Preterm pediatrics
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Searching PubMed
"preterm infant" AND management
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
This is your complete exam-prep guide on preterm pediatrics. Here is a quick orientation to what is covered:
Definitions & Classification - GA-based categories (late/very/extremely preterm, periviable) and birth weight categories (LBW, VLBW, ELBW), with epidemiologic context.
The "Big 5" Complications (almost exclusively preterm):
- RDS - surfactant deficiency, CXR ground glass pattern, treated with antenatal steroids + surfactant replacement
- BPD - chronic lung disease from ventilation/O2 injury, defined as O2 need >28 days in <32-week infant
- IVH - germinal matrix bleeding, Papile grades I-IV, screening by cranial U/S, prevented by antenatal steroids + MgSO4
- NEC - intestinal necrosis, pneumatosis intestinalis on imaging, Bell staging, breast milk is protective
- ROP - retinal neovascularization from O2 exposure, 5 stages, screened by ophthalmology per strict GA-based protocol, treated with laser or anti-VEGF
Other key topics: PDA management, apnea of prematurity (caffeine), thermoregulation, nutrition (breast milk + human milk fortifier), antenatal corticosteroids, and late preterm infant risks.
Ask if you want any section expanded further - for example, IVH grading images, surfactant types, or NICU ventilation strategies.
Acute diarrhea disease Management algorithm
Reading File
Finding Sources
Finding Sources
Searching PubMed
"acute diarrhea" AND management AND guidelines
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
Loading Image
Reading File
Excellent - I now have the full Harrison's algorithm, textbook treatment protocols, and pathogen-specific data. Here is the comprehensive management guide:
Acute Diarrhea Disease - Management Algorithm
Pathophysiology Classification
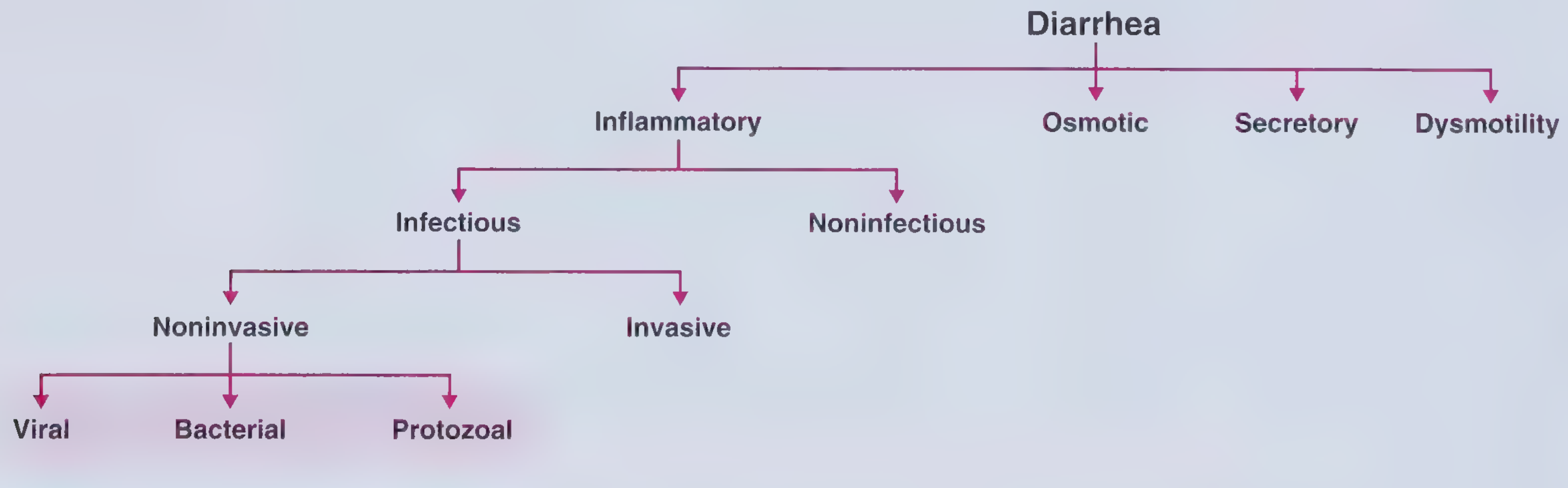
Classification of diarrhea - Frameworks for Internal Medicine
Step 1 - Initial Assessment: History and Physical
The first branch point is infectious vs. noninfectious.
Features suggesting infectious etiology:
- Acute onset (<14 days)
- Nausea, vomiting, fever
- Epidemiologic clues: recent travel, contaminated food/water, sick contacts, outbreaks (cruise ships, daycare, nursing homes)
- Recent antibiotic use (think C. difficile)
Features suggesting noninfectious etiology:
- New medication (hundreds of drugs cause diarrhea)
- Post-surgical bowel changes
- IBD flare, ischemic colitis, partial obstruction
- Radiation exposure → If likely noninfectious: evaluate and treat the underlying cause separately.
