub-phases:
Entry of Agent into Host
↓
Early Pathogenesis
(Agent multiplies, tissue/physiological changes begin)
↓
Discernible Early Lesions
(Pathological changes below "clinical horizon")
↓
CLINICAL HORIZON
(Signs and symptoms appear)
↓
Advanced Disease / Illness
↓
Convalescence
↓
┌────┴────┐
↓ ↓
RECOVERY DEATH / DISABILITY / CHRONIC STATE
Clinical Horizon:
- The threshold below which disease is not detectable clinically
- Above this horizon = signs and symptoms appear
- In chronic diseases (e.g., hypertension, cancer), the presymptomatic phase is silent and prolonged
Host's Reaction to Infection - Not Predictable:
- May be clinical or subclinical
- May be typical or atypical
- Host may become a carrier (e.g., diphtheria, Hepatitis B)
SECTION 7: LEVELS OF PREVENTION (Based on Natural History)
(Leavell & Clark Model - as shown in Park's diagram)
The five levels of prevention are mapped to the natural history of disease:
| Phase | Level of Prevention | Mode of Intervention |
|---|---|---|
| Pre-pathogenesis | Primary Prevention | Health Promotion + Specific Protection |
| Early Pathogenesis | Secondary Prevention | Early Diagnosis and Treatment |
| Late Pathogenesis | Tertiary Prevention | Disability Limitation + Rehabilitation |
PRIMARY PREVENTION:
- Health Promotion - Health education, adequate nutrition, improved housing, regular exercise
- Specific Protection - Immunization, chemoprophylaxis, protection from carcinogens, use of protective equipment
SECONDARY PREVENTION:
- Early Diagnosis - Screening programs, case finding
- Prompt Treatment - Preventing complications, limiting disability
TERTIARY PREVENTION:
- Disability Limitation - Treatment to prevent further complications
- Rehabilitation - Physical, social, psychological rehabilitation to restore maximum function
SECTION 8: BIOMEDICAL MODEL vs SOCIAL MODEL (Comparison)
| Feature | Biomedical Model | Social (Multifactorial) Model |
|---|---|---|
| Cause | Single agent (germ) | Multiple interacting factors |
| Focus | Disease in the body | Disease in the community |
| Approach | Cure by eliminating pathogen | Prevention through social/environmental change |
| Applicable to | Infectious diseases | Both infectious and non-infectious |
| Limitations | Cannot explain chronic disease | Requires complex data |
QUICK SUMMARY MIND MAP
DISEASE CAUSATION
|
┌─────────────────┼─────────────────┐
↓ ↓ ↓
HISTORICAL MODERN NATURAL
THEORIES MODELS HISTORY
| | |
Supernatural Epidemiol. Pre-patho-
Humors Triad genesis
Miasma (AHE) phase
Germ Theory | |
Web of Pathogenesis
Causation phase
| |
BEINGS Levels of
Model Prevention
(1°, 2°, 3°)
KEY DEFINITIONS (For Viva/MCQ):
- Disease Agent - A substance, living or non-living, or force, the excessive presence or relative lack of which may initiate or perpetuate a disease process (Park's PSM)
- Host - "Soil" in which the disease "seed" grows; harbours the disease
- Epidemiological Triad - Agent + Host + Environment operating in combination to determine disease occurrence
- Web of Causation - Model showing complex interrelationship of all predisposing factors (MacMahon & Pugh)
- Natural History of Disease - Evolution of disease from prepathogenesis to recovery/death in absence of treatment
- Clinical Horizon - The threshold above which disease becomes clinically detectable
- Prepathogenesis Phase - Period before disease agent enters the host; "man exposed to risk"
- Pathogenesis Phase - Begins with entry of agent into susceptible host
Source: Park's Textbook of Preventive and Social Medicine (Park's PSM), Chapter on Epidemiology, pp. 43-47. Leavell HR & Clark EG - "Preventive Medicine for the Doctor in His Community" (McGraw-Hill). MacMahon B & Pugh TF - "Epidemiologic Principles and Methods."
Answers all remaining questions fromthe pictures I sent u which u did not answer in previous chat the same way
analyse_media
analyse_media
analyse_media
analyse_media
analyse_media
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Here are all the remaining LAQ answers from your syllabus notes, in detailed format with flowcharts, headings, and points - sourced from Park's Textbook of Preventive and Social Medicine and other authentic references.
SECTION A: FUNDAMENTAL CONCEPTS OF COMMUNITY MEDICINE & PUBLIC HEALTH
LAQ 1: DEFINE AND DIFFERENTIATE COMMUNITY MEDICINE, PREVENTIVE MEDICINE, SOCIAL MEDICINE AND PUBLIC HEALTH
Flowchart - Evolution of Terms:
PUBLIC HEALTH (1840s)
↓
PREVENTIVE MEDICINE (18th-19th century)
↓
SOCIAL MEDICINE (1940s - Virchow, Sand)
↓
COMMUNITY MEDICINE (1960s-70s - modern successor)
↓
All share common ground: Prevention of Disease + Promotion of Health
1. PREVENTIVE MEDICINE
Definition (Clark, 1953):
"Preventive medicine is the science and art of health, dealing with individuals, families and groups, is oriented towards the whole person, and is concerned with the promotion of health and the prevention of disease."
Key Features:
- Focuses on individuals and families
- Applied by the practicing physician in clinical settings
- Deals with primary, secondary and tertiary prevention
- Closely linked with clinical medicine
- Applied to specific individuals (not populations)
Three Levels of Preventive Medicine:
Primary Prevention → Preventing disease before it occurs
Secondary Prevention → Early detection and treatment
Tertiary Prevention → Rehabilitation, limiting disability
2. SOCIAL MEDICINE
Definition (Guérin, 1848):
"Social medicine investigates conditions of life and work that affect the state of health and endeavours to ensure the citizen good means of maintaining health or recovering it when it is impaired."
