Ankylosing spondilitis
Reading File
Finding Sources
Searching PubMed
"ankylosing spondylitis"[MeSH Terms] AND treatment
Finding Sources
Reading File
Reading File
Reading File
Reading File
Searching PubMed
"ankylosing spondylitis"[MeSH Terms] AND biologics
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Here is a comprehensive overview of Ankylosing Spondylitis (AS).
Ankylosing Spondylitis
Definition & Classification
Ankylosing spondylitis (AS) — now formally termed radiographic axial spondyloarthritis (r-AxSpA) — is the most common chronic inflammatory disorder of the axial skeleton. It belongs to the family of spondyloarthropathies, which also includes psoriatic arthritis, reactive arthritis, and enteropathic arthritis.
The ASAS (Assessment of SpondyloArthritis international Society) classification distinguishes:
- Radiographic axial SpA (AS): structural damage visible on plain radiograph of the sacroiliac joint
- Non-radiographic axial SpA: active MRI inflammation without plain radiograph changes
Epidemiology
- Prevalence ~0.2% of the general population; ~2% of HLA-B27–positive individuals; ~20% of B27+ individuals with an affected first-degree relative
- Historically male-predominant (2.5–5:1), though more recent studies suggest a lower ratio
- Onset typically in adolescents and young adults (back pain before age 45)
Pathobiology
| Mechanism | Detail |
|---|---|
| HLA-B27 | Present in ~90% of AS patients; strongest genetic risk factor |
| ERAP1 | Endoplasmic reticulum aminopeptidase-1 polymorphisms are the second strongest genetic risk factor |
| Molecular mimicry | Sequence homology between HLA-B27 and gram-negative enteric bacteria proposed |
| Unfolded protein response | HLA-B27 misfolds in the ER, triggering a pro-inflammatory cascade |
| Heavy-chain homodimers | HLA-B27 forms homodimers at the cell surface, activating NK and T cells |
| IL-17/IL-23 axis | Key inflammatory pathway driving enthesitis and new bone formation |
Clinical Features
Axial Disease (Cardinal Feature)
- Inflammatory back pain: insidious onset, worse at rest/night, improves with exercise, morning stiffness >1 hour
- Sacroiliitis: bilateral and symmetrical — pathognomonic
- Enthesitis: inflammation at tendon/ligament insertions (Achilles, plantar fascia)
