Methanol posiong
Reading File
Finding Sources
Finding Sources
Searching PubMed
"methanol poisoning" AND treatment
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive information to provide a thorough, well-sourced answer.
Methanol Poisoning
Overview
Methanol (CH₃OH), also called methyl alcohol or wood alcohol, is found in paint removers, shellac, antifreeze, and industrial solvents. It is also added to industrial ethanol to make it unfit for drinking. Ingestion of as little as 8 g (10 mL) can cause toxicity ranging from blindness to death.
- Goodman & Gilman's Pharmacological Basis of Therapeutics, p. 540
Pathophysiology & Metabolism
The key to understanding methanol toxicity is its metabolic pathway:
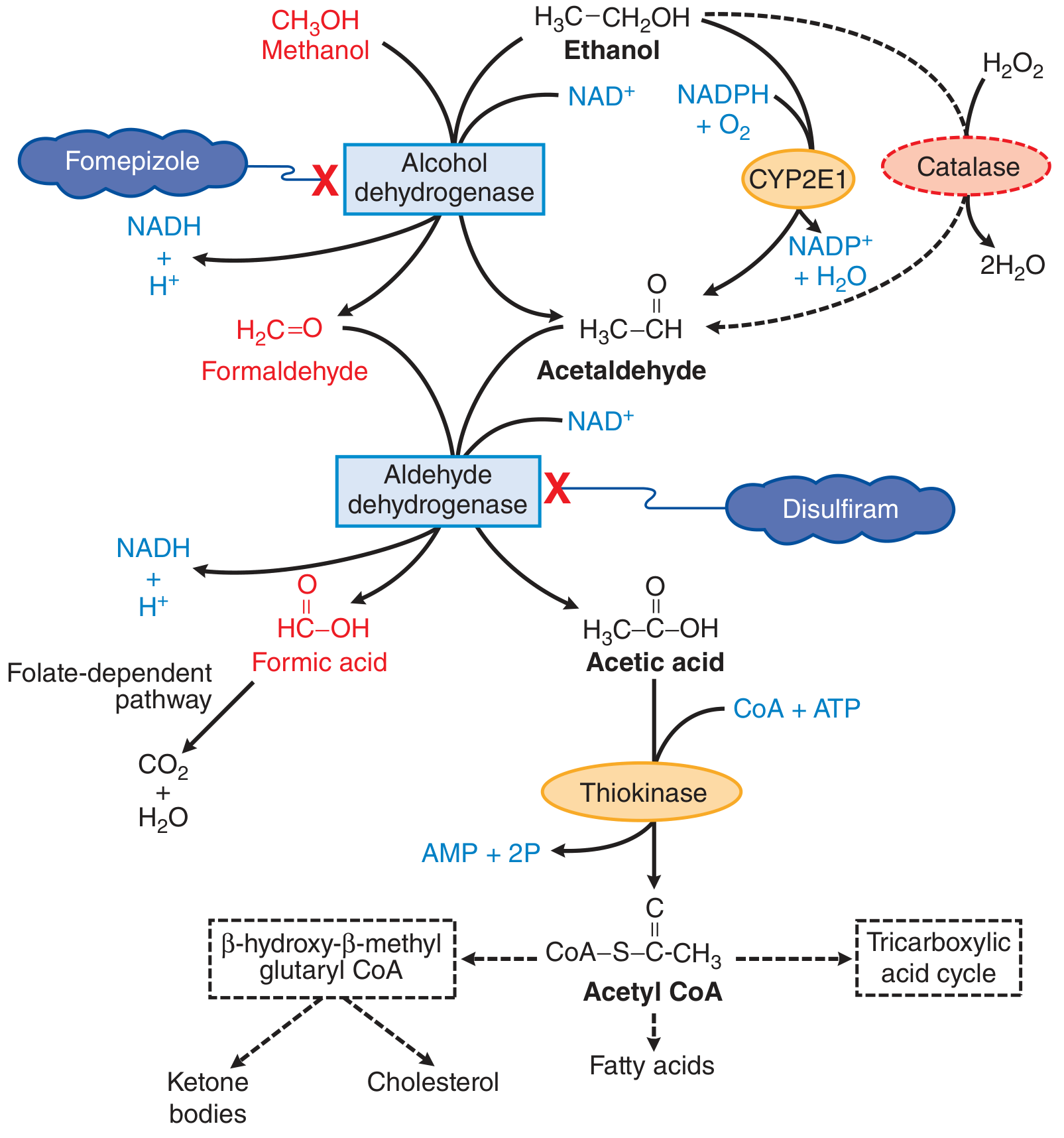
Figure: Metabolism of methanol (red). Fomepizole blocks alcohol dehydrogenase (ADH), preventing conversion to toxic metabolites.
- Methanol → Formaldehyde (via ADH)
- Formaldehyde → Formic acid (via ALDH)
- Formic acid is the main toxic agent -- it injures the optic nerve and retinal ganglion cells, and accumulates to cause severe anion gap metabolic acidosis
Methanol itself is only mildly toxic; the metabolites cause the damage. This explains the characteristic latent period of 12+ hours between ingestion and symptom onset.
