How to describe galucomaflecken in case presentation for ophthalmologist
glaukomflecken clinical description case presentation ophthalmology slit lamp
Describing Glaukomflecken in an Ophthalmology Case Presentation
Standard Slit-Lamp Description Template
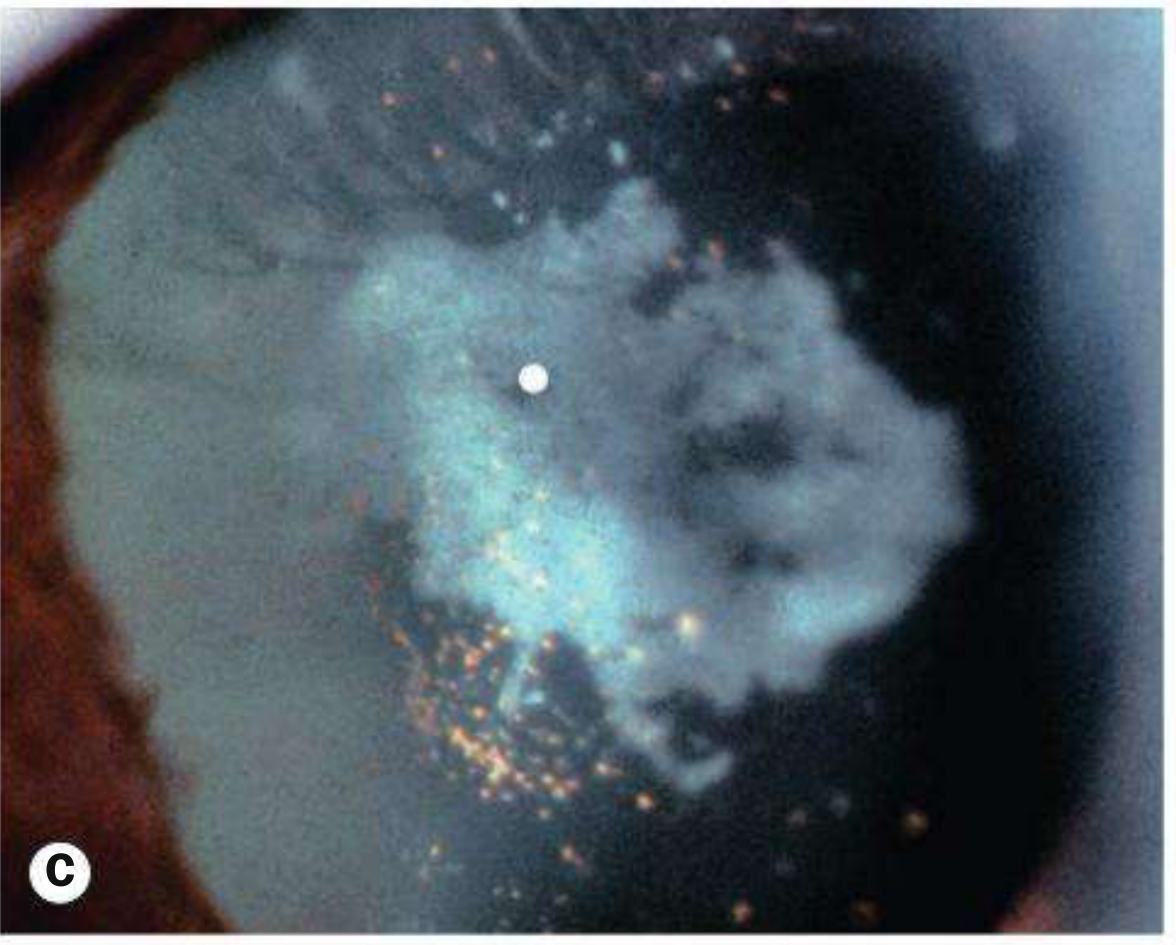
"On slit-lamp examination of the [right/left] eye, there are multiple small, discrete, grey-white anterior subcapsular/capsular opacities scattered within the pupillary zone, consistent with glaukomflecken. These represent focal infarcts of the lens epithelium and are pathognomonic of a prior episode of acute congestive angle closure."
