Teach me about CKD
Reading File
Finding Sources
Finding Sources
Searching PubMed
"chronic kidney disease" management
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full educational response.
Chronic Kidney Disease (CKD)
Definition
CKD is defined as kidney damage or decreased kidney function persisting for 3 months or longer, regardless of the underlying cause. The primary measure of kidney function is the glomerular filtration rate (GFR), which forms the basis for staging. Kidney "damage" may manifest as pathologic renal abnormalities or markers of damage - abnormal blood tests, urine tests (especially proteinuria), or imaging findings.
- Textbook of Family Medicine 9e, p. 1191
- Harrison's Principles of Internal Medicine 22e, p. 2438
Epidemiology
- Approximately 20 million persons in the United States have CKD
- Leading cause of end-stage kidney disease (ESKD) in the US: diabetes mellitus (~45%), followed by hypertension (~30%)
- Other prevalent causes: glomerulonephritis, polycystic kidney disease, obstructive uropathy
- ESKD is disproportionately higher in African Americans, partly due to APOL1 high-risk gene alleles
- Over 800,000 patients in the US have treated ESKD (requiring dialysis or transplantation)
- Harrison's Principles of Internal Medicine 22e, p. 2437
Staging (KDIGO Classification)
Staging is based on GFR and albuminuria (the "G" and "A" categories):
| Stage | Description | GFR (mL/min/1.73 m²) |
|---|---|---|
| G1 | Kidney damage, normal GFR | ≥90 |
| G2 | Kidney damage, mild decrease | 60-89 |
| G3a | Mild-moderate decrease | 45-59 |
| G3b | Moderate-severe decrease | 30-44 |
| G4 | Severe decrease | 15-29 |
| G5 | Kidney failure (ESKD) | <15 |
Albuminuria categories (A1/A2/A3) are layered on top of GFR stage, as proteinuria independently predicts progression and cardiovascular risk.
The graph below illustrates how baseline proteinuria level (left panel) and change in proteinuria over 12 months (right panel) dramatically affect the likelihood of reaching a renal endpoint (doubling of creatinine, ESKD):
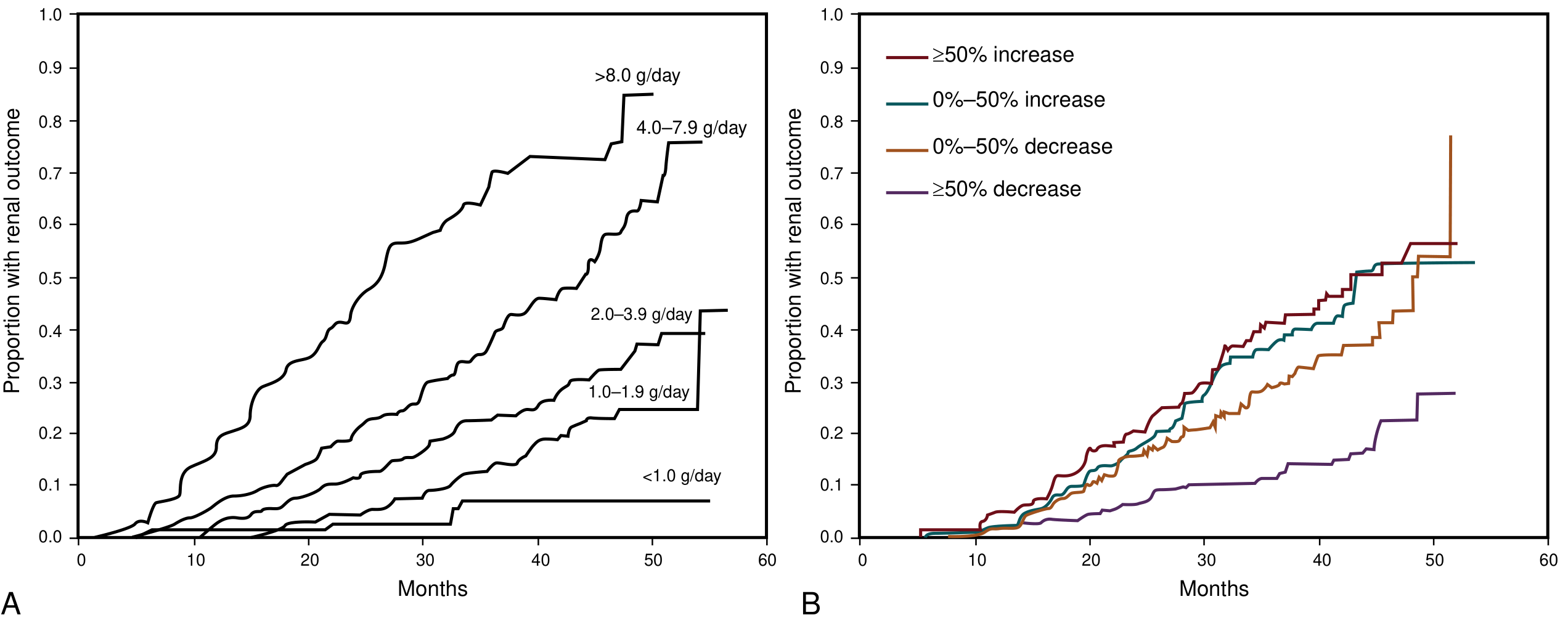
- Textbook of Family Medicine 9e, p. 1191
- NKF Primer on Kidney Diseases, 8e, p. 528
Common Causes / Etiologies
- Diabetic nephropathy - most common cause in developed countries
- Hypertensive nephrosclerosis - second most common
- Glomerulonephritis - (IgA nephropathy, FSGS, membranous, lupus nephritis)
- Polycystic kidney disease (PKD) - hereditary