- Syndesmophytes: vertical, marginal bony outgrowths; progression to the classic bamboo spine if untreated
Peripheral Disease (up to 30%)
- Asymmetrical oligoarthritis; lower extremity predominant
- Hip involvement can occur at any stage and may progress to joint destruction
Extra-articular Manifestations
| Feature | Frequency |
|---|---|
| Acute anterior uveitis (iritis) | ~40% — unilateral, recurrent, photophobia |
| Inflammatory bowel disease | ~10% |
| Psoriasis | ~10% |
| Aortic insufficiency | Less common |
| Cardiac conduction defects | Up to 30% (subaortic fibrosis extending into AV node) |
| Restrictive lung disease / apical fibrosis | Late complication |
| Osteoporosis | Significant; vertebral fractures and cauda equina syndrome possible |
Diagnosis
ASAS Classification Criteria
Chronic back pain before age 45 and >3 months, PLUS either:
- Imaging arm: Sacroiliitis on plain radiograph OR active MRI inflammation + ≥1 other criterion
- Clinical arm: HLA-B27 positive + ≥2 other criteria
Other supporting criteria include: elevated CRP, enthesitis (heel), family history of SpA, inflammatory back pain, good response to NSAIDs, psoriasis, Crohn/UC, dactylitis, HLA-B27 positivity
Modified New York Radiologic Criteria for Sacroiliitis
- Grade ≥2 bilateral, or grade 3–4 unilateral
- Definite AS = radiologic criterion + ≥1 clinical criterion
Imaging Sequence
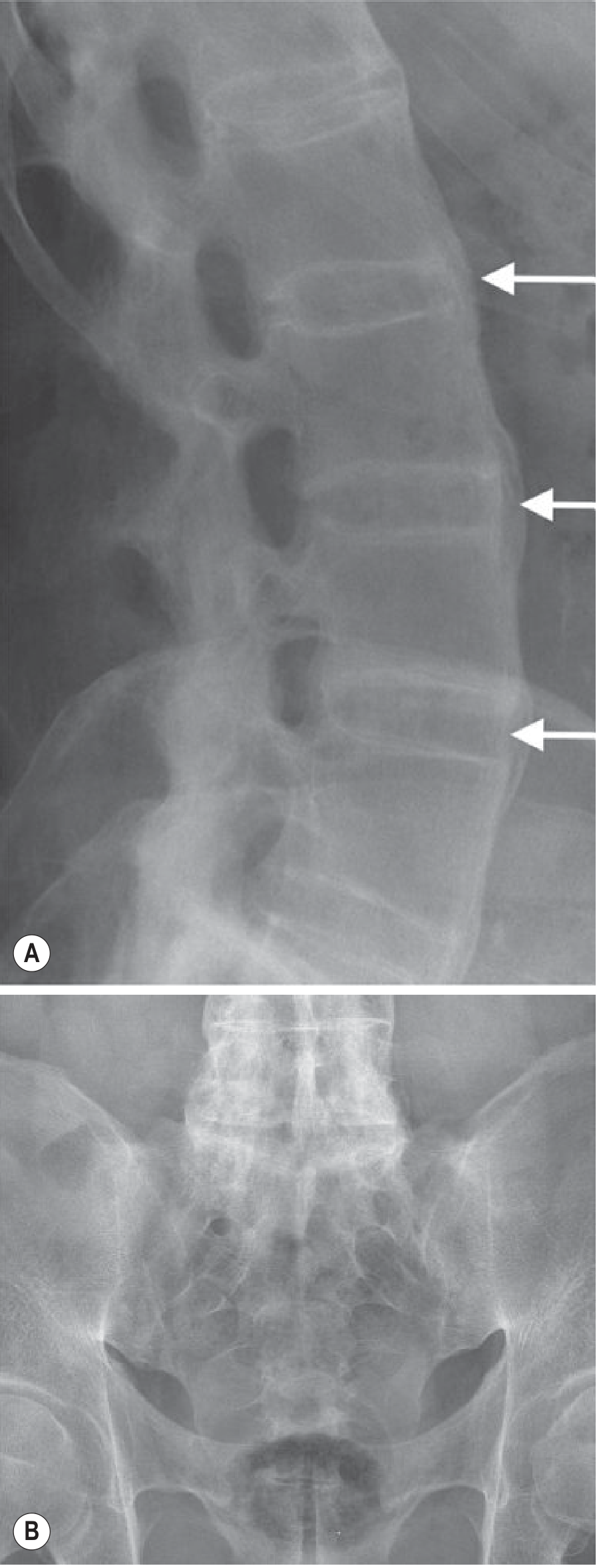
- Plain radiograph (X-ray): First-line; shows sacroiliac joint sclerosis, erosions, ankylosis; Romanus lesions (sclerotic/eroded vertebral corners); bamboo spine (late)
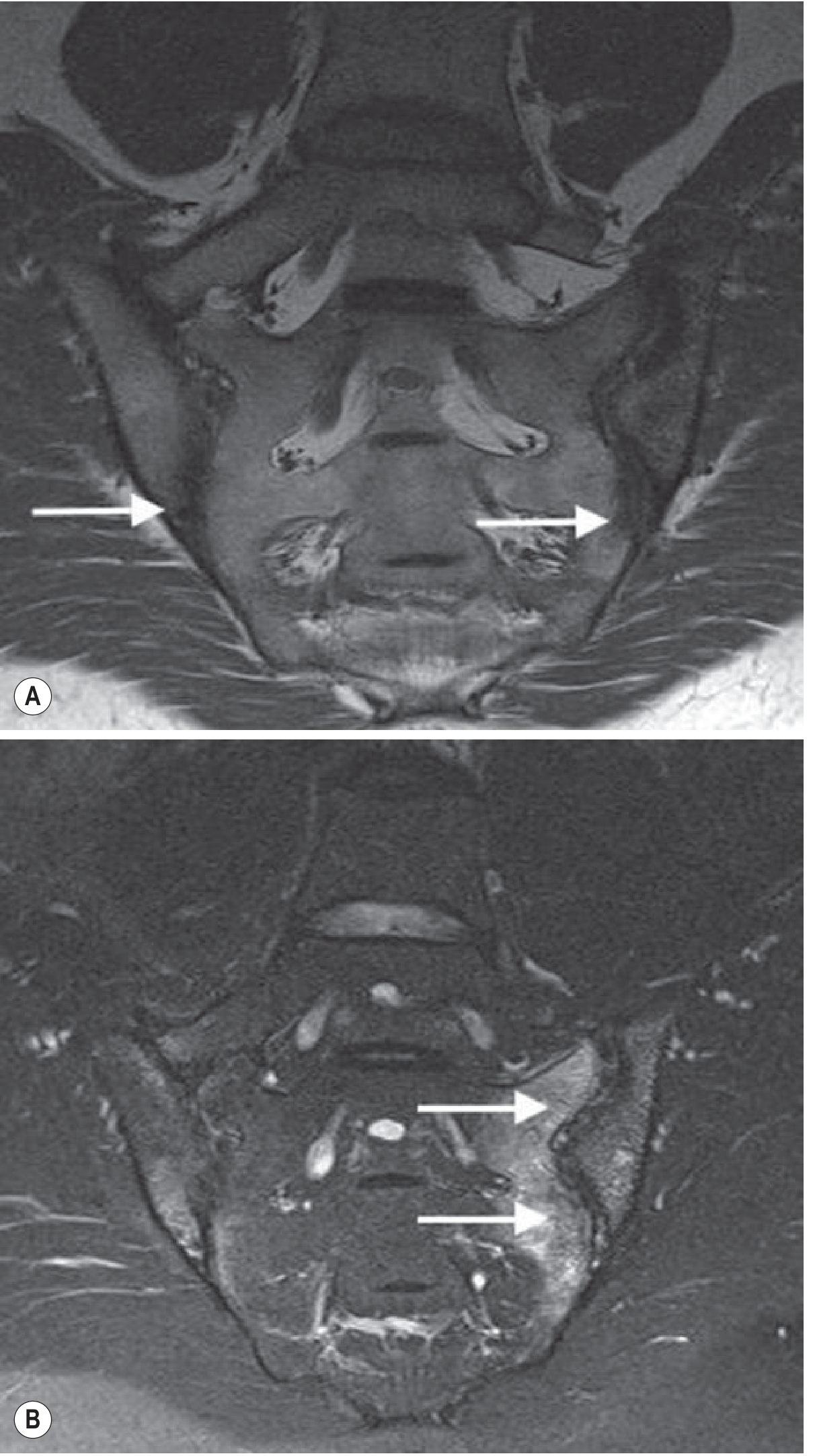
- MRI: Most sensitive for early sacroiliitis — detects subchondral bone marrow edema before X-ray changes; preferred for diagnosis
- CT: Superior for erosions and ankylosis, but high radiation dose
Radiologic Progression

Key radiologic distinction from other SpA:
| Feature | AS | Reactive/Psoriatic Arthritis |
|---|---|---|
| Sacroiliitis | Bilateral, symmetrical | Unilateral/asymmetrical |
| Syndesmophytes | Smooth, marginal, vertical | Coarse, non-marginal, bulky |
Differential Diagnosis vs. Rheumatoid Arthritis
| Feature | Rheumatoid Arthritis | Ankylosing Spondylitis |
|---|---|---|
| Sex ratio (M:F) | 1:3 | 3:1 |
| HLA association | DR4 | B27 |
