A newly diagnosed patient with type 2 diabetes mellitus have HbA1c of 8.6. Uh, he's also a known case of hypertension and is suffering from CKD. So what should be the first choice of antidiabetic drug for this patient?
Reading File
Finding Sources
Finding Sources
Searching PubMed
"SGLT2 inhibitor" AND "chronic kidney disease" AND "type 2 diabetes"
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a comprehensive, well-sourced answer.
First-Choice Antidiabetic Drug: T2DM + Hypertension + CKD
For this patient - newly diagnosed T2DM, HbA1c 8.6%, hypertension, and CKD - the first-choice antidiabetic drug is an SGLT2 inhibitor (empagliflozin, dapagliflozin, or canagliflozin), provided eGFR ≥20 mL/min/1.73 m².
This is clearly recommended by the KDIGO 2022 Clinical Practice Guideline for Diabetes Management in CKD, as represented in the treatment algorithm below:
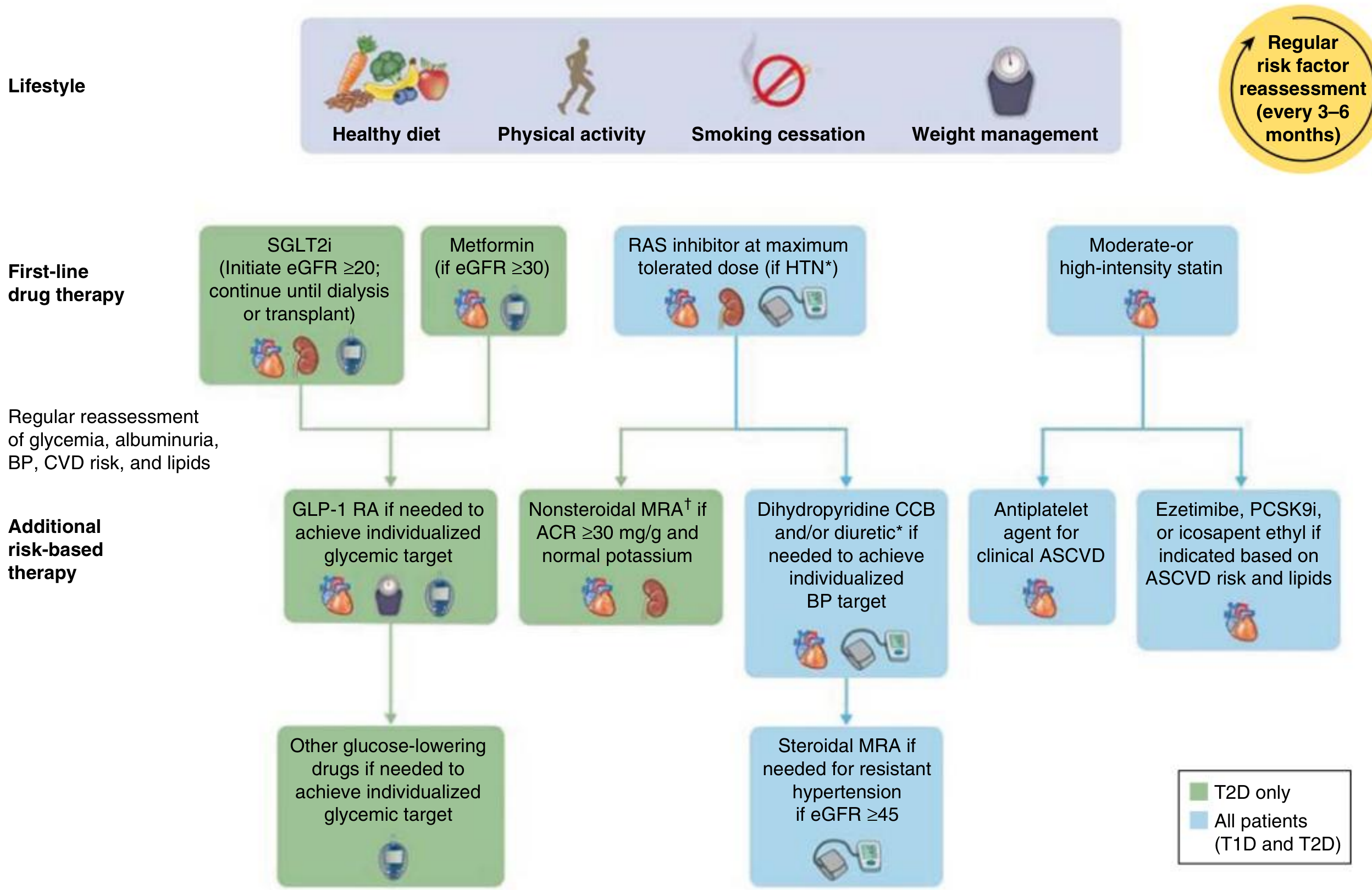
Why SGLT2 Inhibitors Are the Top Choice Here
1. Renoprotection (the primary driver)
SGLT2 inhibitors are now the most potently renoprotective glucose-lowering agents available. Their effect size for kidney protection in T2DM is approximately 2.5 times the protective effect of RAS inhibition when added on top of a maximally tolerated RAS inhibitor - no other drug class currently matches this. They reduce albuminuria by 30-40% and dramatically slow the chronic slope of eGFR decline. In a typical patient with CKD stage G3 (eGFR ~55), SGLT2i can potentially delay or prevent the initiation of dialysis by more than a decade. - Comprehensive Clinical Nephrology, 7th Ed.
