Postoperative nausea and vomiting
Reading File
Finding Sources
Searching PubMed
"postoperative nausea and vomiting" AND prevention
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Excellent - I now have comprehensive information. Let me compile the full answer.
Postoperative Nausea and Vomiting (PONV)
Definition and Incidence
PONV refers to nausea, retching, and/or vomiting occurring in the first 24-48 hours after surgery. Without prophylaxis, it affects approximately 30% of the general surgical population and up to 70-80% in patients with multiple predisposing risk factors. It is one of the most common and distressing complications in the postanesthesia care unit (PACU).
Pathophysiology
The vomiting reflex is coordinated by the vomiting center in the medulla, which receives input from multiple sources including:
- Chemoreceptor trigger zone (CTZ) - located in the area postrema (outside the blood-brain barrier), rich in dopamine (D2), serotonin (5-HT3), neurokinin-1 (NK1), and opioid receptors
- Vestibular system - histamine (H1) and acetylcholine (muscarinic) receptors dominate
- Vagal afferents from the GI tract - 5-HT3 receptors
- Higher cortical centers - emotion, pain, smell
Activating any of these receptor systems can precipitate nausea and vomiting, which guides pharmacologic targeting.
Risk Factors
Apfel Score (Adults) - Simplified Risk Prediction
| Risk Factor | Points |
|---|---|
| Female gender | 1 |
| Nonsmoker | 1 |
| History of PONV or motion sickness | 1 |
| Postoperative opioid use | 1 |
| Total | 0-4 |
Predicted PONV risk: 0 factors ~10% | 1 factor ~20% | 2 factors ~40% | 3 factors ~60% | 4 factors ~80%
Evidence-Based Risk Factor Classification (SAMBA Guidelines)
| Category | Factors |
|---|---|
| Established risk factors | Female sex, history of PONV/motion sickness, nonsmoking status, younger age, general vs regional anesthesia, volatile anesthetics and N2O, postoperative opioids, longer anesthesia duration, surgery type (cholecystectomy, laparoscopic, gynecologic) |
| Conflicting evidence | ASA physical status, menstrual cycle, neostigmine for NMB reversal |
| Disproven/limited relevance | BMI, anxiety, nasogastric tube, supplemental oxygen, perioperative fasting, migraine |
Pediatric Risk (Eberhart Score)
Surgery ≥30 min, age ≥3 years, strabismus surgery, history of POV or family history of PONV - scores 0-4 correspond to ~10%, 10%, 30%, 50%, 70% risk.
PONV Management Algorithm
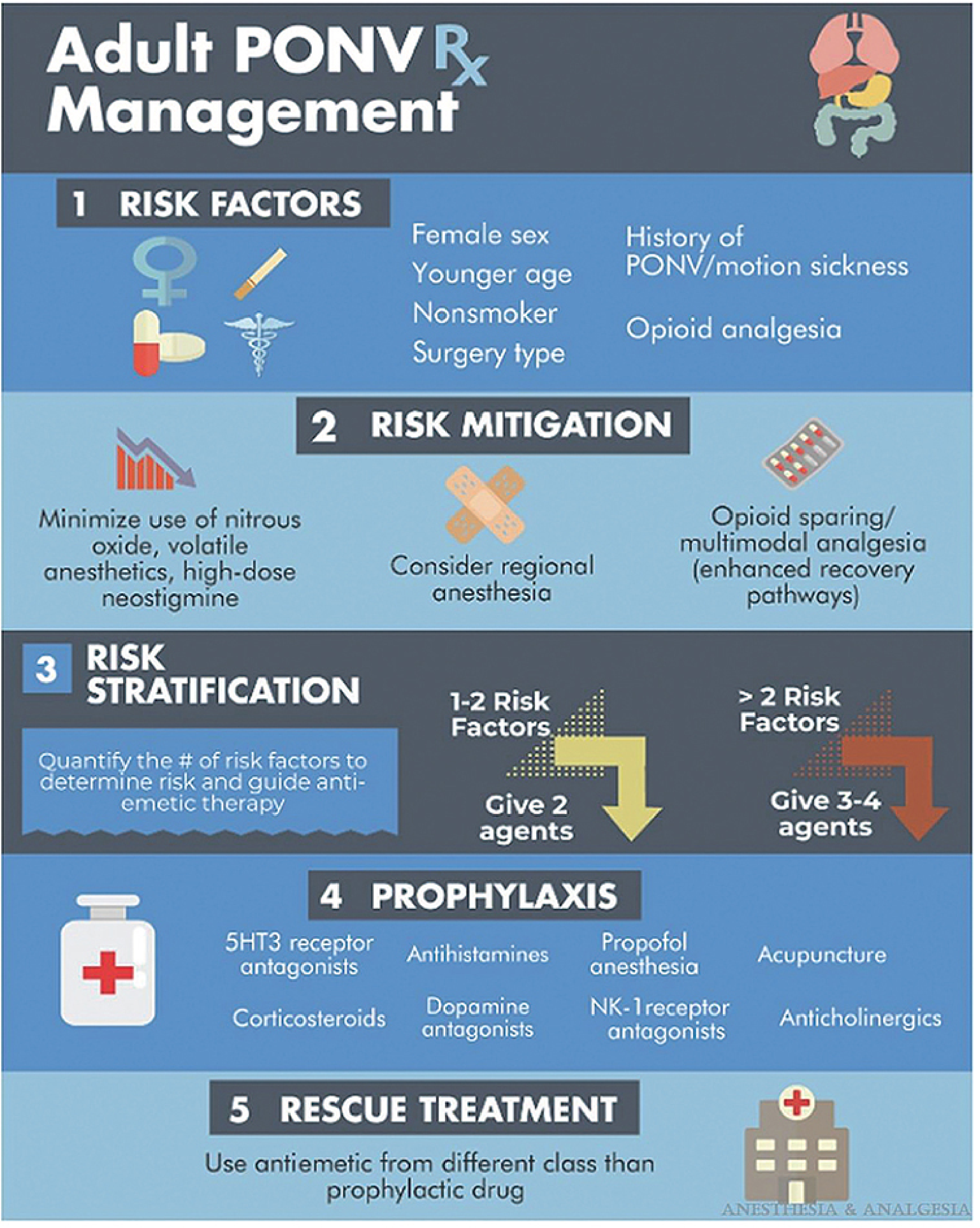
Step 1: Risk Mitigation (Non-Pharmacologic)
Before reaching for antiemetics, reduce baseline risk:
- Use regional anesthesia instead of general anesthesia when possible
- Use propofol for induction AND maintenance (total intravenous anesthesia, TIVA)
- Avoid nitrous oxide in surgeries lasting >1 hour
- Avoid volatile anesthetics
- Minimize intraoperative and postoperative opioids (multimodal analgesia, enhanced recovery pathways)
- Ensure adequate hydration
- Use sugammadex instead of neostigmine for neuromuscular blockade reversal
Step 2: Risk Stratification and Prophylaxis
Number of prophylactic agents should match risk level:
- 1-2 risk factors → 2 antiemetic agents
