Mast cell disorders
Reading File
Finding Sources
Searching PubMed
"mast cell disorders" AND "mastocytosis"
Searching the Web
mast cell disorders classification diagnosis treatment 2024 2025
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
I now have sufficient information to compose a comprehensive response. Let me write it up.
Mast Cell Disorders
Mast cell disorders are a heterogeneous group of conditions caused by either pathologic accumulation of mast cells in tissues (mastocytosis) or inappropriate mast cell activation with excessive mediator release (mast cell activation syndrome, MCAS). They span a wide clinical spectrum from benign self-resolving skin disease in children to aggressive, life-threatening hematologic malignancy.
1. The Mast Cell - Biology
Mast cells arise from CD34+, KIT+ (CD117) pluripotent progenitor cells in the bone marrow. After migrating into peripheral tissues, they acquire their characteristic granular morphology. Key features:
- KIT (CD117): A Type III receptor tyrosine kinase, product of the proto-oncogene c-kit (chromosome 4q12). Its ligand is Stem Cell Factor (SCF), also called KIT ligand, which is required for mast cell maturation, proliferation, and survival.
- Subtypes based on neutral protease content:
- MC-TC: Contain both tryptase and chymase (skin, intestinal submucosa)
- MC-T: Contain tryptase only (bowel mucosa, alveolar wall, nasal mucosa)
- Both subtypes express high-affinity IgE receptors (FcεRI) and can participate in IgE-dependent reactions.
- Cytokines regulating mast cell growth include IL-3, IL-4, IL-6, IL-9, and IFN-γ.
- Dermatology 2-Volume Set 5e (Griffiths); Fitzpatrick's Dermatology, Vol. 1-2
2. Mast Cell Degranulating Stimuli
Mast cells release preformed mediators (histamine, tryptase, chymase, heparin) and newly generated mediators (prostaglandins, leukotrienes, platelet-activating factor, cytokines).
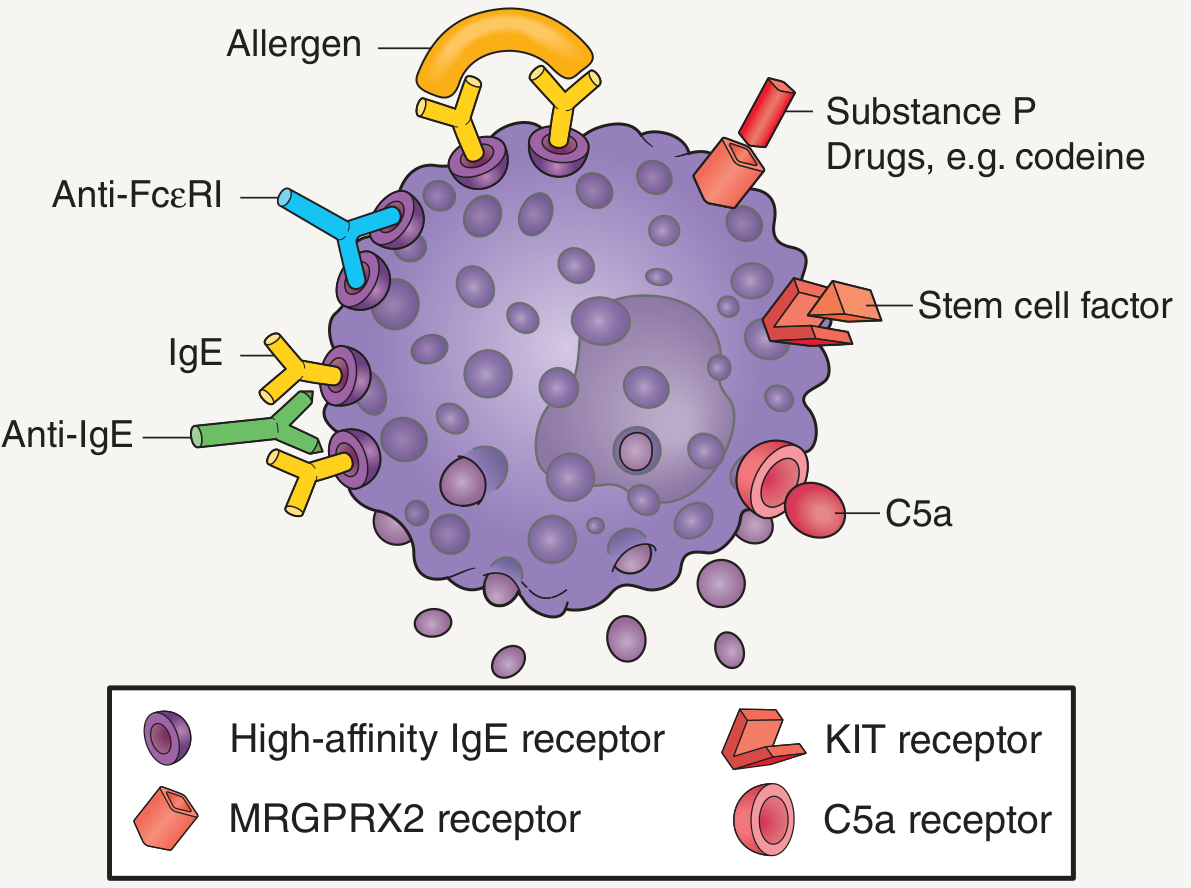
Immunologic triggers:
- Allergen cross-linking of IgE bound to FcεRI (classic Type I hypersensitivity)
- IgG anti-IgE and anti-FcεRI autoantibodies
Non-immunologic triggers:
- Substance P, drugs (e.g., codeine, NSAIDs, opioids)
- Complement fragments (C5a)
- Physical stimuli (heat, friction, pressure)
- MRGPRX2 receptor activation
3. Classification of Mast Cell Disorders
Mast cell disorders divide into two major categories:
A. Mastocytosis (Clonal Mast Cell Neoplasms)
WHO 5th Edition Classification (2022):
| Category | Key Features |
|---|---|
| Cutaneous Mastocytosis (CM) | Skin only, no systemic involvement |