- Tubulointerstitial nephritis - drug-induced, reflux, chronic infection
- Obstructive uropathy - BPH, stones, strictures
- Hereditary/genetic - Alport syndrome, Fabry disease, cystinosis, APOL1-related nephropathy
A careful drug history is essential: NSAIDs, COX-2 inhibitors, lithium, proton pump inhibitors, chemotherapeutic agents, and antiretrovirals can all contribute.
- Harrison's Principles of Internal Medicine 22e, p. 2437
Pathophysiology
Common Pathways of Progression
Regardless of the initial insult, CKD progresses through shared mechanisms:
-
Glomerular hyperfiltration - When nephrons are lost, surviving nephrons compensate by increasing single-nephron GFR. This hyperfiltration causes intraglomerular hypertension, podocyte injury, and eventual sclerosis - a self-perpetuating cycle of nephron loss.
-
Proteinuria and tubular toxicity - Filtered proteins are toxic to tubular cells, triggering inflammation, tubular atrophy, and interstitial fibrosis.
-
RAAS activation - Angiotensin II causes efferent arteriolar constriction (worsening glomerular hypertension), promotes fibrosis via TGF-β, and drives sodium retention and systemic hypertension.
-
Chronic inflammation and fibrosis - Progressive interstitial fibrosis via TGF-β, cytokines (TNF-α, IL-1, IL-6), and myofibroblast activation is the final common pathway to ESKD.
-
Metabolic acidosis - As GFR falls, the kidney loses ability to handle the daily dietary acid load. Acidosis accelerates bone disease, sarcopenia, and CKD progression itself.
-
AKI-on-CKD - Episodes of acute kidney injury accelerate progression and may account for a sizable fraction of ESKD cases. Iatrogenic AKI (hypotension, nephrotoxins, contrast) should be actively avoided.
- NKF Primer on Kidney Diseases, 8e, pp. 528-530
Clinical Presentation
Symptoms are often absent or subtle until advanced CKD. Common features include:
- Early/moderate CKD: usually asymptomatic; found incidentally on labs or urinalysis
- Hypertension - both a cause and consequence of CKD
- Edema - sodium and water retention
- Fatigue, pallor - from anemia of chronic kidney disease
- Sensory polyneuropathy - peripheral numbness/tingling
- Late/uremic CKD: nausea, anorexia, weight loss, hiccups, pruritus, muscle cramps, restless legs, asterixis ("flap"), pericardial friction rub
The physical exam should focus on blood pressure, target organ damage (fundoscopy in diabetics for retinopathy), edema, and neurological signs.