Breaking Down Each Element
| Descriptor | What to Say | Why It Matters |
|---|---|---|
| Location | Anterior subcapsular or capsular | Distinguishes from PSC or nuclear cataract |
| Distribution | Within (confined to) the pupillary area | The dilated pupil during an acute attack exposes this zone to maximum IOP stress |
| Size | Small, discrete | Each is a focal infarct, not a confluent opacity |
| Colour | Grey-white (may appear white/chalky) | Necrosis of lens epithelium |
| Number | Multiple / scattered / few | Degree reflects severity of the prior attack |
| Associated signs | Iris stromal atrophy, irregular/dilated pupil, spiral-shaped iris atrophy, posterior synechiae | Markers of prior ischaemic APAC |
Example Full Lens Presentation Sentence
"The anterior segment examination revealed a shallow anterior chamber. The lens showed multiple small grey-white fleck-like opacities at the anterior subcapsule within the pupillary area - glaukomflecken - along with patchy iris stromal atrophy and an irregular dilated pupil, all consistent with sequelae of a prior acute primary angle closure episode."
Pathognomonic Significance - What to State
"These represent focal infarcts of the lens epithelium and are pathognomonic of previous acute congestive angle closure."
- They confirm a prior APAC attack even if the patient gives no clear history
- They help differentiate the etiology of any co-existing cataract
- They raise the question of fellow eye risk and prophylactic laser iridotomy
When Found at Resolved APAC (Late Signs)
- Glaukomflecken - white foci of necrosis in the superficial lens
- Spiral-shaped iris atrophy
- Irregular or fixed dilated pupil (iris sphincter/dilator damage)
- Posterior synechiae
- Optic nerve - normal or showing pallor and/or cupping
Reference Slit-Lamp Image (Kanski's Clinical Ophthalmology, Fig. 10.5C)
Quick Clinical Pearl
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed., p. 326
- The Wills Eye Manual, relevant section on Acute Angle Closure Glaucoma
For how many years it may persist
glaukomflecken how long persist permanent lens opacity duration
Why They Are Permanent
- The lens is avascular, so there are no macrophages or immune cells to clear the debris
- New epithelial cells that form around them do not displace or dissolve the necrotic foci
- The opacities therefore remain stationary and permanent at the layer of the anterior capsule/subcapsule
Clinical Implication for Case Presentation
"The presence of glaukomflecken indicates a prior episode of acute primary angle closure, which may have occurred months to years ago, even if the patient does not recall a distinct attack."
One Caveat
How to represent a surgical iridectomy while drawing gonioscopic findings of chronic angle closure glaucoma
gonioscopy diagram drawing notation surgical iridectomy peripheral iridotomy representation
https://eyewiki.org/Gonioscopy
gonioscopy clock diagram how to draw peripheral iridectomy "V-shaped" OR "notch" documentation chronic angle closure
Representing Surgical Iridectomy on a Gonioscopy Diagram
The Standard Diagram Format
Outer ring → Cornea / Schwalbe's line
Next ring → Trabecular meshwork (TM)
Next ring → Scleral spur
Inner ring → Ciliary body band
Innermost → Iris root / iris
How to Draw a Surgical Iridectomy
| Feature | How to Draw It |
|---|---|
| Shape | A V-shaped or U-shaped notch cut into the iris ring at the periphery |
| Location | At the 12 o'clock position (most surgical PIs are placed superotemporally, covered by the lid) |
| Depth | The notch reaches through the full thickness of the iris band on the diagram |
| Width | Drawn wider than a laser PI (which is a tiny dot/pinhole) |
| Label | Write "PI" or "surgical PI" or "iridectomy" with an arrow pointing to the notch |