Key Features:
- Studies the relationship between health and social conditions
- Focuses on the social determinants of disease (poverty, unemployment, housing)
- Introduced by Rudolf Virchow: "Medicine is nothing but politics on a large scale"
- Concerned with the social causes of ill-health
3. COMMUNITY MEDICINE
Definition (Faculty of Community Medicine, Royal College of Physicians):
"That speciality which deals with populations...and comprises those doctors who try to measure the needs of the population, both sick and well, who plan and administer services to meet those needs, and those who are engaged in research and teaching in the field." (Park's PSM, p. 23)
Key Features:
- Deals with populations (not just individuals)
- Successor of Public Health, Preventive and Social Medicine
- Studies health needs, plans services, conducts research
- Uses epidemiology as its primary tool
- Applicable to both sick and well populations
4. PUBLIC HEALTH
Definition (Winslow, 1920 / WHO Expert Committee):
"The science and art of preventing disease, prolonging life, and promoting health and efficiency through organized community efforts for the sanitation of the environment, the control of communicable infections, the education of the individual in personal hygiene, the organization of medical and nursing services for early diagnosis and preventive treatment of disease, and the development of social machinery to ensure for every individual a standard of living adequate for the maintenance of health." (Park's PSM, p. 1)
Key Features:
- Arose from the need to protect "the public" from communicable diseases (~1840)
- Organized, community-based effort
- Involves sanitation, immunization, health education, disease control
- A social institution created and maintained by society
- Modern public health also includes organization of medical care
COMPARISON TABLE: Preventive Medicine vs Public Health vs Community Medicine
| Feature | Preventive Medicine | Public Health | Community Medicine |
|---|---|---|---|
| Focus | Individual/Family | Community/Society | Population |
| Setting | Clinical (hospital/clinic) | Community/Environment | Community + academic |
| Tools | Clinical skills | Sanitation, legislation | Epidemiology, statistics |
| Scope | Disease prevention (3 levels) | Organized community effort | Health needs planning |
| Approach | Doctor-patient | Govt/Society | Research + service |
| Era | 18th century | 19th century | 20th century |
LAQ 2: FUNCTIONS OF PUBLIC HEALTH
(Park's PSM)
Core Functions (WHO / Institute of Medicine):
FUNCTIONS OF PUBLIC HEALTH
|
┌──────────────┼──────────────┐
↓ ↓ ↓
ASSESSMENT POLICY ASSURANCE
(Monitoring) DEVELOPMENT (Service Delivery)
Detailed Functions:
1. Assessment / Surveillance
- Monitor health status of communities
- Investigate and diagnose health problems and hazards
- Collect, manage, analyze health data (vital statistics)
2. Policy Development
- Inform, educate and empower people about health issues
- Mobilize community partnerships
- Develop policies and plans that support health efforts
3. Assurance
- Link people to needed health services
- Ensure a competent public health workforce
- Evaluate effectiveness, accessibility of health services
- Research new insights and innovative solutions
4. Specific Functions (Winslow's Framework):
- Sanitation of the environment
- Control of communicable infections
- Education of individuals in personal hygiene
- Organization of medical/nursing services for early diagnosis
- Development of social machinery for adequate standard of living
- Organize medical care as a means of protecting health
LAQ 3: HISTORY OF PUBLIC HEALTH - GLOBALLY AND IN INDIA
GLOBAL HISTORY:
Flowchart - Phases of Public Health:
PHASE 1: Disease Era / Miasmatic Period (before 1850)
Sanitary reforms; John Snow (Cholera, 1854)
↓
PHASE 2: Bacteriological / Germ Theory Era (1850-1900)
Pasteur, Koch; vaccines, antiseptics
↓
PHASE 3: Health Promotion Era (1900-1950)
Maternal & child health, nutrition, housing
↓
PHASE 4: Social Engineering Era (1950-1980)
WHO (1948), Health For All, Primary Health Care
↓
PHASE 5: Health Promotion & Sustainable Development (1980-present)
Ottawa Charter (1986), MDGs, SDGs
Key Milestones Globally:
- 1796 - Jenner: Smallpox vaccination
- 1842 - Chadwick Report (sanitary conditions of labouring population)
- 1848 - Public Health Act, England
- 1854 - John Snow: Cholera epidemic map (Broad Street pump)
- 1860 - Florence Nightingale: Nursing and hospital hygiene
- 1860-1890 - Pasteur, Koch: Golden Age of Bacteriology
- 1948 - WHO established; WHO definition of health
- 1978 - Alma-Ata Declaration: "Health for All by 2000", Primary Health Care
- 1986 - Ottawa Charter: Health Promotion
PUBLIC HEALTH IN INDIA:
Timeline:
PRE-INDEPENDENCE:
1859 - First Sanitary Commissioner appointed
1864 - Sanitary Commission established
1897 - Epidemic Diseases Act
1912 - Indian Red Cross Society
POST-INDEPENDENCE:
1946 - Bhore Committee Report (comprehensive health services plan)
1952 - First Five Year Plan: Community Development Programme
1952 - National Family Planning Programme (first in the world)
1977 - Community Health Workers (CHW) programme
1978 - Alma-Ata Declaration endorsed
1983 - National Health Policy (NHP)
2002 - NHP 2002 (focus on decentralization)
2005 - NRHM (National Rural Health Mission)
2013 - NUHM (National Urban Health Mission)
2017 - NHP 2017
2018 - Ayushman Bharat: Health & Wellness Centres + PM-JAY
SECTION B: CONCEPT OF HEALTH
LAQ 4: DEFINE HEALTH. DISCUSS THE DIMENSIONS AND BIOMEDICAL MODEL OF HEALTH
Definition of Health (WHO, 1948):
"Health is a state of complete physical, mental and social well-being and not merely an absence of disease or infirmity." (Park's PSM, p. 19)
- Amplified later to include: ability to lead a "socially and economically productive life"
- The WHO definition is broad, positive, and sets a standard of "positive health"
- Criticized as being too ideal / not easily measurable
Operational Definition (WHO Study Group):
- Broad sense: "A condition or quality of the human organism expressing the adequate functioning of the organism in given conditions, genetic or environmental"
- Narrow sense (measurable): No obvious evidence of disease + person functioning normally within normal limits for age, sex, community, geography
DIMENSIONS OF HEALTH:
(Park's PSM, p. 19-21)
DIMENSIONS OF HEALTH
|
┌──────┬───────┬───────┬────────┬─────────┬──────────┐
↓ ↓ ↓ ↓ ↓ ↓ ↓
Physical Mental Social Spiritual Emotional Vocational Political
1. Physical Dimension
- "Perfect functioning" of the body
- Every cell and organ functioning at optimum capacity
- Signs: good complexion, clean skin, bright eyes, normal pulse/BP, normal weight
- Evaluated by: self-assessment, inquiry into symptoms, inquiry into medications, laboratory tests
2. Mental Dimension
- Ability to think clearly and coherently
- Absence of mental disorder
- Not just absence of mental illness but positive mental well-being
- Includes: ability to respond to challenges, manage stress, maintain self-esteem
3. Social Dimension
- Ability to make and maintain relationships
- Social harmony and adjustment
- Ability to participate in social activities
- Quantified by: social adjustment, social functioning scales