Multiple large outcome trials (EMPA-REG OUTCOME, CREDENCE, DAPA-CKD, EMPA-KIDNEY) have consistently shown a 30-50% reduction in kidney failure events. Crucially, these benefits are additive to RAAS blockade therapy. - National Kidneys Foundation Primer on Kidney Diseases, 8e
2. Mechanism of renoprotection
- Blockade of SGLT2/SGLT1 in the proximal tubule causes sodium spillover to the macula densa, restoring tubuloglomerular feedback and reducing glomerular capillary pressure (afferent vasoconstriction) - this directly reverses diabetic glomerular hyperfiltration.
- The result is preservation of single-nephron GFR and reduced progression to ESRD. - Brenner and Rector's The Kidney
3. Antihypertensive benefit
SGLT2 inhibitors reduce systolic BP by 4-6 mmHg and diastolic BP by 1-2 mmHg via an osmotic diuretic and natriuretic effect. In a patient who already has hypertension, this is an additional therapeutic bonus.
4. Cardiovascular benefit
All three major SGLT2 inhibitors reduce CV morbidity and all-cause mortality in patients with CKD - independent of diabetes status. Given that hypertension + CKD already confers elevated CV risk, this is a major advantage.
5. Weight and metabolic benefits
Weight loss of 1-4 kg and favorable effects on hepatic glucose output and beta-cell preservation are additional bonuses for T2DM management.
What About Metformin?
Metformin remains the preferred initial antihyperglycemic drug for T2DM in general due to its low cost and low hypoglycemia risk. However, its use in CKD is restricted:
| eGFR | Metformin guidance |
|---|---|
| ≥45 mL/min/1.73 m² | Full dose acceptable |
| 30-44 mL/min/1.73 m² | Reduce to 500 mg twice daily; use cautiously |
| <30 mL/min/1.73 m² | Contraindicated (risk of lactic acidosis) |
- Comprehensive Clinical Nephrology, 7th Ed.; The Washington Manual of Medical Therapeutics
So metformin may be added as a second agent if eGFR is ≥30, but should not be the primary choice in a CKD patient when SGLT2i offers both glycemic control and organ protection.
Complete First-Line Management Bundle for This Patient
| Drug class | Role |
|---|---|
| SGLT2 inhibitor (empagliflozin/dapagliflozin/canagliflozin) | 1st-line antidiabetic + renoprotection + BP lowering |
| ACE inhibitor or ARB | 1st-line antihypertensive in diabetic CKD + antiproteinuric |
| Metformin (if eGFR ≥30) | Add for additional glycemic control if needed |
| GLP-1 RA | Add if HbA1c target not met with SGLT2i ± metformin |
| Moderate/high-intensity statin | Cardiovascular risk reduction |
Note: With HbA1c 8.6%, this patient will likely need both SGLT2i and metformin (if eGFR permits) for adequate glycemic control, as SGLT2i alone typically reduces HbA1c by only 0.6-0.9%. GLP-1 RA (e.g., semaglutide) can be added if needed.
Key Safety Consideration for SGLT2i
- Do not use if eGFR <20 mL/min/1.73 m²
- Avoid in active foot ulcers, lower extremity ischemia, or advanced liver disease
- Monitor for genital mycotic infections (most common side effect) and the rare risk of euglycemic DKA (~13/1000 patient-years)
- An initial eGFR dip of >10% occurs in ~1/3 of patients but is fully reversible and does not warrant discontinuation
Bottom line: An SGLT2 inhibitor is the first-choice antidiabetic agent for this patient because it simultaneously addresses hyperglycemia, slows CKD progression, lowers BP, and reduces cardiovascular risk - making it uniquely suited for the triad of T2DM + hypertension + CKD. This is the recommendation of the KDIGO 2022 guidelines, ADA/EASD consensus, and is backed by recent meta-analyses (PMID: 41203232, 38991584, 41147324) confirming benefit across GFR and albuminuria categories.
This is a shared conversation. Sign in to Orris to start your own chat.