Cochlear implants for ms ent pg level theory answer
Reading File
Finding Sources
Searching PubMed
"cochlear implant" indications outcomes
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Now I have everything needed for a thorough PG ENT-level answer. Here it is:
Cochlear Implants - MS ENT PG Level Theory
Sources: KJ Lee's Essential Otolaryngology, Cummings Otolaryngology Head & Neck Surgery, Scott-Brown's Otorhinolaryngology
Definition
A cochlear implant (CI) is a surgically implanted electronic device used for hearing rehabilitation of adults and children with advanced sensorineural hearing loss (SNHL) and/or poor speech discrimination who gain limited or no benefit from conventional hearing aids.
Basic Principle
The CI exploits the tonotopic arrangement of the cochlea: high-pitched sounds are processed by spiral ganglion cells at the basal turn, and low-pitched sounds by those at the apex. In normal hearing, ~35,000 auditory nerve fibres are present; at least 10,000 functional fibres are estimated to be required for speech recognition using a CI.
The device bypasses the non-functional outer/inner hair cells and delivers direct electrical stimulation to the residual spiral ganglion cells (located in Rosenthal's canal), which propagate signals along the auditory nerve to the brain.
Components of the CI System
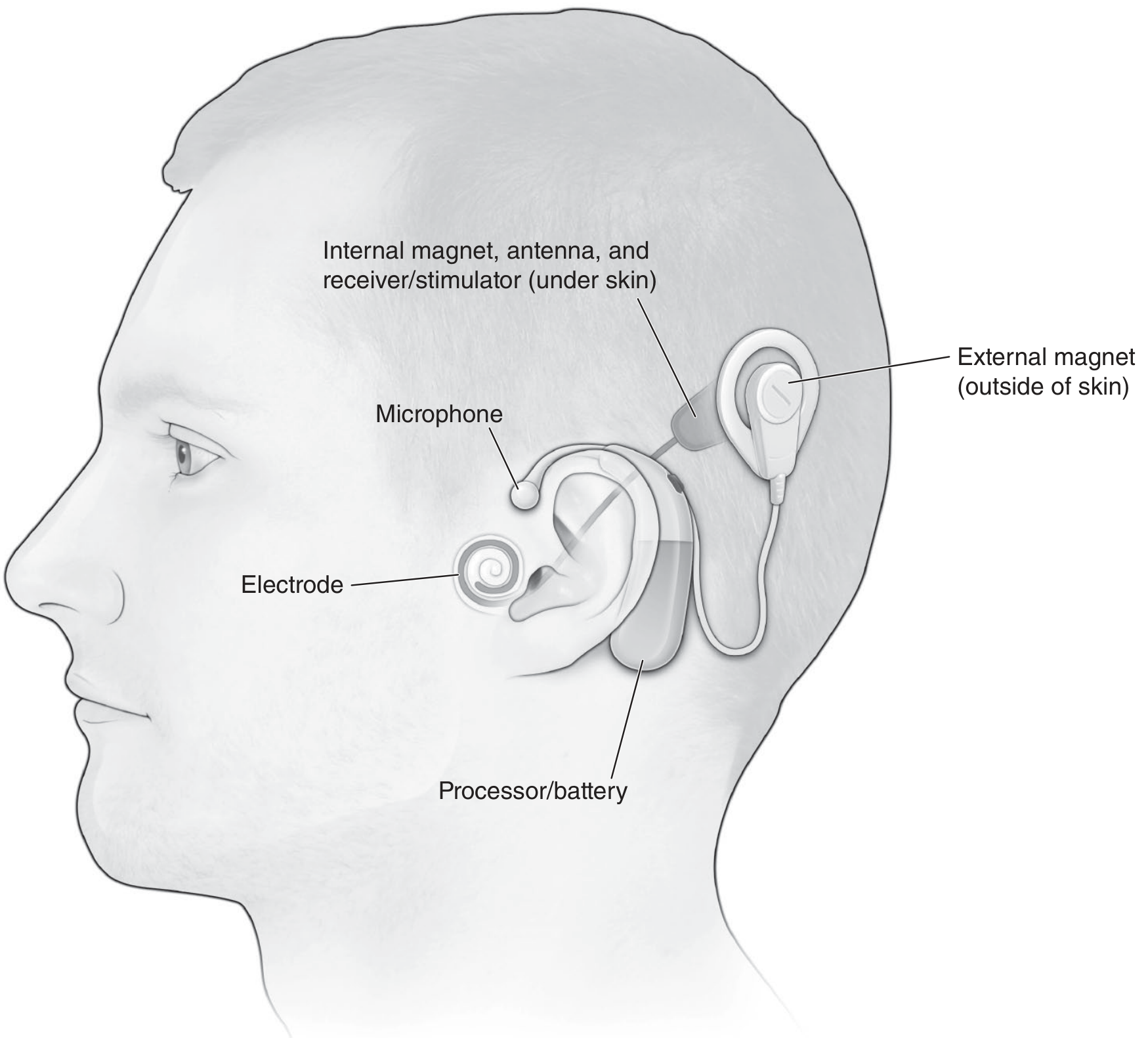
External Components
| Component | Function |
|---|---|
| Microphone | Placed near the earhook; receives natural acoustic information and converts it to an analog electrical signal |
| Sound Processor | Amplifies, compresses, and filters the signal; digitizes via Fourier analysis to convey timing, frequency, and intensity information to the CNS |
| RF Transmitter Antenna | Sends the processed signal transcutaneously to the implanted receiver-stimulator |
| External Magnet | Aligns with the internal magnet to facilitate transcutaneous RF signal transmission |
| Battery | Powers the external unit |
Internal Components
| Component | Function |
|---|---|
| Internal Magnet | Holds the external coil in alignment |
| Internal RF Antenna | Receives the transcutaneous signal |
| Receiver/Stimulator | Translates the electrical signal into rapid electrical impulses distributed to individual wires within the electrode array |
| Electrode Array | Placed within the scala tympani; stimulates spiral ganglion cells in Rosenthal's canal |
Speech Processing Strategies
Continuous Interleaved Sampling (CIS) - the most common strategy used. It minimizes channel interaction by presenting non-simultaneous (interleaved) brief, rapid impulses across the electrode array, better representing the tonotopic organization of the cochlea.
Other strategies include ACE (Advanced Combination Encoder), FSP (Fine Structure Processing), and HiRes.
Electrode Arrays
- Number of electrodes: MED-EL - 12 electrodes; Advanced Bionics - 16 electrodes; Cochlear (Nucleus) - 22 electrodes