Step 2 - Severity Stratification (determines urgency)
| Severity | Description | Action |
|---|---|---|
| Mild | Unrestricted daily activity; few loose stools | Observe + oral fluids |
| Moderate | Activities altered; multiple stools; some cramping | ORS + symptomatic treatment |
| Severe | Incapacitated; profuse stool output; dehydration signs | IV rehydration + urgent workup |
Fluid and electrolyte replacement is the cornerstone at ALL severity levels.
Step 3 - Rehydration (Always First)
Oral Rehydration Therapy (ORT)
- Indicated for mild to moderate diarrhea with any dehydration
- Works by Na⁺-glucose co-transport in small bowel (intact even during acute diarrhea)
- WHO ORS formula: ½ tsp salt + 6 tsp sugar + 1 L clean water
- Commercial premixed solutions (e.g., Pedialyte, Ceralyte) are equivalent
- Zinc supplementation (10 mg/day <6 months; 20 mg/day ≥6 months) for children in resource-limited settings - reduces severity, duration, and recurrence
IV Rehydration
- Indicated for severe diarrhea with significant volume depletion, unable to tolerate oral intake, or profoundly dehydrated patients (especially infants and elderly)
- Fluids: Ringer's lactate (preferred) or normal saline
- Transition to ORS as tolerated
Step 4 - Decision: Evaluate or Observe?
Indications for stool microbiological studies (Harrison's Principles of Internal Medicine, 22e):
| Indication | Rationale |
|---|---|
| Profuse diarrhea with dehydration | Severity demands identification |
| Overtly bloody stools | Invasive pathogen; antibiotic decision needed |
| Fever ≥ 38.5°C | Systemic infection likely |
| Duration >48 h without improvement | Not self-limited |
| Recent antibiotic use | C. difficile possible |
| New community outbreak | Public health implications |
| Severe abdominal pain, age >50 | Ischemia/other pathology |
| Elderly (≥70 yr) or immunocompromised | High-risk host |
If none of the above: observe + symptomatic treatment - most acute diarrhea is self-limited viral gastroenteritis.
Diagnostic Workup (when indicated)
- First-line: Multiplex PCR stool panel - rapid, sensitive, cost-effective; identifies common bacteria, viruses, parasites simultaneously
- Stool culture - used when multiplexed tests unavailable, for outbreak investigation, or antibiotic sensitivity needed
- Fecal leukocytes / calprotectin - elevated = invasive/inflammatory etiology
- C. difficile toxin EIA or PCR - if recent antibiotics, hospitalization, or prolonged course
- Ova and parasites (O&P) - if travel history, immunocompromised, or diarrhea lasting >7-10 days
- Specific cultures - EHEC (O157:H7), Vibrio, Yersinia if clinical clues present
Step 5 - Management Algorithm (Harrison's, Fig. 49-3)
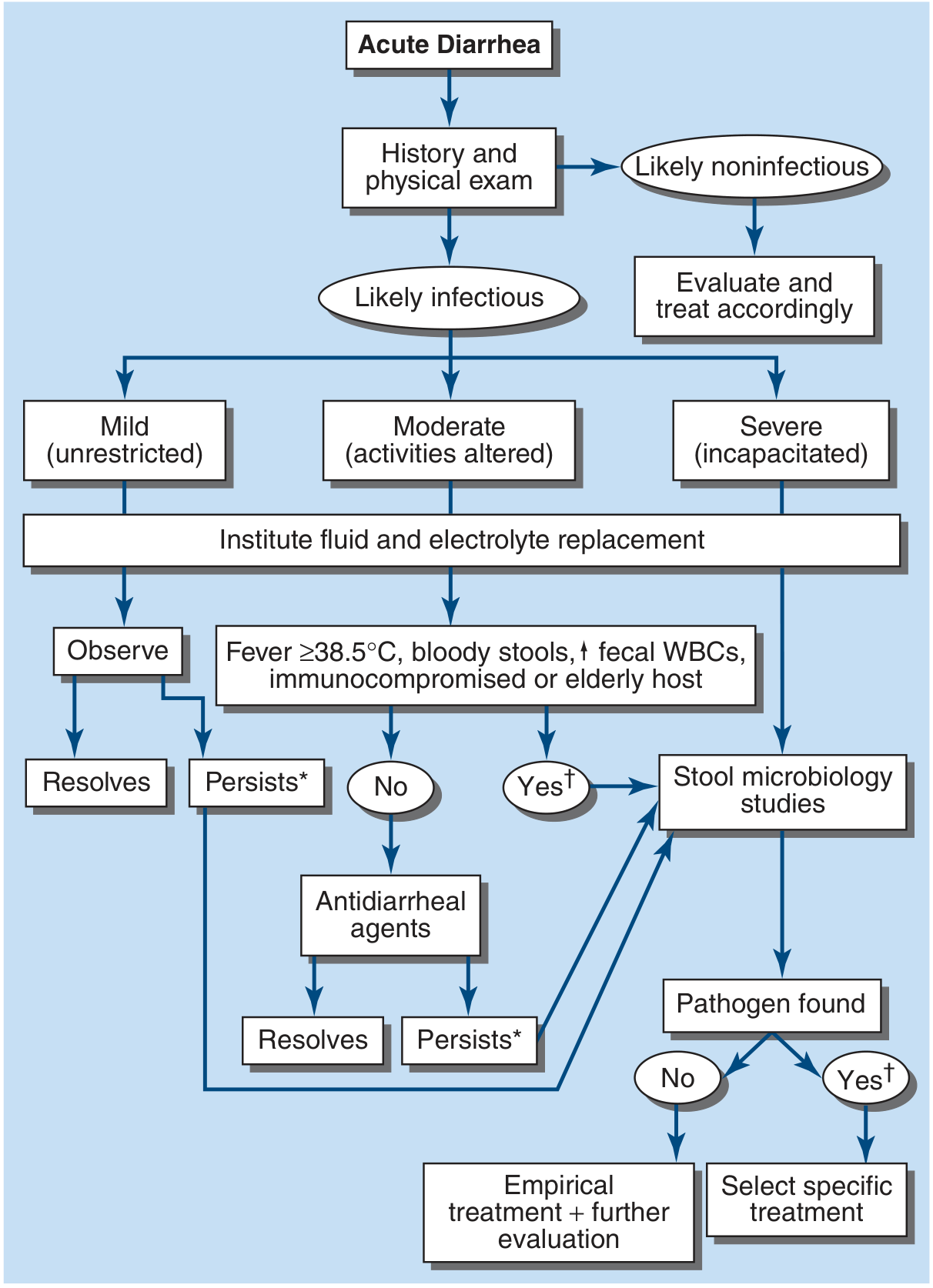
FIGURE 49-3 Algorithm for the management of acute diarrhea. [] = consider empirical metronidazole; [†] = consider empirical quinolone. - Harrison's Principles of Internal Medicine 22e*
Reading the Algorithm:
Acute Diarrhea
↓
History & Physical
↙ ↘