- >2 risk factors (high risk) → 3-4 antiemetic agents
Pharmacologic Prophylaxis and Treatment
Drug Classes and Mechanisms
| Drug Class | Agents | Key Notes |
|---|---|---|
| 5-HT3 receptor antagonists | Ondansetron, granisetron, ramosetron | First-line; headache/constipation as side effects |
| NK1 receptor antagonists | Aprepitant (40 mg PO), fosaprepitant | Most effective single agent per Cochrane review; given preoperatively |
| Corticosteroids | Dexamethasone (4-8 mg IV) | Given at induction; risk of glucose intolerance, wound healing concerns |
| D2 receptor antagonists (butyrophenones) | Droperidol, haloperidol | Droperidol has FDA black box warning for QTc prolongation - requires ECG monitoring |
| D2 antagonists (phenothiazines) | Prochlorperazine, chlorpromazine | Sedation; extrapyramidal effects |
| Antihistamines (H1) | Diphenhydramine, promethazine, meclizine | Sedation, dry mouth; useful for motion-sickness-mediated PONV |
| Anticholinergics | Transdermal scopolamine, atropine | Applied 4 hours preoperatively; dry mouth, sedation, blurred vision |
| Propofol anesthesia | Propofol infusion | Antiemetic properties at subhypnotic doses; useful in high-risk patients |
Key Dosing Points
- Ondansetron: 4 mg IV at end of surgery (adults); 50-100 mcg/kg in children
- Dexamethasone: 4-8 mg IV at induction
- Aprepitant: 40 mg PO preoperatively - most effective single agent for reducing postoperative vomiting
- Droperidol: 0.625-1.25 mg IV - effective but requires QTc monitoring due to FDA black box warning
Combination Therapy
Combination of agents from different classes is more efficacious than any single drug. The ondansetron + dexamethasone combination is the most widely used two-drug regimen.
Rescue Treatment
For breakthrough PONV (nausea/vomiting despite prophylaxis):
- Use an antiemetic from a different drug class than the prophylactic agent used
- If ondansetron was given prophylactically, giving another dose is unlikely to be effective - switch to a D2 antagonist, dexamethasone, or scopolamine patch
- Low-dose propofol (20 mg IV boluses) can be used as rescue in the PACU
PONV vs PDNV
Postdischarge nausea and vomiting (PDNV) occurs after hospital discharge (>2 hours postoperatively in ambulatory patients). Risk factors slightly differ - female sex, age <50, history of PONV, opioid use in PACU, and nausea in PACU are the strongest predictors.
Special Considerations
- Pregnancy: Ondansetron is the preferred antiemetic; avoid droperidol
- Pediatrics: Ondansetron + dexamethasone combination is standard; droperidol is used but requires caution; propofol TIVA reduces risk
- Cardiac patients: Avoid droperidol if prolonged QTc; haloperidol at low doses (0.5-1 mg) is safer
- Laparoscopic/bariatric surgery: High-risk procedures; opioid-free or opioid-sparing anesthesia significantly reduces PONV (per 2025 meta-analysis, PMID 38578868)
Sources: Morgan and Mikhail's Clinical Anesthesiology 7e, p. 514-517; Sabiston Textbook of Surgery, Table 20.9; Barash Clinical Anesthesia 9e; SAMBA Consensus Guidelines (Gan TJ et al., Anesth Analg 2014)
This is a shared conversation. Sign in to Orris to start your own chat.