- Despite the number, most users have fewer than 10 perceptually unique channels active at any one time
- Modern electrodes are shorter, thinner, and more flexible to minimize insertion trauma and preserve residual hearing
Candidacy Criteria (FDA-Based)
Pediatric Candidacy
| Age Group | Hearing Threshold | Additional Criteria |
|---|---|---|
| 12-23 months | Profound SNHL (>90 dB HL) | Limited benefit from HA trial; failure to reach auditory milestones |
| >2 years (up to 17 years) | Severe to profound SNHL (>70 dB HL) | Word recognition <20-30% on MLNT/LNT; limited HA benefit |
- Children 2-17 years: Moderate to profound SNHL (>40 dB) with sentence recognition ≤50% in the ear to be implanted and ≤60% in the contralateral ear (or ≤40% by CMS criteria)
- Special circumstances (e.g., post-meningitis with risk of cochlear ossification) may warrant implantation before 12 months (off-label)
- Off-label implantation <12 months is increasingly common - studies show language comprehension and expressive development comparable to normal hearing children
Adult Candidacy
| Criteria | Details |
|---|---|
| Hearing threshold | Profound SNHL (>90 dB HL) bilaterally |
| Speech recognition | Limited benefit from HA - based on MAIS (Meaningful Auditory Integration Scale) |
| Open-set testing | CNC word score ≤50% in the ear to be implanted; ≤60% contralaterally or binaurally |
| Age | No upper age limit; outcomes are good even in 65-80 year age group |
Non-Traditional / Expanding Indications
- Single-sided deafness (SSD)
- Retrocochlear hearing loss
- Asymmetrical SNHL
- Auditory Neuropathy Spectrum Disorder (ANSD)
Electroacoustic Stimulation (EAS) / Cochlear Nucleus Hybrid System
For candidates with residual low-frequency hearing (thresholds ≤60 dB HL at frequencies up to 500 Hz) but severe to profound high-frequency loss (PTA at 2, 3, 4 kHz ≥75 dB HL):
- Shortened electrode arrays (20 mm for MED-EL; 10 mm for Nucleus Hybrid) are inserted via the round window to preserve low-frequency residual hearing
- Combined electric (basal cochlea) + acoustic (apical cochlea) stimulation provides better outcomes than conventional CI alone
- FDA criteria: aided CNC word recognition score 10%-60% in the ear to be implanted; contralateral ear score equal to or better but ≤80%
Pre-operative Assessment
Medical Assessment
- Determine etiology of hearing loss (affects prognosis)
- Screen for factors causing cochlear ossification: meningitis, temporal bone fracture, otosclerosis
- Duration of deafness: longer duration predicts poorer outcomes
- Chronic otitis media: may require staged surgery (treat COM first, then CI)
- Recurrent AOM should not unduly delay implantation in children
Audiometric Assessment
- Children: OAE, ABR, behavioral audiometry, parental questionnaires (IT-MAIS), minimum 3-month HA trial