4. Spiritual Dimension
- Relates to personal beliefs, values, morals
- Provides a sense of purpose and direction
- Not necessarily linked to religion; involves living according to one's values
- Important especially in palliative care
5. Emotional Dimension
- Ability to express emotions appropriately
- Emotional maturity and control
- Ability to handle stress and adversity
6. Vocational Dimension
- Ability to engage in productive work
- Occupational health and satisfaction
- "Health is the essence of productive life" (WHO philosophy)
BIOMEDICAL MODEL OF HEALTH:
Definition: Health = absence of disease; disease = due to specific biological causative agents
Key Features:
- Based on the Germ Theory of Disease
- Focuses on pathological, biochemical and physiological changes
- Treats disease as a deviation from normal biological function
- Single cause → single disease model
- Ignores social, psychological, environmental factors
Disease Model:
Disease Agent → Biological Defect → Disease → Treatment → Cure
Limitations of Biomedical Model:
- Cannot explain chronic non-communicable diseases
- Ignores social determinants of health
- Ignores psychological factors (mind-body connection)
- Does not explain why some exposed individuals do not get disease
- Leads to over-medicalization
- Not applicable to health promotion
COMPARISON OF MODELS OF HEALTH:
| Model | Key Concept | Limitation |
|---|---|---|
| Biomedical | Absence of disease | Too narrow; ignores social factors |
| Ecological | Balance between man and environment | Incomplete without host factors |
| Psychological | Mind-body interaction | Hard to measure |
| Social | Health as social well-being | Too broad |
| Holistic | Complete physical, mental, social well-being | Difficult to operationalize |
SECTION C: NUTRITION FOR COMMUNITY
LAQ 5: DISCUSS THE TYPES OF MALNUTRITION. METHODS TO MEASURE AND PREVENTION/CONTROL
Definition of Malnutrition:
"Malnutrition is a pathological state resulting from a relative or absolute deficiency or excess of one or more essential nutrients." - WHO / Park's PSM
Flowchart - Classification of Malnutrition:
MALNUTRITION
|
┌─────────────┴─────────────┐
↓ ↓
UNDERNUTRITION OVERNUTRITION
(Deficiency) (Excess)
| |
┌────────┴────────┐ Obesity, Metabolic
↓ ↓ Syndrome, CVD
Protein Energy Micronutrient
Malnutrition Deficiency
(PEM) |
┌────┴────┐
↓ ↓
Vitamins Minerals
(A, D, B1, (Iron, Iodine,
B2, C, etc) Calcium, Zinc)
TYPES OF MALNUTRITION:
A. Protein Energy Malnutrition (PEM):
| Feature | Kwashiorkor | Marasmus |
|---|---|---|
| Cause | Protein deficiency with adequate calories | Total calorie deficiency |
| Age | 1-3 years | <1 year |
| Growth | Some height preserved | Severe stunting |
| Muscle | Wasted with oedema | Severely wasted |
| Oedema | Present (pitting) | Absent |
| Appearance | "Pot belly", moon face | "Skin and bones", old man look |
| Hair | Dyspigmented, sparse | May be sparse |
| Skin | Dermatosis (flaky paint) | Wrinkled, loose |
| Appetite | Poor | Ravenous |
B. Micronutrient Deficiencies:
| Deficiency | Disease | Key Features |
|---|---|---|
| Vit A | Xerophthalmia | Night blindness, Bitot's spots, corneal ulcer |
| Vit D | Rickets (child) / Osteomalacia (adult) | Bone deformity, bow legs |
| Vit B1 (Thiamine) | Beriberi | Wet (cardiac) / Dry (neurological) |
| Vit B2 (Riboflavin) | Ariboflavinosis | Angular stomatitis, glossitis |
| Niacin (B3) | Pellagra | 4 Ds: Dermatitis, Diarrhea, Dementia, Death |
| Vit C | Scurvy | Bleeding gums, perifollicular haemorrhage |
| Iron | Iron deficiency anaemia | Fatigue, pallor, koilonychia |
| Iodine | Goitre, Cretinism | Thyroid enlargement, intellectual disability |
| Zinc | Growth retardation, immune deficiency | Poor wound healing |
C. Overnutrition:
- Obesity (BMI >30), metabolic syndrome, type 2 DM, CVD, NAFLD
METHODS TO MEASURE MALNUTRITION (Nutritional Assessment):
NUTRITIONAL ASSESSMENT
|
┌────────┼────────┬─────────┐
↓ ↓ ↓ ↓
Anthro- Clinical Dietary Biochem-
pometric Signs Methods ical/Lab
1. Anthropometric Methods:
| Measurement | Normal Values / Significance |
|---|---|
| Weight-for-Age | Underweight (WHO Z-score <-2 SD) |
| Height-for-Age | Stunting (chronic malnutrition) |
| Weight-for-Height | Wasting (acute malnutrition) |
| BMI (Body Mass Index) | Wt (kg) / Ht (m²); <18.5 = underweight |
| Mid-upper Arm Circumference (MUAC) | <12.5 cm in children = severe malnutrition |
| Head circumference | Microcephaly |
| Skin fold thickness | Body fat assessment |
Key Terms:
- Stunting = Low Height-for-Age (chronic, long-standing malnutrition)
- Wasting = Low Weight-for-Height (acute, recent malnutrition)
- Underweight = Low Weight-for-Age (composite indicator)
2. Clinical Signs:
- Hair: flag sign, easily pluckable, dyspigmentation
- Skin: dermatosis, oedema, pallor
- Eyes: Bitot's spots, corneal ulceration
- Mouth: angular stomatitis, glossitis, bleeding gums
- Bones: rickets, bowing of legs
- Abdomen: hepatomegaly, pot belly
3. Dietary Assessment Methods:
| Method | Description |
|---|---|
| 24-hour Recall | Patient recalls all food consumed in past 24 hours; quick, cheap, but recall bias |
| Food Frequency Questionnaire | Frequency of consuming specific foods over weeks/months; good for chronic intake |
| Diet History | Detailed usual pattern over long period; comprehensive |
| Weighed Food Record | Food weighed before and after eating; most accurate but laborious |
4. Biochemical / Laboratory Methods:
- Serum albumin, total protein, transferrin (protein status)
- Haemoglobin, serum ferritin (iron status)
- Serum retinol (Vitamin A)
- Urinary iodine excretion (iodine status)
- Serum 25-OH Vitamin D (Vit D status)
PREVENTION AND CONTROL OF MALNUTRITION:
Flowchart:
PREVENTION OF MALNUTRITION
|
┌─────────┼─────────┐
↓ ↓ ↓
Primary Secondary Tertiary
(Before (Early (Treatment
disease) detection) & Rehab)
Primary Prevention:
- Promotion of breastfeeding (exclusive for 6 months)
- Appropriate complementary feeding after 6 months
- Food fortification (iodized salt, iron-fortified flour)
- Dietary diversification
- Growth monitoring and promotion
- Nutrition education
- Food security programs (ICDS, PDS, Mid-Day Meal)
Secondary Prevention:
- Screening for malnutrition (growth monitoring)
- Treatment of micronutrient deficiencies (Vitamin A supplementation, iron-folic acid tablets)
- Management of acute malnutrition at community level
Tertiary Prevention:
- Nutritional Rehabilitation Centres (NRC)
- Therapeutic feeding (F75 and F100 formula feeds for SAM)
- Community-based Management of Acute Malnutrition (CMAM)
LAQ 6: NATIONAL NUTRITIONAL PROGRAMMES OF INDIA (POSHAN ABHIYAN, ICDS, MID-DAY MEAL)
Overview Flowchart:
NATIONAL NUTRITIONAL PROGRAMMES
|
┌─────────────┼──────────────┐
↓ ↓ ↓
ICDS Poshan Mid-Day
(1975) Abhiyan Meal
(2018) Programme
1. ICDS (Integrated Child Development Services) - 1975:
- Launched: 2 October 1975
- Target group: Children (0-6 years), pregnant women, lactating mothers, adolescent girls
- Delivered through: Anganwadi Centres (AWCs)
- Services provided (6 services):
- Supplementary nutrition
- Immunization
- Health check-up
- Referral services
- Non-formal pre-school education
- Nutrition and health education