| Indolent Systemic Mastocytosis (ISM) | Most common adult form; low mast cell burden; near-normal life expectancy |
| Bone Marrow Mastocytosis | BM involvement; no skin lesions; low burden |
| Smoldering Systemic Mastocytosis (SSM) | High mast cell burden; hepatosplenomegaly; serum tryptase >200 ng/mL |
| SM with Associated Hematologic Neoplasm (SM-AHN) | SM + co-existing hematologic disorder (most commonly MDS, MPN) |
| Aggressive Systemic Mastocytosis (ASM) | Organ damage (C-findings); rapidly increasing MC numbers |
| Mast Cell Leukemia (MCL) | >20% mast cells in bone marrow smear; ≥10% in peripheral blood; multiorgan failure |
| Mast Cell Sarcoma | Localized destructive growth; highly atypical/immature mast cells |
- Goldman-Cecil Medicine, Table 235-1; Fitzpatrick's Dermatology, Ch. 42
B. Mast Cell Activation Syndrome (MCAS)
Characterized by symptoms of mast cell mediator release WITHOUT evidence of unregulated mast cell proliferation. Divided into:
- Clonal (monoclonal) MCAS: Has KIT D816V or abnormal MC immunophenotype but does not meet full SM criteria
- Secondary MCAS: Due to IgE-mediated allergy, chronic urticaria, or other triggers
- Idiopathic (nonclonal) MCAS: No clonal or secondary cause identified
- Fitzpatrick's Dermatology, Akin C 2026 (PMID 41285202)
4. Pathogenesis - KIT Mutations
The hallmark molecular event in mastocytosis is an activating point mutation in the KIT gene:
- KIT D816V (exon 17) - present in >90% of adult SM cases; causes ligand-independent, constitutive KIT activation
- Also found in CBF-AML, GI stromal tumors, and a subset of melanomas
- D816V is resistant to imatinib (unlike exon 11 mutations which are sensitive)
- Midostaurin (PKC412): FDA-approved 2017 for ASM, SM-AHN, and MCL - the first targeted therapy active against D816V mutant KIT
- Avapritinib: More selective KIT D816V inhibitor, approved 2021 for adults with ASM, SM-AHN, MCL
- Henry's Clinical Diagnosis and Management by Laboratory Methods; Fitzpatrick's Dermatology
5. Clinical Presentation
Cutaneous Manifestations
| Lesion | Features |
|---|---|
| Urticaria Pigmentosa (UP) | Most common; tan-brown papules/macules; Darier's sign positive; predominantly trunk |
| Solitary Mastocytoma | Children; tan-brown nodule, usually distal extremities; onset before 6 months |
| Diffuse Cutaneous Mastocytosis (DCM) | Diffuse dermal infiltration; rare; may cause bullae in infants |
| Telangiectasia Macularis Eruptiva Perstans (TMEP) | Adults; telangiectatic macules |
Darier's sign: Urtication and erythema when skin lesion is vigorously rubbed - pathognomonic.