| Joint pattern | Symmetrical, peripheral | Axial |
| Sacroiliac | Absent | Symmetrical |
| Eye | Scleritis | Iritis |
| Rheumatoid factor | >80% | Rare |
Management
Step 1 — Physical Therapy (all patients)
Regular exercise and physiotherapy to maintain posture and range of motion; essential throughout all disease stages.
Step 2 — NSAIDs (first-line pharmacotherapy)
- Full therapeutic doses; many patients require long-term continuous use
- Evidence of possible structural benefit (slowing syndesmophyte formation) with continuous vs. on-demand use
- First-line for symptom control of axial disease
Step 3 — Biologics (refractory disease)
TNF-α inhibitors (e.g., adalimumab, etanercept, infliximab, certolizumab, golimumab)
- Highly effective for both axial and peripheral disease
- Cochrane-level evidence supports their use (Maxwell et al., 2015)
- First choice when NSAIDs fail
IL-17A inhibitors (secukinumab, ixekizumab)
- RCT evidence (Baeten et al., NEJM 2015): secukinumab significantly effective in AS
- Preferred over TNF inhibitors in patients with comorbid psoriasis; avoid in IBD
Peripheral arthritis
- Sulfasalazine or methotrexate (conventional DMARDs) for predominantly peripheral disease
- Anti-TNF for refractory cases
Surgical
- Hip arthroplasty for severe hip involvement
- Spinal fractures in fused spine require urgent stabilization (highly unstable, potentially catastrophic)
Complications & Prognosis
- Syndesmophyte progression is predicted by presence of syndesmophytes at baseline
- Spinal fracture: increased risk due to osteopenia + rigid spine; minimal trauma can cause transverse fracture
- Osteoporosis: due to chronic inflammation and abnormal biomechanical loading
- Cauda equina syndrome (late)
- Spondylodiscitis (Andersson lesion): inflammatory disc lesion at unfused segments; may mimic infection
- Restrictive lung disease: chest wall rigidity + upper lobe fibrosis/bullae (no proven therapy for apical fibrobullous disease)
- Work disability and quality of life significantly affected; clinical course is highly variable
Sources: Goldman-Cecil Medicine (International Edition), Grainger & Allison's Diagnostic Radiology, Fuster & Hurst's The Heart, Goodman & Gilman's Pharmacological Basis of Therapeutics.
This is a shared conversation. Sign in to Orris to start your own chat.