- Adults: AzBio sentences, CNC monosyllabic word testing, BKB-SIN (Bamford-Kowal-Bench Speech-in-Noise)
- ANSD evaluation: requires ear-specific data; MRI to rule out cochlear nerve deficiency (CND)
Radiologic Assessment
MRI (preferred):
- Gold standard for cochlear patency (distinguishes fluid vs. fibrosis vs. ossification)
- Superior for visualizing the cochlear nerve (heavily T2-weighted - CISS or FIESTA sequences, sagittal plane)
- Identifies retrocochlear pathology (e.g., vestibular schwannoma)
- Should be done pre-operatively as last opportunity for high-quality brain imaging without artifact
HRCT Temporal Bone:
- Diagnoses bony cochlear malformations
- Evaluates bony cochlear nerve canal (BCNC) in cases of narrow IAC (<3 mm)
- Identifies surgical obstacles: poorly pneumatized mastoid, anterior sigmoid sinus, high-riding jugular bulb, aberrant facial nerve course
- Risk of CSF gusher in: thin cribriform area, widened IAC, enlarged vestibular aqueduct, IP3 deformity
Contraindications
Absolute:
- Absence/aplasia of the cochlear nerve (cochlear nerve deficiency)
- Complete cochlear ossification (relative - partial insertion may still be possible)
- Active middle ear infection
Relative:
- Severe cognitive impairment
- Significant medical comorbidity precluding general anesthesia
- Unrealistic patient/family expectations
- Lack of adequate rehabilitation support
The CI Team (Multidisciplinary)
Core team: ENT surgeon, audiologist, speech and language pathologist
Additional members: Educational specialist, psychologist, social worker, early interventionist, educational audiologist, deaf/hard-of-hearing itinerant teacher
For children with complex needs: physical therapist, occupational therapist, behavioral interventionist, developmental pediatrician
Surgical Approach
The standard approach is mastoidectomy and posterior tympanotomy (facial recess approach):
- Cortical mastoidectomy
- Posterior tympanotomy (via the facial recess, between the facial nerve and chorda tympani)
- Cochleostomy or round window membrane approach into scala tympani
- Electrode array insertion
- Receiver-stimulator placed in a bony well posterior to the mastoid
Round window approach is preferred to minimize insertion trauma and preserve residual hearing (especially for EAS candidates).
Bilateral Cochlear Implantation
Options: Simultaneous bilateral CI vs. sequential bilateral CI (separate procedures)
Benefits of binaural hearing:
- Binaural summation (improved SNR)
- Directional hearing / sound localization
- Better speech in noise performance
- Benefit for visually impaired patients
- Incidental/background learning through listening
- Logistical benefit: one device remains functional if the other fails
Key principle: Decreasing the inter-device interval (time between two CIs) is strongly beneficial - CNS evidence of binaural integration is seen with intervals under 1 year.