- Harrison's Principles of Internal Medicine 22e, p. 2437
Workup / Diagnosis
Laboratory
- Serum creatinine + eGFR (calculated by CKD-EPI or MDRD equation)
- Urine albumin-to-creatinine ratio (uACR) or 24-h urine protein
- Serum electrolytes - look for hyperkalemia, metabolic acidosis (low bicarb)
- Calcium, phosphorus, PTH - evaluate CKD-mineral bone disorder
- CBC - hemoglobin for anemia; iron, B12, folate
- Urinalysis + microscopy - hematuria, casts, proteinuria
- Serum and urine protein electrophoresis (SPEP/UPEP) in patients >35 with unexplained CKD to rule out multiple myeloma
- Autoimmune panel (ANA, anti-dsDNA) and hepatitis B/C, HIV if hematuria or proteinuria
Imaging
- Renal ultrasound (first-line): checks kidney size/symmetry, excludes obstruction and masses
- Bilaterally small kidneys = long-standing CKD
- Large kidneys: diabetic nephropathy (early), amyloidosis, HIV nephropathy, or PKD
Predicting Progression
The Kidney Failure Risk Equation (KFRE) - using age, sex, eGFR, and albuminuria - accurately predicts 2- and 5-year risk of requiring dialysis, validated in >720,000 patients from 30+ countries.
- Harrison's Principles of Internal Medicine 22e, p. 2438
- NKF Primer on Kidney Diseases, 8e, p. 529
Complications of CKD
These are the "AEIOU" of advanced CKD - all requiring regular monitoring:
1. Cardiovascular Disease
The #1 cause of death in CKD patients. Risk factors amplified in CKD include hypertension, sodium/volume retention, anemia, hyperphosphatemia, high prevalence of diabetes, and dyslipdemia. There is synergy between cardiovascular and kidney disease progression.
2. Anemia
- Caused primarily by decreased erythropoietin (EPO) production from damaged peritubular cells
- Iron deficiency frequently coexists
- Managed with iron repletion and erythropoiesis-stimulating agents (ESAs) (e.g., epoetin alfa, darbepoetin)
- Target Hb generally 10-11.5 g/dL (avoid >13 g/dL due to cardiovascular risk)
3. CKD-Mineral Bone Disorder (CKD-MBD)
A triad of interconnected problems:
- Hyperphosphatemia - impaired phosphate excretion → elevated FGF-23 → reduced calcitriol synthesis
- Hypocalcemia - due to low calcitriol + hyperphosphatemia
- Secondary hyperparathyroidism (SHPT) - PTH rises to correct calcium; causes high-turnover bone disease (osteitis fibrosa cystica)
- Treatment: dietary phosphate restriction → phosphate binders (calcium-based or non-calcium) → active vitamin D (calcitriol, paricalcitol) → calcimimetics (cinacalcet) for severe SHPT
4. Metabolic Acidosis
- Low bicarb from impaired tubular ammoniagenesis and reduced acid excretion
- Leads to bone dissolution (carbonate buffers H⁺), sarcopenia, and faster CKD progression
- Treated with oral sodium bicarbonate supplementation
- Multiple RCTs and a recent meta-analysis suggest treating acidosis may slow CKD progression
5. Hyperkalemia
- Impaired potassium excretion (high risk with RAAS inhibitors)
- Most serious electrolyte complication - can cause fatal arrhythmias
- Managed with dietary potassium restriction, diuretics, patiromer, or sodium zirconium cyclosilicate (SZC)
- NKF Primer on Kidney Diseases 8e; Harrison's 22e; Miller's Anesthesia 10e
6. Volume Overload and Hypertension
- Sodium/water retention worsens hypertension and cardiac preload
- Loop diuretics are key (thiazides lose efficacy at GFR <30)
7. Uremia (End-Stage)
- Accumulation of uremic toxins: encephalopathy, pericarditis, coagulopathy, immune dysfunction
- Indication for renal replacement therapy
Management
Disease-Modifying Therapies (Slow Progression)
1. RAAS Blockade - First Line
- ACE inhibitors or ARBs reduce intraglomerular pressure, proteinuria, and fibrosis
- Established benefit in diabetic and non-diabetic CKD with proteinuria (>300 mg/day)
- Do NOT combine ACEi + ARB (no added benefit, increased harm)
- NKF Primer; Brenner & Rector's The Kidney