2. POSHAN ABHIYAN (National Nutrition Mission) - 2018:
- Launched: 8 March 2018 (International Women's Day), Rajasthan
- Aims to reduce stunting, undernutrition, anaemia, and low birth weight
- Targets:
- Reduce stunting by 2% per year
- Reduce underweight by 2% per year
- Reduce anaemia by 3% per year
- Technology-driven: Real-time monitoring through ICDS-CAS (Common Application Software)
- Focus: Convergence of multiple schemes
3. MID-DAY MEAL SCHEME (PM POSHAN - 2021):
- Started: 1995 (National Programme of Nutritional Support to Primary Education)
- Renamed: PM POSHAN Shakti Nirman in 2021
- Target: Children in Classes 1-8 in government/government-aided schools
- Provides: Hot cooked meals
- Calorie norms: 450 kcal + 12g protein (primary); 700 kcal + 20g protein (upper primary)
- Benefits: Increases school enrolment and attendance, reduces hunger, improves nutrition
4. National Nutrition Policy of India (1993) - Salient Features:
- Diet-based approach
- Food fortification
- Popularize low-cost nutritious foods
- Minimum Nutritional Status monitoring
- Prophylaxis against micronutrient deficiencies
- Promotes research in nutrition
LAQ 7: FOOD SAFETY, FOOD PROCESSING, FOOD FORTIFICATION, FOOD ADDITIVES AND FOOD ADULTERATION
KEY DEFINITIONS:
| Term | Definition |
|---|---|
| Food Safety | Assurance that food will not cause harm to the consumer when prepared and/or eaten as intended (WHO) |
| Food Hygiene | All conditions and measures necessary to ensure safety and suitability of food at all stages of the food chain |
| Food Adulteration | Addition of inferior, harmful or foreign substance to food that reduces its quality |
| Food Fortification | Addition of one or more essential nutrients to a food to improve the nutritional quality |
| Food Preservation | Prevention of food spoilage by physical, chemical or biological means |
| Food Additive | Any substance added intentionally to food during production, processing, storage or packaging |
| Food Toxicant | Naturally occurring or artificially introduced toxic substance in food |
WHO'S FIVE KEYS FOR FOOD SAFETY:
- Keep CLEAN - Wash hands, clean utensils
- Separate RAW and COOKED - Avoid cross-contamination
- COOK thoroughly - Heat kills pathogens
- Keep food at SAFE temperatures - Below 5°C or above 60°C
- Use SAFE water and raw materials
FOOD PROCESSING:
Definition: Any method used to convert raw agricultural products into safe, edible, storable food products
Objectives:
- Preserve food from spoilage
- Improve palatability and digestibility
- Extend shelf life
- Improve safety
- Create convenience foods
Methods / Techniques:
| Method | Examples |
|---|---|
| Heat treatment | Pasteurization, sterilization, UHT |
| Cold treatment | Refrigeration (4°C), freezing (-18°C) |
| Drying/Dehydration | Sun drying, spray drying, freeze drying |
| Canning | Hermetically sealed, heat sterilized |
| Fermentation | Yogurt, idli, dosa batter |
| Smoking | Fish, meat |
| Salting/Pickling | Pickles, cured meats |
| Irradiation | Gamma rays to kill pathogens |
Advantages of Food Processing:
- Extends shelf life, reduces wastage
- Destroys pathogens (safety)
- Improves digestibility
- Makes food available in off-season
Disadvantages:
- Loss of nutrients (especially Vitamins B, C)
- Addition of preservatives/additives may be harmful
- Processed foods often high in salt, sugar, fats
FOOD FORTIFICATION:
Definition: Process of adding micronutrients to food to correct or prevent deficiency
Need for Fortification:
- Widespread micronutrient deficiency ("hidden hunger")
- Not everyone can afford/access diverse diets
- Cost-effective public health intervention
Examples in India:
- Iodized salt (prevents iodine deficiency / goitre)
- Iron and folic acid fortified wheat flour (prevents anaemia)
- Vitamin A fortified vanaspati and sugar
- Vitamin D fortified milk
Government Program - Food Fortification Initiative (FFI):
- FSSAI (Food Safety and Standards Authority of India) mandates fortification of staple foods
- Large-scale wheat flour, rice, edible oil, milk fortification
- Logo: "+F" symbol on fortified food packages
FOOD ADDITIVES:
Definition: Any substance not normally consumed as food itself, deliberately added during production, processing, storage or packaging to achieve a technological purpose
Classification of Food Additives:
| Class | Purpose | Examples |
|---|---|---|
| Preservatives | Prevent microbial spoilage | Benzoic acid, Sodium benzoate |
| Antioxidants | Prevent oxidative rancidity | BHA, BHT, Vitamin C |
| Colorants | Improve appearance | Tartrazine, Carmoisine |
| Flavouring agents | Improve flavour | Vanilla, MSG |
| Emulsifiers | Maintain consistency | Lecithin, mono-glycerides |
| Sweeteners | Sugar substitutes | Saccharin, Aspartame |
| Thickeners | Improve texture | Agar, pectin, starch |
| Raising agents | Baking | Baking powder, yeast |
Laws Related to Food Additives in India:
- Prevention of Food Adulteration Act, 1954 (PFA) - now superseded
- Food Safety and Standards Act, 2006 (FSSA) - current legislation
- FSSAI (Food Safety and Standards Authority of India) - regulatory body
- Lays down standards for permitted additives, their maximum permissible limits
FSSAI (Food Safety and Standards Authority of India):
- Established under FSSA 2006
- Autonomous body under Ministry of Health & Family Welfare
- Functions:
- Lay down food safety standards
- Regulate and supervise food safety
- Grant licenses to food businesses
- Conduct surveillance, monitoring, and inspection
- Promote general awareness about food safety
PASTEURIZATION OF MILK:
Definition: Process of heating milk to a specific temperature for a specific time to destroy pathogenic microorganisms without significantly altering its composition or nutritive value
Methods of Pasteurization:
| Method | Temperature | Time | Notes |
|---|---|---|---|
| LTLT (Low Temperature Long Time) | 63°C | 30 minutes | Holder method; batch process |
| HTST (High Temperature Short Time) | 72°C | 15 seconds | Continuous flow; most common |
| UHT (Ultra High Temperature) | 135-150°C | 2-5 seconds | Shelf-stable milk; sterile |
| Boiling | 100°C | 3-5 min | Household method |
Laboratory Tests for Milk Safety:
- Phosphatase Test - Tests adequacy of pasteurization (enzyme destroyed at pasteurization temp)
- Methylene Blue Reduction Test (MBRT) - Bacterial count estimation
- Standard Plate Count (SPC) - Colony counting
- Coliform test - Faecal contamination
- Fat content - Gerber test / Babcock test
SECTION D: ENVIRONMENT AND HEALTH
LAQ 8: WATER AND HEALTH - DEFINE, SOURCES, PURIFICATION, QUALITY STANDARDS
KEY DEFINITIONS:
| Term | Definition |
|---|---|
| Safe Water | Free from harmful microorganisms, toxic chemicals and excessive minerals |
| Wholesome Water | Palatable, aesthetically acceptable, safe for all domestic purposes |
| Improved Drinking Water | Water from a protected source (piped water, borewell, protected spring) |
| Potable Water | Water that is safe and suitable for drinking |
WATER-RELATED DISEASE CLASSIFICATION (Bradley Classification):
WATER-RELATED DISEASES
|
┌─────────┼──────────┬──────────┐
↓ ↓ ↓ ↓
Water- Water- Water- Water-
borne washed based related
diseases diseases diseases (vector)
| | | |