Activation and Programming ("Mapping")
- Begins 3-4 weeks post-surgery
- Impedance testing at each visit to check electrode functionality
- Programming involves setting T-levels (threshold/detection) and M/C-levels (maximum comfort)
- Electrophysiologic aids: eCAP (electrically evoked compound action potential) and eSRT (electrically evoked stapedial reflex threshold) - useful when behavioral responses are unreliable in infants
Outcomes
Adults
- Primary goal: improved open-set speech perception
- Mean open-set word recognition (CNC): 25-55% at >6 months
- With modern processing strategies: mean sentence recognition >80% (range up to 100%)
- Continued improvement up to 3 years post-implantation; smaller improvements beyond 3 years
- Telephone speech recognition and music appreciation occasionally reported
- Multichannel implants clearly superior to single-channel designs
Children
- Earlier implantation = better language outcomes
- CI before 12 months: language comprehension and expressive development comparable to normal hearing peers
- Auditory training post-CI further improves outcomes
Factors Predicting Better Outcomes
- Shorter duration of deafness
- Postlingual (vs. prelingual) onset of deafness
- Younger age at implantation
- Higher pre-implant residual hearing
- Good cognitive function
- Active rehabilitation and family involvement
Factors Predicting Poorer Outcomes
- Long-standing profound deafness
- Cochlear ossification/malformation
- Cochlear nerve deficiency
- Significant neurodevelopmental comorbidities
Post-implant Complications
| Level | Finding | Management |
|---|---|---|
| I | Skin erythema within antenna disc (intact) | Magnet rest; reduce magnet strength |
| II | Erythema extending beyond disc with tenderness/swelling | Discontinue use; oral antibiotics; monitor |
| III | Wound dehiscence, device exposed, no infection signs | Urgent surgical washout and wound revision |
| IV | Fluctuation or dehiscence (device not exposed) | IV antibiotics; consider operative drainage; if unresolved, explant leaving intracochlear electrode |
| V | Dehiscence with device exposed + purulent drainage | Urgent explant; IV antibiotics |
Other complications: facial nerve injury, CSF gusher, meningitis, device failure, tinnitus, vestibular disturbance
Special Considerations in CI Patients
Meningitis Risk
- CI recipients are at higher risk for meningitis after AOM
- No observation period permitted for AOM in CI patients (unlike standard children)
- AOM <2 months after surgery: parenteral antibiotics
- AOM >2 months after surgery: high-dose amoxicillin-clavulanate
- Suspected meningitis: LP with CSF culture
Vaccination (Mandatory Pre-/Post-implantation)
Children:
- PCV13 at least 2 weeks prior to implantation
- Children 6-18 years: single dose PCV13 regardless of prior history
- Children >2 years: PPSV23 after completing PCV13 series
Adults:
- Single dose PCV13 followed by PPSV23 at least 8 weeks later
- Second dose PPSV23 for CI recipients >65 years
Tympanostomy Tubes in CI Patients
- CIs can safely coexist with PE tubes
- Children susceptible to RAOM may keep PE tubes without placing CI or patient at undue risk
- Replacement of PE tubes after CI is acceptable for treatment of RAOM
- If history of recurrent AOM: consider subtotal petrosectomy with ET ablation and EAC closure with second-stage CI
MRI Safety
- Modern CI devices are MRI-conditional (typically up to 1.5 T with precautions)
- Pre-implant MRI should be obtained as this is the last opportunity for high-quality brain imaging without artifact
Auditory Neuropathy Spectrum Disorder (ANSD) and CI
- Defined by: cochlear microphonic (wave I) present + distal ABR waveforms absent ± OAEs present
- Cannot predict hearing thresholds by electrophysiology alone
- Worse discrimination scores than expected from thresholds
- Stepwise approach: observation → hearing thresholds + discrimination → amplification or alternate communication → CI if severe/profound range
- MRI mandatory to rule out cochlear nerve deficiency before CI in ANSD
- IT-MAIS used for candidacy evaluation in young children with ANSD
KJ Lee's Essential Otolaryngology, pp. 406-410 | Cummings Otolaryngology Head & Neck Surgery, pp. 3072-3726 | Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 2, pp. 1201-1202
This is a shared conversation. Sign in to Orris to start your own chat.