Likely Infectious Likely Noninfectious → Evaluate & Treat
↓
Severity: Mild / Moderate / Severe
↓
FLUID & ELECTROLYTE REPLACEMENT (all patients)
↙ ↘
Mild: Observe Fever ≥38.5°C, bloody stools,
↓ ↑ fecal WBCs, immunocompromised, elderly
Resolves? ↙ ↘
Yes → done No Yes
No → Antidiarrheal Stool Microbiology Studies
agents ↙ ↘
↓ Pathogen Pathogen
Resolves? NOT found Found
Yes → done ↓ ↓
No → ↓ Empirical Tx + Specific Tx
Stool microbiology Further evaluation
Step 6 - Symptomatic (Non-Antibiotic) Treatment
Antimotility Agents
- Loperamide 4 mg initial dose, then 2 mg after each unformed stool (max 16 mg/day)
- Use only in nonfebrile, non-bloody diarrhea (moderate, watery)
- AVOID with:
- Febrile dysentery (prolongs illness)
- Bloody/mucoid stools
- Suspected EHEC O157:H7 or Shigella (may worsen HUS risk)
- C. difficile
Bismuth Subsalicylate
- 524 mg every 30-60 min as needed, up to 8 doses/day
- Useful for mild diarrhea and viral gastroenteritis; reduces nausea and stool frequency
- Avoid in: immunocompromised, renal impairment (bismuth encephalopathy risk)
- Contains salicylate - avoid in children (Reye syndrome risk)
Probiotics
- Not recommended as treatment for acute diarrhea (Goldman-Cecil, 2024)
Step 7 - Antibiotic Therapy
When to use antibiotics:
- Moderate-severe febrile diarrhea
- Bloody diarrhea (invasive pathogen confirmed or suspected - except EHEC)
- Traveler's diarrhea
- Immunocompromised patients (treat regardless of identified organism)
- Mechanical heart valves, recent vascular grafts, elderly
Empiric Regimens
| Indication | First-line | Alternative |
|---|---|---|
| Adults - general | Azithromycin 500 mg single dose or 500 mg/day x 3 days | Ciprofloxacin 500 mg q12h x 3-5 days |
| Traveler's diarrhea (noninvasive) | Rifaximin 200 mg TID x 3 days | Azithromycin 1000 mg single dose |
| Traveler's diarrhea (invasive/febrile) | Azithromycin (fluoroquinolone resistance is common in SE Asia) | Ciprofloxacin 500 mg q12h x 3 days (where resistance is low) |
| Suspected Giardia | Metronidazole 250 mg QID x 7 days | Nitazoxanide 500 mg bid x 3 days |
| Children - traveler's | Azithromycin 10 mg/kg (max 500 mg) single dose | - |
Pathogen-Specific Antibiotic Choices
| Pathogen | Treatment | Key Notes |
|---|---|---|
| Salmonella (non-typhoidal) | Usually self-limited; no routine antibiotics - prolongs excretion | Treat high-risk: infants <3 mo, immunocompromised, hemoglobinopathy, invasive disease → Ceftriaxone or Ciprofloxacin |
| Typhoid fever (S. Typhi) | Ceftriaxone 50-75 mg/kg/day OR Ciprofloxacin x 10-14 days | Multidrug resistance is common; check susceptibilities; Dexamethasone for delirium/shock |
| Shigella | Azithromycin 20 mg/kg/day (max 500 mg) | Ceftriaxone if unable to take oral; TMP-SMX/ampicillin often resistant |
| Campylobacter | Azithromycin 500 mg/day x 3 days | Can cause Guillain-Barré syndrome (ascending paralysis post-gastroenteritis) |
| EHEC (E. coli O157:H7) | NO ANTIBIOTICS - increases HUS risk | NO loperamide either; supportive care only |