Distinguishing Surgical PI from Laser PI on the Diagram
| Type | Drawn As | Notes |
|---|---|---|
| Surgical iridectomy | Wide V or U-shaped notch in the iris | Full-thickness, sector-shaped gap |
| Laser peripheral iridotomy (LPI) | Small dot or tiny gap (pinhole) in the iris | Much smaller than surgical |
| Sector iridectomy | Large wedge-shaped defect | Occupies a wider arc |
For Chronic Angle Closure - What to Show on the Same Diagram
- Narrow or closed angle - shade or hatch the TM ring in the affected quadrants to indicate iridotrabecular contact (ITC)
- PAS (Peripheral Anterior Synechiae) - drawn as tent-like or tooth-like projections of the iris reaching up to or beyond the scleral spur / TM, shaded differently (often in red or hatched)
- Surgical iridectomy - the V-notch in the iris ring at the clock position where it sits
- Pigmentation - dot or shade the TM to indicate degree (0-4+ by Shaffer)
- Angle grade - note the Shaffer or Scheie grade per quadrant
ASCII Representation of the Concept
12 o'clock
___V___ ← V = iridectomy notch in iris ring
/ | | \
9 | TM TM | 3
| /// \\ | ← hatching = PAS / closed angle
\_____________/
6
Practical Tips for Case Presentation
- Always label the clock position (e.g., "surgical PI at 11 o'clock")
- Note whether the iridectomy is patent (visible light reflex through it on slit lamp) - this is important and should be mentioned in your verbal description alongside the diagram
- In CACG with PAS, mark the extent of PAS in clock hours (e.g., "PAS from 10 to 2 o'clock, superior 4 clock hours") - this directly guides prognosis and surgical planning
- The EyeWiki gonioscopy article shows a real gonioscopic photo with both a trabeculectomy ostium and peripheral iridectomy visible simultaneously in the superior angle - a useful reference image
Draw a diagram of this findings
A clean medical ophthalmology gonioscopy clock-face diagram showing chronic angle closure glaucoma with surgical peripheral iridectomy findings. The diagram is a circular concentric ring drawing viewed from above (like a target/bullseye), oriented with 12 o'clock at top, 3 o'clock right, 6 o'clock bottom, 9 o'clock left. Clock hour numbers 1-12 are labeled around the outer edge. From outside to inside, the concentric rings are clearly labeled: 1. Outermost ring: "Schwalbe's Line" (thin white line) 2. Next ring: "Trabecular Meshwork" (lightly pigmented, stippled gray) 3. Next ring: "Scleral Spur" (thin white line) 4. Next ring: "Ciliary Body Band" (light gray band) 5. Innermost ring: "Iris Root" (brown/tan colored) 6. Center circle: "Pupil" (black circle) Key findings drawn on the diagram: - At 12 o'clock position on the iris ring: a clear wide V-shaped notch or gap cut into the iris, labeled "Surgical PI" with a small arrow pointing to it. The notch is wide and obvious, distinguishable as a surgical iridectomy. - In the superior quadrant (10 o'clock to 2 o'clock arc): the trabecular meshwork ring is heavily shaded/hatched in dark gray/red to indicate peripheral anterior synechiae (PAS), with small tent-like projections of iris tissue reaching up to the trabecular meshwork, labeled "PAS" with arrows. - In the inferior quadrant (4 to 8 o'clock): the angle is narrow but open, TM lightly pigmented, labeled "Narrow angle (Shaffer Grade I-II)". - Nasal and temporal quadrants show moderate narrowing with some ITC (iridotrabecular contact), lightly shaded. - A small legend box in the corner showing: dark hatching = PAS/synechial closure, light stipple = pigmented TM, V-notch = surgical iridectomy. - Title at top: "Gonioscopy Diagram - Chronic Angle Closure Glaucoma" - Clean white background, professional medical illustration style, clearly readable labels with leader lines.