Childhood lesions: MC concentration 40-150x normal (explains more pronounced reactions). Adult lesions: only ~8x normal.
Systemic Manifestations
Mast cell mediator symptoms (from histamine, prostaglandins, tryptase):
- Flushing, pruritus, urticaria
- Hypotension, anaphylaxis (particularly triggered by Hymenoptera stings)
- Nausea, dyspepsia, diarrhea, peptic ulcer disease (histamine-driven gastric acid hypersecretion)
- Headache, cognitive difficulties
- Osteoporosis (from heparin and tryptase effect on bone)
Organ infiltration (advanced disease):
- Bone marrow, liver, spleen, lymph nodes most commonly involved
- Hepatosplenomegaly, malabsorption, cytopenias, portal hypertension
6. Diagnosis
Diagnostic Criteria for Systemic Mastocytosis (WHO)
Major criterion:
- Multifocal, dense mast cell aggregates (≥15 MCs in clusters) in bone marrow biopsy and/or other extracutaneous organs
Minor criteria (need 1 major + 1 minor, OR 3 minor):
-
25% of mast cells in BM smear are atypical (spindle-shaped) or multi-focal clusters >15 MCs
- Activating point mutation at codon 816 of KIT (usually D816V) in BM, blood, or other extracutaneous organ
- KIT+ mast cells co-express CD2 and/or CD25
- Total serum tryptase persistently >20 ng/mL (not valid if SM-AHN is present)
"B-Findings" (Burden) vs. "C-Findings" (Cytoreduction needed)
B-Findings (high burden but no organ damage):
- BM biopsy >30% mast cells, tryptase >200 ng/mL
- Dysplastic/hypercellular BM with signs of MPN/MDS
- Hepatomegaly without ascites; palpable splenomegaly without hypersplenism; lymphadenopathy
C-Findings (organ damage - indicates ASM):
- Cytopenias (ANC <1000, Hb <10, platelets <100)
- Hepatomegaly with portal hypertension, ascites
- Palpable splenomegaly with hypersplenism
- Malabsorption with weight loss
- Skeletal lesions with large osteolytic foci, pathologic fracture
Key Investigations
- Serum tryptase: Most validated marker; >20 ng/mL raises suspicion for SM; baseline tryptase helps monitor. Note: hereditary alpha-tryptasemia (HAT) can elevate baseline tryptase without SM.