Typhoid, Diarrhoea, Guinea Malaria,
Cholera, Trachoma, worm, Dengue,
Hepatitis Scabies Schisto- Filariasis
A, E somiasis
SOURCES OF WATER:
| Source | Characteristics | Advantages | Disadvantages |
|---|---|---|---|
| Rain water | Naturally distilled | Purest form | Low quantity, may absorb pollutants |
| Surface water (rivers, lakes, ponds) | High microbial contamination | Large quantity | High pollution risk |
| Ground water (wells, borewells, springs) | Filtered by soil | Lower contamination | May have hardness, fluoride |
| Piped water supply | Treated and distributed | Most reliable | Infrastructure cost |
DAILY WATER REQUIREMENTS:
| Purpose | Quantity |
|---|---|
| Drinking | 2-3 litres/person/day |
| Cooking | 5 litres/person/day |
| Bathing | 15-45 litres/person/day |
| Total (minimum) | 50 litres/person/day (WHO) |
| Total (comfortable) | 150-200 litres/person/day |
METHODS OF WATER PURIFICATION:
A. Natural (Household level):
- Storage - Allows sedimentation and natural die-off of bacteria (ineffective alone)
- Sunlight (SODIS) - Solar water disinfection in PET bottles; 6 hours in sunlight
- Boiling - Most reliable household method; kills all pathogens; 100°C for 3-5 minutes
B. Small-Scale / Household Treatment:
RAW WATER
↓
Sedimentation (allow particles to settle - 24 hrs)
↓
Filtration (Candle filter / Slow sand filter)
↓
Disinfection (Chlorine tablets / Boiling / UV)
↓
SAFE STORAGE (covered container)
C. Large-Scale (Community Level):
SOURCE WATER
↓
COAGULATION (Alum added; floc forms)
↓
FLOCCULATION (Slow mixing; floc particles aggregate)
↓
SEDIMENTATION (Floc settles; removes turbidity, 70-80% bacteria)
↓
FILTRATION (Rapid sand filter / Slow sand filter)
↓
DISINFECTION (Chlorination: 0.5 ppm residual chlorine)
↓
STORAGE & DISTRIBUTION
↓
FLUORIDATION (optional; 0.7-1.0 ppm)
Chlorination:
- Most widely used disinfectant
- Residual chlorine: 0.2-0.5 mg/L at point of use
- BLEACHING POWDER: 30% available chlorine; 2-4 kg/million liters for clear water
- Breakpoint chlorination: Enough chlorine to satisfy demand + residual 0.2 ppm
WATER QUALITY STANDARDS (BIS/WHO):
| Parameter | WHO Guideline | BIS Standard (India) |
|---|---|---|
| pH | 6.5-8.5 | 6.5-8.5 |
| Turbidity | <1 NTU (ideal) | 1 NTU (desirable), 5 NTU (permissible) |
| Total Dissolved Solids | 600 mg/L | 500 mg/L |
| Coliform bacteria | 0 (absent) | 0 in 100 mL |
| Fluoride | 1.5 mg/L | 1.0 mg/L |
| Nitrate | 50 mg/L | 45 mg/L |
| Arsenic | 0.01 mg/L | 0.01 mg/L |
FLUORIDATION OF WATER:
- Optimal level: 0.7-1.0 mg/L (WHO recommends 1.5 mg/L maximum)
- Prevents dental caries
- Excess fluoride (>1.5 mg/L): Fluorosis (dental mottling, skeletal fluorosis)
- Deficient fluoride: Increased dental caries
JAL JEEVAN MISSION (National Rural Drinking Water Programme):
- Launched: 15 August 2019
- Goal: Provide Functional Household Tap Connection (FHTC) to every rural household by 2024
- "Har Ghar Jal" - water in every home
- Potable water: 55 litres per person per day
- Focus: Water quality testing, women participation
LAQ 9: AIR POLLUTION - CAUSES, EFFECTS, COMPONENTS, AQI AND PREVENTION
Definition:
"Environmental pollution is the presence of a substance in the environment at a concentration which is harmful to human beings, plants, animals or which interferes with well-being of the ecosystem." - Park's PSM
SOURCES / CAUSES OF AIR POLLUTION:
AIR POLLUTION SOURCES
|
┌────────┴────────┐
↓ ↓
NATURAL MAN-MADE (Anthropogenic)
SOURCES SOURCES
| |
Volcanoes, ┌─────────┼──────────┐
Dust storms, ↓ ↓ ↓
Forest fires Industry Transport Domestic
(factories, vehicles, (cooking,
power plants) aircraft) burning)
COMPONENTS OF AIR POLLUTANTS:
| Pollutant | Sources | Health Effects |
|---|---|---|
| Particulate Matter (PM2.5/PM10) | Dust, combustion | Lung disease, CVD, cancer |
| Sulphur Dioxide (SO₂) | Coal burning, smelters | Bronchitis, acid rain |
| Nitrogen Oxides (NOₓ) | Vehicles, power plants | Lung damage, smog |
| Carbon Monoxide (CO) | Incomplete combustion | Headache, asphyxia |
| Ozone (O₃) | Secondary pollutant | Eye/lung irritation |
| Lead | Leaded petrol (historical) | Neurotoxic, especially children |
| VOCs | Paints, solvents | Cancer (benzene = leukemia) |
HEALTH EFFECTS OF AIR POLLUTION:
Acute Effects:
- Eye irritation, burning
- Coughing, sneezing
- Exacerbation of asthma/COPD
- CO poisoning: headache, nausea, death
Chronic Effects:
- Chronic bronchitis, emphysema, COPD
- Lung cancer (PM2.5, PAH, benzene)
- Cardiovascular disease (PM2.5, NO₂)
- Neurological damage (lead, mercury)
- Developmental effects in children (lead)
- Increased mortality
AIR QUALITY INDEX (AQI):
| AQI Range | Category | Health Implications |
|---|---|---|
| 0-50 | Good | Minimal impact |
| 51-100 | Satisfactory | Minor discomfort to sensitive individuals |
| 101-200 | Moderate | Breathing discomfort to asthma/elderly |
| 201-300 | Poor | Breathing discomfort to most people |
| 301-400 | Very Poor | Respiratory illness on prolonged exposure |
| 401-500 | Severe | Healthy people also affected |
PREVENTION AND CONTROL OF AIR POLLUTION:
Technical Measures:
- Use of cleaner fuels (CNG, LPG, electric vehicles)
- Electrostatic precipitators, scrubbers in industry
- Catalytic converters in vehicles
- Transition to renewable energy (solar, wind)
Legislative Measures:
- Air (Prevention and Control of Pollution) Act, 1981
- Environment Protection Act, 1986
- National Ambient Air Quality Standards (NAAQS)
- Bharat Stage Emission Standards (BS-VI)
Behavioural/Public Health Measures:
- Promoting public transport, cycling
- Reducing open burning (crop stubble, waste)
- Tree planting / Green corridors
- Construction dust control measures
- AQI alerts to public
LAQ 10: HOUSING AND HEALTH - HEALTHFUL HOUSING, STANDARDS, HAZARDS OF OVERCROWDING
Definition of Healthful Housing:
"Healthful housing means construction of a house so as to create and maintain healthy conditions for the occupants and their neighbors." - Park's PSM
CHARACTERISTICS OF HEALTHFUL HOUSING:
1. Site:
- High, well-drained land
- Free from flooding
- Away from swamps, nuisance industries
- Near school, market, health centre
2. Physical Structure:
- Adequate floor space (min 9 sq m per person)
- Adequate ventilation (windows on opposite walls)
- Adequate natural lighting
- Smooth, cleanable walls and floors
- Proof against insects and rodents
3. Essential Services:
- Safe water supply
- Sanitary disposal of excreta and refuse
- Electricity
HOUSING STANDARDS (India - CPWD/BIS):
- Floor area: 9.5 sq m per person minimum
- Ventilation: Windows = 1/10 of floor area (minimum)
- Ceiling height: 2.75 m minimum
- Cubic air space: 14.2 m³ per person minimum
FACTORS AFFECTING HEALTHFUL HOUSING:
- Socioeconomic status (poverty)
- Land availability and cost
- Cultural practices (joint families)
- Government housing policies
- Urbanization and migration
- Building regulations enforcement
HAZARDS OF OVERCROWDING:
Definition: Overcrowding = more than 2 persons per habitable room OR less than 5.6 m³ space per adult
Health Hazards:
OVERCROWDING
|
┌────┴─────┐
↓ ↓
DIRECT INDIRECT
EFFECTS EFFECTS
| |
Facilitates Mental
disease health
spread stress
|
Airborne: TB, measles,
meningitis,
influenza
Faecal-oral: diarrhea,
typhoid
Skin: scabies,