2. SGLT2 Inhibitors - Major Advance
- Empagliflozin, dapagliflozin, canagliflozin - originally anti-diabetic, now proven renoprotective in diabetic AND non-diabetic CKD
- Reduce glomerular hyperfiltration, proteinuria, inflammation, and fibrosis
- Dapagliflozin (DAPA-CKD trial): reduced CKD progression and cardiovascular events even in non-diabetic CKD
- Now considered standard of care alongside RAAS blockade
- Harrison's Principles of Internal Medicine 22e; NKF Primer 8e
3. Finerenone (Non-steroidal MRA)
- Novel mineralocorticoid receptor antagonist (not spironolactone)
- FIDELIO and FIGARO trials (>13,000 patients): 18% relative risk reduction in CKD endpoint + 13% reduction in major adverse cardiovascular events in patients with diabetes and CKD
- NKF Primer on Kidney Diseases, 8e, p. 530
4. GLP-1 Receptor Agonists
- Semaglutide and liraglutide show additional cardiorenal benefit in diabetes + CKD
- Reduce albuminuria and slow GFR decline
Blood Pressure Control
- Target: <130/80 mmHg (KDIGO 2021) for most CKD patients with albuminuria
- Usually requires 2-4 antihypertensive agents (RAAS blocker + diuretic as backbone)
- A "J-curve" effect exists: very low systolic BP (<120 mmHg) may increase risk (ACCORD trial data)
- NKF Primer on Kidney Diseases, 8e, pp. 535-538
Glycemic Control
- HbA1c target ~7% in most diabetic CKD patients
- SGLT2 inhibitors preferred for dual glycemic + renal benefit
Dietary Management
- Protein restriction (0.6-0.8 g/kg/day) may reduce hyperfiltration and proteinuria
- Low phosphate, low potassium diet in stages 4-5
- Low sodium (<2 g/day) to control BP and volume
- Avoid nephrotoxins: NSAIDs, contrast where possible
Management by Stage
| Stage | GFR | Key Actions |
|---|---|---|
| 1-2 | ≥60 | Control diabetes/HTN, maximize RAAS+SGLT2i, reduce proteinuria |
| 3 | 30-59 | Above + screen for anemia, CKD-MBD, acidosis, neuropathy; KFRE risk assessment |
| 4 | 15-29 | Above + refer to nephrologist, prepare for renal replacement therapy (AV fistula creation, PD catheter) |
| 5 | <15 | Initiate dialysis if uremic symptoms, uncontrolled hyperkalemia/acidosis/volume; or GFR <10 |
Renal Replacement Therapy (ESKD)
Indications for dialysis initiation:
- Uremic symptoms (encephalopathy, pericarditis, bleeding)
- Hyperkalemia unresponsive to conservative measures
- Persistent volume overload despite diuretics
- Refractory metabolic acidosis
- eGFR <10 mL/min/1.73m² (not an absolute trigger - symptoms matter)
Modalities:
- Hemodialysis (HD): 3x/week, 3-4h sessions; most common in developed world
- Peritoneal dialysis (PD): home-based, daily; comparable outcomes but less used
- Kidney transplantation: best outcomes - superior survival compared to dialysis; pre-emptive transplant (before dialysis) is ideal
Deaths in ESKD are mainly from cardiovascular disease and infections.
- Harrison's Principles of Internal Medicine 22e, pp. 2437-2440
Key Points Summary
| Aspect | Key Fact |
|---|---|
| Definition | Kidney damage or GFR <60 for ≥3 months |
| Top causes | Diabetes, hypertension, glomerulonephritis |
| Most dangerous complication | Cardiovascular disease (leading cause of death) |
| #1 drug class for progression | RAAS inhibitors (ACEi/ARB) |
| Newer game-changer | SGLT2 inhibitors (benefit even in non-diabetic CKD) |
| Newest approved agent | Finerenone (FIDELIO/FIGARO trials) |
| When to refer | eGFR <30; prepare for RRT at eGFR <20 |
| Dialysis trigger | Uremic symptoms, not a specific GFR number |
| Best long-term outcome | Kidney transplantation |
Sources:
- NKF Primer on Kidney Diseases, 8e (pp. 528-560)
- Harrison's Principles of Internal Medicine 22e (pp. 2437-2445)
- Brenner and Rector's The Kidney, 2-Volume Set
- Textbook of Family Medicine 9e (pp. 1191-1192)
- Comprehensive Clinical Nephrology, 7th Edition
This is a shared conversation. Sign in to Orris to start your own chat.