mkdir -p /tmp/workspace/gonioscopy && python3 << 'EOF' import matplotlib.pyplot as plt import matplotlib.patches as mpatches from matplotlib.patches import Arc, FancyArrowPatch, Wedge, Circle import numpy as np fig, ax = plt.subplots(1, 1, figsize=(10, 10)) ax.set_xlim(-1.6, 1.6) ax.set_ylim(-1.6, 1.6) ax.set_aspect('equal') ax.axis('off') ax.set_facecolor('white') fig.patch.set_facecolor('white') # ---------- concentric rings (radii) ---------- r_schwalbe = 1.30 r_tm_outer = 1.20 r_tm_inner = 1.00 r_scleral = 0.95 r_cb_inner = 0.78 r_iris_outer = 0.72 r_iris_inner = 0.52 r_pupil = 0.30 # Helper: draw a filled annulus sector def annulus_sector(ax, r_out, r_in, theta1, theta2, color, alpha=1.0, zorder=2): theta = np.linspace(np.radians(theta1), np.radians(theta2), 200) xs = np.concatenate([r_out*np.cos(theta), r_in*np.cos(theta[::-1])]) ys = np.concatenate([r_out*np.sin(theta), r_in*np.sin(theta[::-1])]) ax.fill(xs, ys, color=color, alpha=alpha, zorder=zorder) # ---------- 1. Schwalbe's line (outermost thin ring) ---------- schwalbe_ring = Circle((0,0), r_schwalbe, fill=False, edgecolor='navy', linewidth=2.5, zorder=3) ax.add_patch(schwalbe_ring) # ---------- 2. Trabecular Meshwork ring (full 360, light grey base) ---------- annulus_sector(ax, r_tm_outer, r_tm_inner, 0, 360, '#c8b89a', alpha=0.6, zorder=2) # TM pigmentation - heavier inferiorly (normal) annulus_sector(ax, r_tm_outer, r_tm_inner, 240, 300, '#7a5c3a', alpha=0.55, zorder=3) # inferior heavy pigment # PAS in superior quadrant 300-420 deg (i.e. 300->360 and 0->60, = 10 o'clock to 2 o'clock) # Draw as darker reddish-brown hatched wedge for offset in np.arange(0, 1.0, 0.07): annulus_sector(ax, r_tm_outer+0.005, r_iris_outer, 300+offset*8, 300+offset*8+5, '#8B1A1A', alpha=0.75, zorder=4) annulus_sector(ax, r_tm_outer, r_iris_outer, 300, 420, '#c0392b', alpha=0.28, zorder=4) # PAS tooth projections - small triangles pointing outward from iris into TM for ang_deg in [310, 325, 340, 355, 10, 25, 40, 55]: ang = np.radians(ang_deg) tip_r = r_tm_inner + 0.12 base_r = r_iris_outer + 0.01 d = np.radians(4) tip = (tip_r*np.cos(ang), tip_r*np.sin(ang)) bl = (base_r*np.cos(ang-d), base_r*np.sin(ang-d)) br = (base_r*np.cos(ang+d), base_r*np.sin(ang+d)) ax.fill([tip[0], bl[0], br[0]], [tip[1], bl[1], br[1]], color='#8B1A1A', alpha=0.85, zorder=5) # ---------- 3. Scleral spur line ---------- scleral_ring = Circle((0,0), r_scleral, fill=False, edgecolor='#555555', linewidth=1.8, linestyle='--', zorder=3) ax.add_patch(scleral_ring) # ---------- 4. Ciliary body band ---------- annulus_sector(ax, r_cb_inner+0.06, r_cb_inner, 0, 360, '#b5cfa8', alpha=0.7, zorder=2) # ---------- 5. Iris ring (full, brown) ---------- annulus_sector(ax, r_iris_outer, r_iris_inner, 0, 360, '#8B6914', alpha=0.85, zorder=2) # Narrow angle shading: nasal & temporal - overlay slightly lighter to show appositional ITC for region in [(60, 120), (240, 300)]: annulus_sector(ax, r_tm_inner+0.02, r_iris_outer, region[0], region[1], '#d4a017', alpha=0.30, zorder=3) # ---------- 6. Surgical PI at 12 o'clock (90 deg in math convention) ---------- # Cut a notch out of the iris ring at 90 deg (top) notch_half = np.radians(9) # width of notch notch_ang = np.radians(90) # Redraw iris WITHOUT the notch region by drawing two arcs annulus_sector(ax, r_iris_outer+0.01, r_iris_inner-0.01, 99, 441, # 99 to 441 = full circle minus 90±9 'white', alpha=1.0, zorder=6) # left side of iris (notch excluded) annulus_sector(ax, r_iris_outer, r_iris_inner, 99, 360+81, '#8B6914', alpha=0.85, zorder=6) # Fill notch with dark (through-and-through gap) theta_notch = np.linspace(notch_ang - notch_half, notch_ang + notch_half, 60) xs_out = r_iris_outer * np.cos(theta_notch) ys_out = r_iris_outer * np.sin(theta_notch) xs_in = r_iris_inner * np.cos(theta_notch[::-1]) ys_in = r_iris_inner * np.sin(theta_notch[::-1]) ax.fill(np.concatenate([xs_out, xs_in]), np.concatenate([ys_out, ys_in]), color='#1a1a2e', alpha=0.9, zorder=7) # V-notch visual marker mid = np.radians(90) tip_x, tip_y = (r_iris_inner+0.04)*np.cos(mid), (r_iris_inner+0.04)*np.sin(mid) ax.plot([r_iris_outer*np.cos(mid-notch_half), tip_x, r_iris_outer*np.cos(mid+notch_half)], [r_iris_outer*np.sin(mid-notch_half), tip_y, r_iris_outer*np.sin(mid+notch_half)], color='black', linewidth=2.5, zorder=8) # ---------- 7. Pupil ---------- pupil = Circle((0,0), r_pupil, color='black', zorder=5) ax.add_patch(pupil) # ---------- Clock numbers ---------- for hr in range(1, 13): angle_deg = 90 - hr * 30 # 12 o'clock = 90 deg angle_rad = np.radians(angle_deg) r_label = 1.48 x = r_label * np.cos(angle_rad) y = r_label * np.sin(angle_rad) ax.text(x, y, str(hr), ha='center', va='center', fontsize=11, fontweight='bold', color='#222222') # ---------- Structural labels ---------- label_params = dict(fontsize=8.5, color='#1a1a2e', ha='center', bbox=dict(boxstyle='round,pad=0.2', fc='white', ec='none', alpha=0.8)) ax.text(0, r_schwalbe+0.12, "Schwalbe's Line", **label_params) ax.annotate("", xy=(0.72, r_schwalbe), xytext=(0.72, r_schwalbe+0.09), arrowprops=dict(arrowstyle='->', color='navy', lw=1.2)) ax.text(-1.55, 0.22, "Trabecular\nMeshwork", fontsize=8, color='#5a3e1b', ha='center', bbox=dict(boxstyle='round,pad=0.2', fc='white', ec='none', alpha=0.8)) ax.annotate("", xy=(-r_tm_outer+0.05, 0.12), xytext=(-1.38, 0.18), arrowprops=dict(arrowstyle='->', color='#5a3e1b', lw=1.2)) ax.text(1.55, -0.18, "Scleral\nSpur", fontsize=8, color='#444', ha='center', bbox=dict(boxstyle='round,pad=0.2', fc='white', ec='none', alpha=0.8)) ax.annotate("", xy=(r_scleral*np.cos(np.radians(-10)), r_scleral*np.sin(np.radians(-10))), xytext=(1.35, -0.16), arrowprops=dict(arrowstyle='->', color='#444', lw=1.2)) ax.text(-1.50, -0.30, "Ciliary Body\nBand", fontsize=8, color='#4a7040', ha='center', bbox=dict(boxstyle='round,pad=0.2', fc='white', ec='none', alpha=0.8)) ax.annotate("", xy=(-r_cb_inner*np.cos(np.radians(20)), -r_cb_inner*np.sin(np.radians(20))), xytext=(-1.30, -0.30), arrowprops=dict(arrowstyle='->', color='#4a7040', lw=1.2)) ax.text(1.52, 0.35, "Iris Root", fontsize=8, color='#6b4f10', ha='center', bbox=dict(boxstyle='round,pad=0.2', fc='white', ec='none', alpha=0.8)) ax.annotate("", xy=(r_iris_outer*np.cos(np.radians(15)), r_iris_outer*np.sin(np.radians(15))), xytext=(1.32, 