- Skin biopsy: Shows mast cell aggregates; positive Darier sign guides sampling
- Bone marrow biopsy and aspirate: Required for diagnosis of SM; CD117 (KIT), CD2, CD25 immunostaining; KIT D816V molecular testing
- 24-hour urinary histamine metabolites
- CBC with differential, LFTs, DEXA scan for osteoporosis
Diagnostic Algorithm
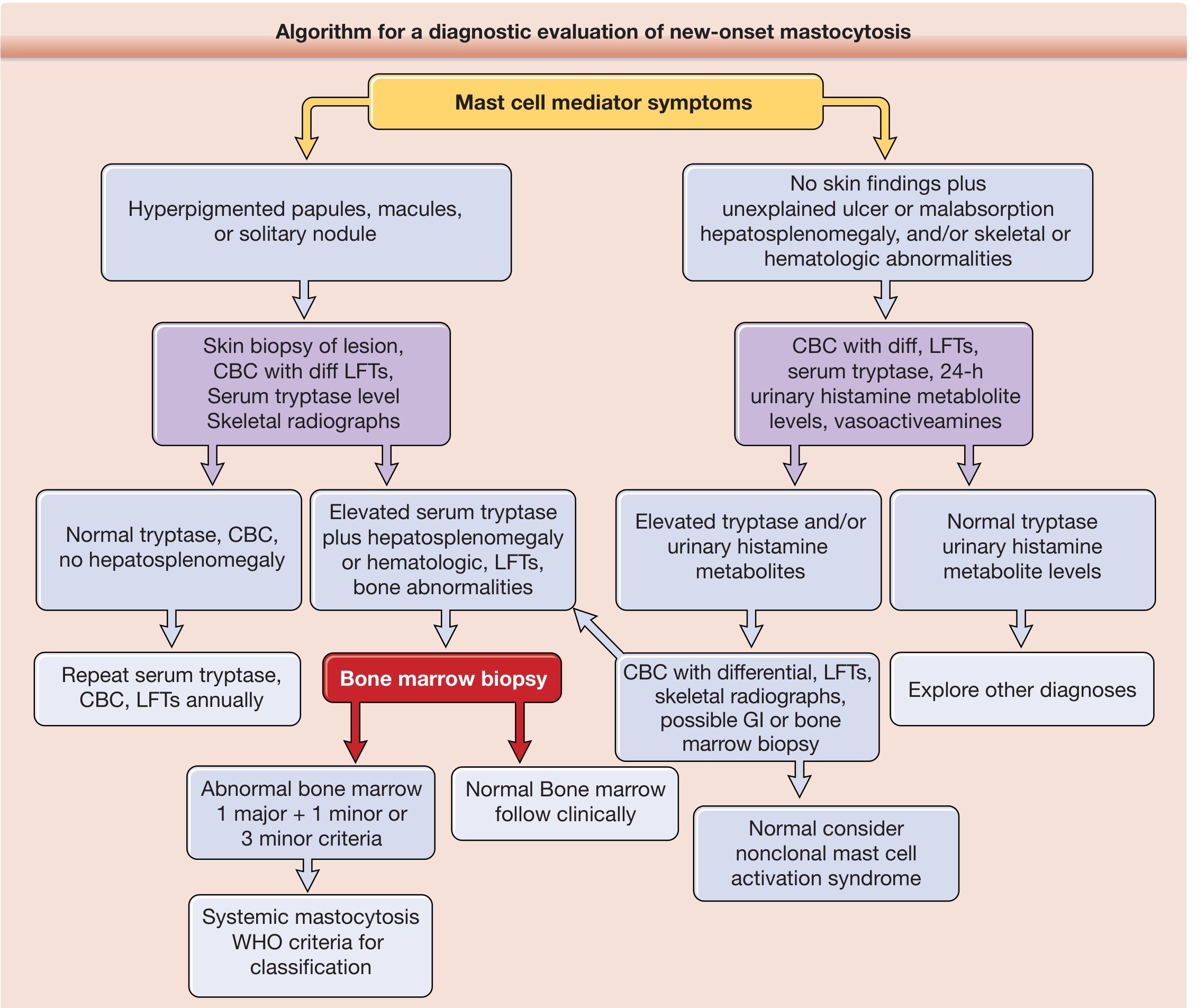
- Fitzpatrick's Dermatology, Fig. 42-9
7. Management
General Principles
Treatment is symptom-focused; no current cure for most forms. The goal is controlling mediator-related symptoms and, in advanced disease, reducing mast cell burden.