| C. difficile | Stop offending antibiotic; Vancomycin PO or Fidaxomicin | Metronidazole for mild disease |
| Vibrio cholerae | ORS (massive losses); Doxycycline or Azithromycin single dose | IV rehydration often needed given massive secretory losses |
| Giardia | Metronidazole 250 mg QID x 7 days | Nitazoxanide as alternative |
| Cryptosporidium | Nitazoxanide 500 mg bid x 3 days | Immunocompromised: difficult to treat |
| E. histolytica (amebic dysentery) | Metronidazole + Paromomycin (to clear cysts) | Associated with liver abscesses |
Step 8 - When Diarrhea Persists (>7-14 days)
If diarrhea persists after initial evaluation/treatment:
- Reconsider stool studies: Giardia is the most common cause of persistent diarrhea
- Rule out C. difficile (especially if antibiotics recently given)
- Consider Cryptosporidium, Campylobacter, E. histolytica
- If >30 days (chronic): sigmoidoscopy/colonoscopy with biopsies and upper endoscopy with duodenal aspirates may be needed to exclude celiac disease, Crohn's disease, or microscopic colitis (do NOT scope during or immediately after acute enteritis - false positives)
Special Populations
| Population | Key Modifications |
|---|---|
| Infants/children | ORS is critical; zinc supplementation (resource-limited settings); Azithromycin preferred over fluoroquinolones; AVOID loperamide in young children |
| Elderly ≥70 years | High risk for dehydration and systemic spread; lower threshold for antibiotics and IV fluids |
| Immunocompromised | Always treat with antibiotics even without identified pathogen; consider broader workup including CMV |
| Pregnant | Azithromycin preferred; avoid fluoroquinolones; avoid bismuth subsalicylate |
| Traveler's diarrhea | Rifaximin first-line if noninvasive (not absorbed); Azithromycin if febrile/invasive; avoid TMP-SMX (widespread resistance) |
High-Yield "Avoid" Summary (Exam Favorite)
| Drug | Avoid When | Reason |
|---|---|---|
| Loperamide | EHEC, Shigella, febrile dysentery, bloody stools | Prolongs organism clearance; increases HUS risk with EHEC |
| Antibiotics | EHEC O157:H7 | Triggers Shiga toxin release → HUS |
| Bismuth subsalicylate | Immunocompromised, renal impairment, children | Encephalopathy risk; Reye syndrome risk |
| TMP-SMX | Traveler's diarrhea (empiric) | Widespread global resistance |
| Rifaximin | Invasive/febrile traveler's diarrhea | Not absorbed; no systemic activity |
Sources: Harrison's Principles of Internal Medicine 22e, Ch. 49; Goldman-Cecil Medicine (International Ed.); Goodman & Gilman's Pharmacological Basis of Therapeutics; Rosen's Emergency Medicine (Treatment of infectious diarrhea in children); Frameworks for Internal Medicine
Recent guideline note: A 2025 Chinese Pediatric Practice Guideline (PMID 40437180) for acute infectious diarrhea in children reinforces ORS as first-line with selective antibiotic use - consistent with current international standards.
This is a shared conversation. Sign in to Orris to start your own chat.