ringworm
|
Sleep deprivation
Domestic accidents
Domestic violence
Sexual abuse
Specific Diseases Associated with Overcrowding:
- Tuberculosis (most important)
- Meningococcal meningitis
- Influenza, COVID-19
- Measles, chickenpox
- Typhus (louse-borne)
- Scabies, tinea
Problems in Poor Housing:
- Dampness - mould growth, respiratory disease
- Lack of ventilation - CO poisoning, respiratory infections
- Inadequate lighting - eye strain, accidents
- Pest infestation (rats, mosquitoes) - rodent-borne diseases
- No safe water - waterborne diseases
- No sanitation - fecal-oral diseases
LAQ 11: RADIATION AND HEALTH - TYPES, SOURCES, EFFECTS AND PREVENTION
Types of Radiation:
RADIATION
|
┌───┴───┐
↓ ↓
IONIZING NON-IONIZING
| |
Alpha, X-rays UV, Infrared,
Beta, Radio waves,
Gamma Microwaves
SOURCES OF RADIATION EXPOSURE:
| Source | Type | Examples |
|---|---|---|
| Natural background | Ionizing | Cosmic rays, radon gas, rocks (granite) |
| Medical | Ionizing | X-rays, CT scans, nuclear medicine |
| Nuclear industry | Ionizing | Power plants, weapons testing |
| Consumer products | Ionizing | Smoke detectors (Am-241) |
| Sunlight | Non-ionizing | UV-A, UV-B |
| Mobile phones | Non-ionizing | Radiofrequency electromagnetic fields |
HEALTH EFFECTS OF RADIATION:
Ionizing Radiation:
| Effect | Description |
|---|---|
| Deterministic effects | Dose-dependent; have threshold; acute radiation syndrome, burns, cataracts |
| Stochastic effects | Probabilistic; no threshold; cancer, genetic mutations |
Acute Radiation Syndrome (ARS):
- High doses (>1 Gy): nausea, vomiting, bone marrow suppression, death
- Hematopoietic syndrome: bone marrow failure
- GI syndrome: intestinal epithelium destruction
- CNS syndrome: most severe; cerebral oedema, rapid death
Chronic Effects:
- Cancers: leukemia (most common), thyroid, breast, lung
- Cataracts (eye lens)
- Genetic mutations in offspring
- Aplastic anaemia
Non-Ionizing (UV) Radiation Effects:
- Sunburn, premature aging of skin
- Skin cancer (melanoma, non-melanoma)
- Cataracts
- Immune suppression
PREVENTION AND PROTECTION AGAINST RADIATION:
Principles (3 Ts):
- Time - Minimize time of exposure
- Distance - Maximize distance from source (inverse square law)
- Shielding - Use appropriate shielding material
Specific Measures:
- Lead aprons, thyroid shields in X-ray departments
- Dosimetry badges for radiation workers
- ALARA principle: As Low As Reasonably Achievable
- Iodine tablets (KI) for nuclear accidents (protects thyroid from I-131)
- Limiting medical radiation (justify each investigation)
- Sunscreen, protective clothing for UV
LAQ 12: NOISE AND HEALTH - EFFECTS, PREVENTION
Definition:
Noise = Unwanted sound; measured in decibels (dB)
Health Effects of Noise:
| Level (dB) | Effect |
|---|---|
| 0-40 dB | Comfortable |
| 40-65 dB | Annoyance, sleep disturbance |
| 65-85 dB | Psychological stress |
| 85-95 dB | Hearing impairment with prolonged exposure |
| >120 dB | Immediate pain and hearing damage |
Auditory Effects:
- Noise-Induced Hearing Loss (NIHL) - most important
- Tinnitus (ringing in ears)
- Temporary Threshold Shift (TTS) - reversible
- Permanent Threshold Shift (PTS) - irreversible
Non-Auditory Effects:
- Cardiovascular: hypertension, increased heart rate
- Psychological: anxiety, irritability, decreased concentration
- Sleep disturbance, fatigue
- Interference with communication
- Reduced work efficiency
Prevention:
- Engineering controls: noise barriers, mufflers, sound-absorbing materials
- Administrative controls: rotate workers, limit exposure hours
- Personal protection: earplugs (25 dB attenuation), earmuffs
- Legislative: Noise Pollution (Regulation and Control) Rules, 2000
- Standards: Industrial noise <90 dB for 8 hours/day; residential area: day 55 dB, night 45 dB
LAQ 13: VENTILATION AND HEALTH
Definition:
"Ventilation is the process of supplying and removing air by natural or mechanical means to and from any space in a building."
Types of Ventilation:
| Type | Mechanism | Examples |
|---|---|---|
| Natural ventilation | Wind pressure + temperature difference | Windows, doors, cowl ventilators |
| Artificial / Mechanical | Fans, blowers, AC systems | Supply/exhaust systems, HVAC |
| Special systems | Hospitals, labs | Laminar flow, HEPA filters |
Standards for Adequate Ventilation:
- Air changes per hour: 6-10 changes in living rooms; 15-20 in hospitals
- CO₂ level: should not exceed 0.1% (1000 ppm)
- Temperature: 18-24°C (comfortable range)
- Relative humidity: 40-60%
- Air velocity: 0.1-0.2 m/s (draught-free)
Effects of Inadequate Ventilation:
- Accumulation of CO₂ → headache, drowsiness, suffocation
- Build-up of CO (if combustion indoors) → poisoning, death
- Increased humidity → mould growth → asthma, allergies
- Spread of airborne infections (TB, measles, COVID-19)
- Radon accumulation → lung cancer
- Sick Building Syndrome
SECTION E: SOCIAL AND BEHAVIOURAL HEALTH
LAQ 14: HEALTH BEHAVIOUR, ILLNESS BEHAVIOUR, SICK ROLE BEHAVIOUR AND HEALTH-SEEKING BEHAVIOUR
KEY DEFINITIONS:
Health Behaviour (Kasl and Cobb, 1966):
"Any activity undertaken by a person believing themselves to be healthy, for the purpose of preventing disease or detecting it at an asymptomatic stage."
Illness Behaviour:
"Any activity undertaken by a person who feels ill, to define the state of his health and to discover a suitable remedy." - Mechanic (1961)
Sick Role Behaviour (Parsons, 1951):
The behaviour expected from a person who is declared sick. It has 4 components:
- Person is exempt from normal social responsibilities
- Person cannot recover by willpower alone; needs help
- Person must try to get well
- Person must seek technically competent help
Health Risk Behaviour:
Any behaviour that increases the risk of developing disease (smoking, sedentary lifestyle, unprotected sex, alcohol)
HEALTH-SEEKING BEHAVIOUR:
Definition: The actions taken by individuals when they perceive themselves to be unwell, to find an appropriate remedy
Factors Influencing Health-Seeking Behaviour:
HEALTH-SEEKING BEHAVIOUR
|
┌─────────┼────────┬─────────┐
↓ ↓ ↓ ↓
Patient Provider Health Community
Factors Factors System Factors
| | Factors |
Age, sex, Cost, Availability, Culture,
education competence distance stigma
perception quality waiting social
of illness time support
Barriers to Good Health-Seeking Behaviour:
- Financial: cost of consultation, medicines, transport
- Geographical: distance from health facility
- Social/Cultural: stigma, traditional healers preferred
- Educational: low health literacy
- System barriers: long waiting times, poor quality, unfriendly staff
- Fear of diagnosis, denial
Methods to Overcome Barriers:
- Community health workers (ASHA, ANM) to improve access
- Health education and awareness programmes
- Telemedicine and mobile health clinics
- Free essential drugs and diagnostics (Jan Aushadhi)
- Community engagement and trust building
- Cultural sensitivity in health services
LAQ 15: SOCIAL DETERMINANTS OF HEALTH
Definition (WHO Commission on Social Determinants of Health):
"The conditions in which people are born, grow, live, work and age. These circumstances are shaped by the distribution of money, power and resources at global, national and local levels."