0.32), arrowprops=dict(arrowstyle='->', color='#6b4f10', lw=1.2)) # Surgical PI label ax.annotate("Surgical PI\n(12 o'clock)", xy=(0, r_iris_outer+0.06), xytext=(0.48, 1.15), fontsize=8.5, fontweight='bold', color='#1a1a2e', ha='center', bbox=dict(boxstyle='round,pad=0.3', fc='#fff9c4', ec='#888', alpha=0.95), arrowprops=dict(arrowstyle='->', color='#333', lw=1.3)) # PAS label ax.annotate("PAS\n(10–2 o'clock)\nSynechial closure", xy=(0.18, r_tm_inner+0.07), xytext=(0.85, 1.10), fontsize=8.5, fontweight='bold', color='#8B1A1A', ha='center', bbox=dict(boxstyle='round,pad=0.3', fc='#fdecea', ec='#c0392b', alpha=0.95), arrowprops=dict(arrowstyle='->', color='#c0392b', lw=1.3)) # Narrow angle label ax.annotate("Narrow angle\nITC (appositional)\nShaffer Grade I", xy=(-r_tm_inner-0.02, -0.55), xytext=(-1.35, -0.80), fontsize=8, color='#7a5200', ha='center', bbox=dict(boxstyle='round,pad=0.3', fc='#fff3cd', ec='#d4a017', alpha=0.95), arrowprops=dict(arrowstyle='->', color='#d4a017', lw=1.2)) # Heavy TM pigment label ax.annotate("Heavy TM\npigment (inf.)", xy=(0, -r_tm_inner-0.05), xytext=(0.75, -1.20), fontsize=8, color='#5a3e1b', ha='center', bbox=dict(boxstyle='round,pad=0.2', fc='#f5e6d0', ec='#7a5c3a', alpha=0.9), arrowprops=dict(arrowstyle='->', color='#7a5c3a', lw=1.2)) # ---------- Legend ---------- legend_x, legend_y = -1.55, -1.30 ax.add_patch(mpatches.Rectangle((legend_x-0.02, legend_y-0.28), 1.12, 0.60, fc='#f9f9f9', ec='#999', linewidth=1, zorder=9)) ax.fill_betweenx([legend_y+0.04, legend_y+0.18], [legend_x, legend_x], [legend_x+0.22, legend_x+0.22], color='#c0392b', alpha=0.5, zorder=10) ax.text(legend_x+0.27, legend_y+0.11, "PAS / synechial closure", fontsize=7.5, va='center', zorder=10) ax.fill_betweenx([legend_y-0.22, legend_y-0.08], [legend_x, legend_x], [legend_x+0.22, legend_x+0.22], color='#8B6914', alpha=0.85, zorder=10) ax.text(legend_x+0.27, legend_y-0.15, "Iris / surgical PI notch", fontsize=7.5, va='center', zorder=10) # ---------- Title ---------- ax.set_title("Gonioscopy Diagram\nChronic Angle Closure Glaucoma with Surgical Peripheral Iridectomy", fontsize=13, fontweight='bold', color='#1a1a2e', pad=14) plt.tight_layout() plt.savefig('/tmp/workspace/gonioscopy/gonioscopy_CACG.png', dpi=180, bbox_inches='tight', facecolor='white') print("Saved.") EOF
gonioscopy CACG
Image · PNG
Key findings represented on the diagram:
| Structure | What's Shown |
|---|---|
| Schwalbe's Line | Outermost navy ring |
| Trabecular Meshwork | Tan/beige annular band |
| Scleral Spur | Dashed ring (grey) |
| Ciliary Body Band | Light green band |
| Iris Root | Brown/gold ring |
| Pupil | Central black circle |
| Surgical PI | Dark V-shaped notch at 12 o'clock in the iris ring - wide and full-thickness, distinguishable from a laser PI |
| PAS (10-2 o'clock) | Red tent/tooth-shaped projections in the superior quadrant extending from iris into the TM, with red shading indicating synechial closure (~4 clock hours) |
| Narrow angle / ITC | Yellow overlay in nasal/inferior-nasal quadrant showing appositional iridotrabecular contact (Shaffer Grade I) |
| Heavy TM pigment | Darker brown shading inferiorly (normal finding, common in angle closure) |