- Goodman & Gilman's, p. 540
Clinical Presentation (Time Course)
| Time | Symptoms |
|---|---|
| 0-12 hours | Inebriation (like ethanol intoxication), asymptomatic period |
| 12-24 hours | Headache, nausea, vomiting, abdominal pain (pancreatitis) |
| 24-36 hours | Visual disturbances (blurred vision, "snowfield" vision), retinal edema progressing to blindness; seizures; severe metabolic acidosis |
| >48 hours | Putamen and white matter hemorrhage, Parkinson-like state, coma, death |
- Comprehensive Clinical Nephrology, 7th Ed., Box 13.6
Key features:
- Optic toxicity: Formic acid injures retinal ganglion cells and the optic nerve -- can cause permanent bilateral blindness
- Pancreatitis: GI pain is partially due to pancreatic necrosis
- Respiratory depression: Severe metabolic acidosis can lead to coma or death
Diagnosis
Two-gap approach -- the hallmark of methanol (and ethylene glycol) poisoning:
Early: Elevated Osmolar Gap
- Osmolar gap = Measured osmolality - Calculated osmolality (2[Na] + BUN/2.8 + glucose/18)
- Methanol is osmotically active before it is metabolized
- Osmolar gap >10 mOsm/kg is an important early clue
- As methanol is metabolized, the osmolar gap falls but the anion gap rises
Later: Elevated Anion Gap Metabolic Acidosis
- Formic acid accumulation drives a high anion gap
- Anion gap = Na - (Cl + HCO₃) ; normal ~12 mEq/L
- High anion gap + high osmolar gap simultaneously = strong indicator of toxic alcohol ingestion
Methanol level
-
Methanol level >20 mg/dL (>6 mmol/L) is diagnostic and an indication for treatment
-
Washington Manual of Medical Therapeutics, p. 1100; Goldman-Cecil Medicine
Treatment
1. Fomepizole (First-Line - Drug of Choice)
Fomepizole (4-methylpyrazole) is an ADH inhibitor -- it competitively blocks the enzyme that converts methanol to formaldehyde, halting toxic metabolite production.
Dosing:
- Loading dose: 15 mg/kg IV
- Maintenance: 10 mg/kg IV every 12 hours for 48 hours
- After 48 hours: increase to 15 mg/kg every 12 hours (fomepizole auto-induces its own metabolism)
- Increase frequency to every 4 hours during hemodialysis
- Continue until methanol level <20 mg/dL
Important: Fomepizole does NOT reverse existing acidosis or end-organ damage -- it only prevents further toxic metabolite formation.
2. Ethanol (Second-Line - Only if Fomepizole Unavailable)
Ethanol has >10-fold greater affinity for ADH than methanol, competitively displacing it. Target blood ethanol level of 100-200 mg/dL.
- IV loading dose: 0.6 g/kg, then 66 mg/kg/hour maintenance
- Significantly harder to dose and titrate; adverse effects include CNS depression and hypoglycemia
- Not indicated if fomepizole is available
3. Hemodialysis
Indications (any of the following):
- pH ≤ 7.15
- Coma or seizures
- Shock
- Visual deficits / blindness
- Significant renal impairment
- Methanol level markedly elevated
Hemodialysis directly removes methanol and formic acid, and corrects acidosis. It is frequently required in methanol poisoning because fomepizole alone results in a very prolonged methanol half-life.
4. Sodium Bicarbonate
- Temporizing measure for severe acidosis
- Does not treat or reverse the underlying toxicity
- Also used in dialysate during hemodialysis
5. Folate / Leucovorin
-
Folinic acid (leucovorin) or folic acid 1 mg/kg IV (max 50 mg) every 4-6 hours
-
Promotes the folate-dependent pathway that metabolizes formic acid to CO₂ + H₂O (non-toxic)
-
Should be given in all methanol poisonings
-
Washington Manual of Medical Therapeutics, pp. 1099-1101; Comprehensive Clinical Nephrology, 7th Ed.
Treatment Summary Table
| Intervention | Role | Dose |
|---|---|---|
| Fomepizole | ADH inhibitor (blocks toxic metabolism) | 15 mg/kg IV load → 10 mg/kg q12h |
| Ethanol | ADH competitor (if fomepizole unavailable) | 0.6 g/kg load → 66 mg/kg/h |
| Hemodialysis | Removes methanol + formic acid, corrects acidosis | Indications: pH ≤7.15, coma, seizures, vision loss |
| NaHCO₃ | Treat severe acidosis | Per clinical severity |
| Folate/Leucovorin | Accelerates formic acid detoxification | 1 mg/kg IV (max 50 mg) q4-6h |
Key Points to Remember
- The latent period (12+ hours) is due to slow accumulation of formic acid
- Formic acid, not methanol itself, causes blindness and acidosis
- Early diagnosis relies on osmolar gap; late diagnosis relies on anion gap metabolic acidosis
- Fomepizole has replaced ethanol as first-line therapy
- Hemodialysis is often required because fomepizole alone prolongs methanol's half-life dramatically
- Folate is always co-administered to help detoxify formic acid via the folate pathway
This is a shared conversation. Sign in to Orris to start your own chat.