Mediator Symptom Control (All Forms)
| Drug | Target | Use |
|---|---|---|
| H1 antihistamines (cetirizine, loratadine) | Histamine H1 | Urticaria, pruritus, flushing |
| H2 antihistamines (famotidine, ranitidine) | Histamine H2 | GI symptoms, peptic ulcers |
| Cromolyn sodium (mast cell stabilizer) | Mast cell membrane | GI symptoms; not systemically absorbed |
| Leukotriene antagonists (montelukast) | Cysteinyl LT receptor | Additional mediator blockade |
| Aspirin (low dose) | Prostaglandin D2 | Flushing; use cautiously (can trigger degranulation) |
| Epinephrine auto-injector | All mediators | Anaphylaxis - ALL patients should carry one |
| Bisphosphonates | Bone | Osteoporosis prevention/treatment |
Cytoreductive Therapy (Advanced Disease - ASM, SM-AHN, MCL)
| Agent | Mechanism | Indication |
|---|---|---|
| Midostaurin (Rydapt) | Multi-kinase inhibitor; active vs D816V | ASM, SM-AHN, MCL (FDA 2017) |
| Avapritinib (Ayvakit) | Selective KIT D816V + PDGFRα inhibitor | ASM, SM-AHN, MCL (FDA 2021) |
| Imatinib | KIT exon 11 inhibitor | Non-D816V mutations only; select cases |
| Cladribine (2-CdA) | Purine analogue | Cytoreduction in ASM/MCL |
| Interferon-alpha | Immunomodulator | Cytoreduction; second-line |
| Allogeneic SCT | Myeloablation | MCL, high-risk SM-AHN; potentially curative |
MCAS Management
- H1 + H2 antihistamines + leukotriene inhibitors (often sufficient)
- Avoid triggers (physical, pharmacologic)
- Omalizumab (anti-IgE) in refractory cases
- Epinephrine auto-injector for anaphylaxis risk
8. Prognosis
| Form | Prognosis |
|---|---|
| Pediatric CM | Excellent - 45-68% complete regression by adulthood |
| ISM (adult) | Near-normal life expectancy; cumulative risk of progression to advanced SM only 1.7% at 10 years, 8.4% at 25 years |
| SSM | Less favorable; watch for progression |
| SM-AHN | Dependent on the associated hematologic disorder |
| ASM | Poor without treatment; high mast cell burden, rapid progression |
| MCL | Very poor; median survival historically <6 months (improving with avapritinib/midostaurin) |
| Mast cell sarcoma | Very poor; aggressive local destruction with metastatic potential |
9. Recent Updates (2025-2026)
A 2026 review (Akin C et al., PMID 41285202) on MCAS diagnosis and management status 2026 highlights evolving diagnostic criteria and the growing recognition of hereditary alpha-tryptasemia (HAT) - a germline copy number gain in the TPSAB1 gene - as a distinct genetic condition that elevates baseline tryptase and predisposes to more severe mast cell activation symptoms. A 2025 review (Chantran & Arock, PMID 40612891) specifically addresses the overlap between HAT and monoclonal mast cell disorders.
A 2023 review (Li JY et al., PMID 38067330) provides updated classification and management guidance for systemic mastocytosis and related entities, including avapritinib's role as a highly selective and potent frontline option.
10. Key Associations and Exam Pearls
- Darier's sign = pathognomonic urtication on rubbing skin lesions
- KIT D816V = found in >90% of adult SM; resistant to imatinib; sensitive to avapritinib/midostaurin
- Tryptase = most specific and validated mast cell marker; use for diagnosis AND to monitor response
- Children with CM: mostly regress; adults rarely get complete remission
- Anaphylaxis with negative skin prick tests in otherwise healthy adult → think ISM or monoclonal MCAS
- SM + MDS/MPN = SM-AHN; prognosis driven by the hematologic component
- Mast cell leukemia: >20% MCs in BM smear + >10% in peripheral blood
- HAT + high tryptase: do not diagnose SM on elevated tryptase alone; requires BM biopsy
Sources: Fitzpatrick's Dermatology 9e, Goldman-Cecil Medicine, Henry's Clinical Diagnosis & Management by Laboratory Methods, Dermatology 2-Volume Set 5e, Harrison's Principles of Internal Medicine 22e (2025)
Secondary leukemia
Reading File
Finding Sources
Finding Sources
Searching PubMed
"therapy-related leukemia" OR "secondary AML"
Searching the Web
secondary leukemia therapy-related AML pathogenesis classification treatment 2024 2025
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.