SOCIAL DETERMINANTS (BEINGS framework applied socially):
SOCIAL DETERMINANTS OF HEALTH
|
┌─────────────┼──────────────┐
↓ ↓ ↓
SOCIOECONOMIC PHYSICAL SOCIAL &
CONDITIONS ENVIRONMENT COMMUNITY
| | CONTEXT
Income, Housing, |
Education, Transport, Social support,
Employment, Clean water, Discrimination,
Occupation Safe food Community
cohesion
Key Social Determinants:
- Income and social protection - poverty is the biggest determinant
- Education - health literacy, behaviour change
- Employment and working conditions - occupational health
- Housing - overcrowding, sanitation
- Food security - nutritional status
- Social support networks - mental health, resilience
- Gender - inequalities in health access for women
- Culture and ethnicity - traditional beliefs, discrimination
- Health systems - access, quality, affordability
"Health is not just a medical issue, it is a social, economic and political issue." - Park's PSM
LAQ 16: COMMUNITY - DEFINITION, TYPES (BRINT), COMMUNITY BEHAVIOUR AND ENGAGEMENT
Definition of Community:
"A group of people who share a common place, common interests, common problems and have developed a capacity to act collectively." - Park's PSM
Brint's Definition: A community is a group of people who share a sense of identity, culture, history, or location and who have social bonds with each other.
TYPES OF COMMUNITY (Brint, 2001):
| Type | Based on | Example |
|---|---|---|
| Gemeinschaft (Community of Place) | Geographic proximity | Village, neighbourhood |
| Community of Interest | Shared interests | Professional associations |
| Community of Faith | Religion | Church/Mosque congregations |
| Community of Need | Shared problems | Self-help groups, patient groups |
| Imagined Community | Shared identity/nationality | Nation-state |
COMMUNITY BEHAVIOUR:
The norms, values, traditions, and collective actions of a community that influence health
Importance of Community Behaviour for Public Health:
- Shapes health practices (diet, hygiene, immunization acceptance)
- Determines social support during illness
- Affects healthcare-seeking behaviour
- Community mobilization is essential for disease control programs
- Community behaviour discipline = study of collective behaviours affecting health
COMMUNITY ENGAGEMENT / COMMUNITY RELATIONSHIP:
Definition:
"The process of working collaboratively with groups of people affiliated by geographic proximity, special interests, or similar situations, to address issues affecting their well-being." - CDC
Importance of Community Relationships:
- Builds trust between health services and community
- Improves acceptance of health programs
- Identifies locally relevant health problems
- Sustains health interventions beyond program periods
- Promotes health equity and social justice
- Essential for the Homoeopath practicing at community level
Principles of Community Engagement:
- Respect for community values and culture
- Transparency and honesty
- Two-way communication
- Shared decision-making
- Building on community strengths and assets
SECTION F: SANITATION AND EXCRETA DISPOSAL
LAQ 17: EXCRETA DISPOSAL - METHODS, SANITARY BARRIERS AND SEWAGE SYSTEM
Sanitation Definition:
"The provision of facilities and services for the safe disposal of human urine and faeces." - WHO
TYPES OF EXCRETA DISPOSAL METHODS:
Unsanitary Methods:
- Open defecation in fields, bushes, water bodies
- Wrap and throw method
- Shallow pit (non-lined)
Sanitary Methods:
SANITARY EXCRETA DISPOSAL
|
┌──────────┼──────────┐
↓ ↓ ↓
Non-water Water- Sewerage
carriage carriage Systems
methods methods
| | |
Pit latrine, Pour-flush WC + sewer
Compost latrine, network
latrine, Septic tank
SULABH
TYPES OF LATRINES:
| Type | Features | Suitable for |
|---|---|---|
| Pit latrine | Single pit, superstructure; VIP variety uses ventilation | Rural areas |
| Pour-flush latrine | Water seal (P/S/U trap) blocks odour; pit or leach pit | Rural/peri-urban |
| Composting toilet | Converts excreta to compost; no water needed | Waterless areas |
| Septic tank | Two-chambered; solids settled, liquids disposed in soak pit | Individual homes |
| Sanitary latrine (water closet) | Connected to sewerage system | Urban areas |
PRINCIPLES OF SANITARY LATRINE:
- Prevent access of flies, rodents, insects to excreta
- Prevent contamination of soil, water
- No objectionable odour
- No aesthetic nuisance
- Easy to construct and maintain
- Affordable
SEWERAGE SYSTEM:
Components:
- House connections - from WC to main sewer
- Lateral sewers - small pipes collecting from houses
- Main sewers / Trunk sewers - large pipes carrying to treatment
- Lift stations - pumps to raise sewage where gravity is insufficient
- Sewage Treatment Plant (STP)
Sewage Treatment Process:
RAW SEWAGE
↓ Preliminary Treatment
Screen (removes large objects) + Grit chamber
↓ Primary Treatment
Sedimentation (removes 50-60% SS, 25-35% BOD)
↓ Secondary Treatment
Biological treatment (removes 90% BOD)
- Activated sludge process / Trickling filter
↓ Tertiary Treatment
Chlorination, filtration (removes remaining pathogens)
↓
TREATED EFFLUENT (discharged to water body)
BOD (Biochemical Oxygen Demand):
- Amount of oxygen needed by microorganisms to decompose organic matter in water
- Raw sewage BOD: 200-400 mg/L
- Treated effluent: <30 mg/L (standard)
- High BOD = high organic pollution
COD (Chemical Oxygen Demand):
- Oxygen needed to oxidize all chemical substances in water
- Includes both biodegradable and non-biodegradable organic matter
SWACHH BHARAT ABHIYAN / MISSION:
- Launched: 2 October 2014 (Mahatma Gandhi's birth anniversary)
- Goal: Open Defecation Free (ODF) India
- Achievements: Construction of millions of household toilets; India declared ODF in 2019 (rural)
- Phase 2: Solid waste management, greywater management, ODF+
LAQ 18: BIOMEDICAL WASTE MANAGEMENT
Definitions:
Biomedical Waste (BMW):
"Any waste which is generated during the diagnosis, treatment or immunization of human beings or animals, or in research activities pertaining thereto, or in the production or testing of biologicals." - Biomedical Waste (Management and Handling) Rules, 1998 (amended 2016)
Hospital Waste: All waste generated in hospital/health facility
CLASSIFICATION OF BIOMEDICAL WASTE (BMW Rules 2016):
| Category | Type | Disposal |
|---|---|---|
| Yellow | Infectious, pathological, pharmaceutical waste | Incineration or deep burial |
| Red | Contaminated recyclable waste (IV bags, syringes without needle) | Autoclaving + recycling |
| White (Puncture proof) | Sharps (needles, blades) | Sharp pit or autoclaving |
| Blue | Broken glass, metallic implants | Sharp pit |
MANAGEMENT STEPS (Flowchart):
GENERATION of BMW at source
↓
SEGREGATION (at point of generation)
(Colour-coded bins: Yellow/Red/White/Blue)
↓
COLLECTION & TRANSPORTATION
(Labelled, leak-proof containers; closed trolleys)
↓
STORAGE (max 48 hours at facility)
↓
TREATMENT
↓ ↓ ↓
INCINERATION AUTOCLAVING CHEMICAL
(Yellow waste) (Red waste) DISINFECTION
↓
FINAL DISPOSAL
TREATMENT TECHNOLOGIES:
| Technology | Applicable Waste | Principle |
|---|---|---|
| Incineration | Infectious, pathological, pharmaceutical | High-temperature combustion (850-1200°C) |
| Autoclaving | Sharps, cultures, infectious | Steam under pressure (134°C, 18 min) |
| Chemical disinfection | Liquid waste, some sharps | Sodium hypochlorite, formaldehyde |
| Microwave | Infectious waste | Microwave energy + steam |
| Deep burial | Pathological, body parts | In remote areas only |
BMW RULES IN INDIA:
- Biomedical Waste Management Rules, 2016 (replaced 1998 rules)
- Key provisions:
- Hospitals must have an Authorization from State Pollution Control Board
- Bar-coded bags and containers mandatory
- Annual report to State PCB
- Training to all staff
- Common Biomedical Waste Treatment Facilities (CBWTFs) for smaller units
SECTION G: TEMPERATURE AND SPECIAL ENVIRONMENTS
LAQ 19: EFFECTS OF HOT ENVIRONMENT, HEAT STROKE, HEAT EXHAUSTION AND PREVENTION
Heat-Related Illness Classification:
HOT ENVIRONMENT HEALTH EFFECTS
|
┌────────────┼─────────────┐
↓ ↓ ↓
MILD MODERATE SEVERE
| | |
Heat Heat HEAT
cramps exhaustion STROKE
(muscle) (fatigue, (Medical emergency)
sweating)
COMPARISON: Heat Exhaustion vs Heat Stroke:
| Feature | Heat Exhaustion | Heat Stroke |
|---|---|---|
| Core Temperature | <40°C | >40°C (often 41-42°C) |
| Sweating | Profuse sweating | Absent (anhidrosis) |
| Mental status | Normal/mildly confused | Disoriented, unconscious |
| Skin | Pale, moist, cool | Red, dry, hot |
| Pathology | Volume depletion | Thermoregulatory failure |
| Urgency | Urgent care | MEDICAL EMERGENCY |
FIRST AID for Heat Stroke:
- Call emergency services immediately
- Move to cool shaded area
- Remove excess clothing
- Rapid cooling: ice packs to neck, axilla, groin; cool water spraying
- IV fluids (if available)
- Monitor and transfer to hospital
PREVENTION:
- Avoid outdoor activity 11am-4pm in summer
- Wear light, loose, light-coloured clothing
- Stay hydrated (ORS, water, lemon water)
- Avoid alcohol and caffeinated beverages
- Use shade, fans, AC
- Buddy system for outdoor workers
- Heat health action plans (HHAP) - India has National Action Plan for Heat
LAQ 20: EFFECTS OF COLD ENVIRONMENT - HYPOTHERMIA, FROSTBITE AND PREVENTION
Definitions:
- Hypothermia: Core body temperature <35°C
- Frostbite: Freezing of skin and underlying tissues
HYPOTHERMIA - Stages:
| Stage | Core Temp | Signs |
|---|---|---|
| Mild | 32-35°C | Shivering, confusion, impaired coordination |
| Moderate | 28-32°C | No shivering, drowsy, arrhythmias |
| Severe | <28°C | Unconscious, no pulse, death risk |
FROSTBITE - Degrees:
| Degree | Features |
|---|---|
| 1st (Frostnip) | Superficial; red, painful; no blistering |
| 2nd | Blistering, superficial necrosis |
| 3rd | Deep; haemorrhagic blisters; full skin thickness |
| 4th | All layers + muscle/bone; gangrene |
FIRST AID FOR COLD INJURIES:
- Remove from cold environment
- Remove wet clothing
- Gradual rewarming (warm room, warm drinks, warm water 38-42°C for frostbite)
- Do NOT rub frostbitten tissue
- Do NOT rewarm if refreezing is possible
- Homoeopathic: Agaricus muscarius (frostbite), Camphora (hypothermia)
PREVENTION OF COLD ILLNESS:
- Layered clothing (wool/synthetic, not cotton)
- Cover extremities: gloves, socks, hat
- High calorie diet (generates heat)
- Avoid alcohol (causes vasodilation, increases heat loss)
- Shelter from wind
- Buddy system in extreme cold environments
LAQ 21: HIGH ALTITUDE ILLNESS - ADVERSE EFFECTS, PREVENTION AND FIRST AID
High Altitude Definition:
- High altitude: 2500-3500 m
- Very high: 3500-5500 m
- Extreme altitude: >5500 m
TYPES OF HIGH ALTITUDE ILLNESS:
HIGH ALTITUDE ILLNESS
|
┌─────────┼──────────┐
↓ ↓ ↓
AMS HACE HAPE
(Acute (High Alt (High Alt
Mountain Cerebral Pulmonary
Sickness Oedema) Oedema)
| Condition | Features | Management |
|---|---|---|
| AMS (Acute Mountain Sickness) | Headache + nausea/fatigue/dizziness within 6-12 hrs of ascent | Rest, descent, acetazolamide |
| HACE | AMS + ataxia, altered consciousness; cerebral oedema | Immediate descent, dexamethasone, oxygen |
| HAPE | Breathlessness at rest, cough, frothy sputum; pulmonary oedema | MOST DANGEROUS; immediate descent, nifedipine, oxygen |
PREVENTION:
- Gradual ascent (not more than 300-500 m/day above 3000 m)
- Acclimatization (rest day every 1000 m gain)
- Acetazolamide 250 mg BD starting 24 hours before ascent (prophylaxis)
- Stay hydrated
- Avoid alcohol
- Know the rule: "Climb high, sleep low"
FIRST AID:
- DESCEND IMMEDIATELY for HACE or HAPE (most important)
- Supplemental oxygen
- Portable hyperbaric chamber (Gamow bag) if descent not immediately possible
- Dexamethasone (HACE), Nifedipine (HAPE)
- Homoeopathic: Coca (altitude sickness)
QUICK REVISION TABLES
Comparison: Community Medicine vs Public Health vs Preventive Medicine
| Community Medicine | Public Health | Preventive Medicine | |
|---|---|---|---|
| Focus | Populations | Community | Individuals |
| Tool | Epidemiology | Sanitation/Legislation | Clinical skills |
| Setting | Community/Academic | Government | Clinic/Hospital |
WHO Definition Summary:
- Health (1948): Complete physical, mental and social well-being
- Public Health (Winslow): Science and art of preventing disease...through organized community efforts
- Environment: All that is external to the individual human host (physical, biological, social)
- Malnutrition: Pathological state from relative/absolute deficiency or excess of nutrients
All answers sourced from:
- Park's Textbook of Preventive and Social Medicine (Park's PSM), 26th Edition
- Leavell & Clark, Preventive Medicine for the Doctor in His Community
- WHO Technical Reports and Guidelines
- FSSAI, GoI Guidelines; BMW Rules 2016; Jal Jeevan Mission documents
- MacMahon B & Pugh TF - Epidemiologic Principles and Methods
This is a shared conversation. Sign in to Orris to start your own chat.