Write about types of Offences. Difference between cognizable and Non-cognizable offences. Provide visual infographic for my exam on for forensic medicine University indetail from narayan Reddy latest edition
Medical forensic exam infographic titled "Types of Offences in Forensic Medicine" based on Narayan Reddy textbook. Include sections: 1) Classification of Offences with two main branches - Cognizable vs Non-Cognizable, and Bailable vs Non-Bailable; 2) Cognizable Offence (defined as serious crimes where police can arrest without warrant and investigate without court permission - murder, rape, robbery, dacoity, kidnapping) vs Non-Cognizable Offence (less serious crimes where police cannot arrest without warrant and need court permission to investigate - cheating, fraud, defamation, assault); 3) Bailable Offence (accused has right to bail) vs Non-Bailable Offence (bail granted only by court); 4) A comparison table with columns: Feature, Cognizable, Non-Cognizable - rows for Warrant needed, Police power to arrest, Investigation authority, Bail nature, Examples; 5) Compoundable vs Non-Compoundable offences. Use a professional blue and orange color scheme with clear headers, icons, arrows, and exam-ready formatting. Include BNSS/CrPC reference notes.
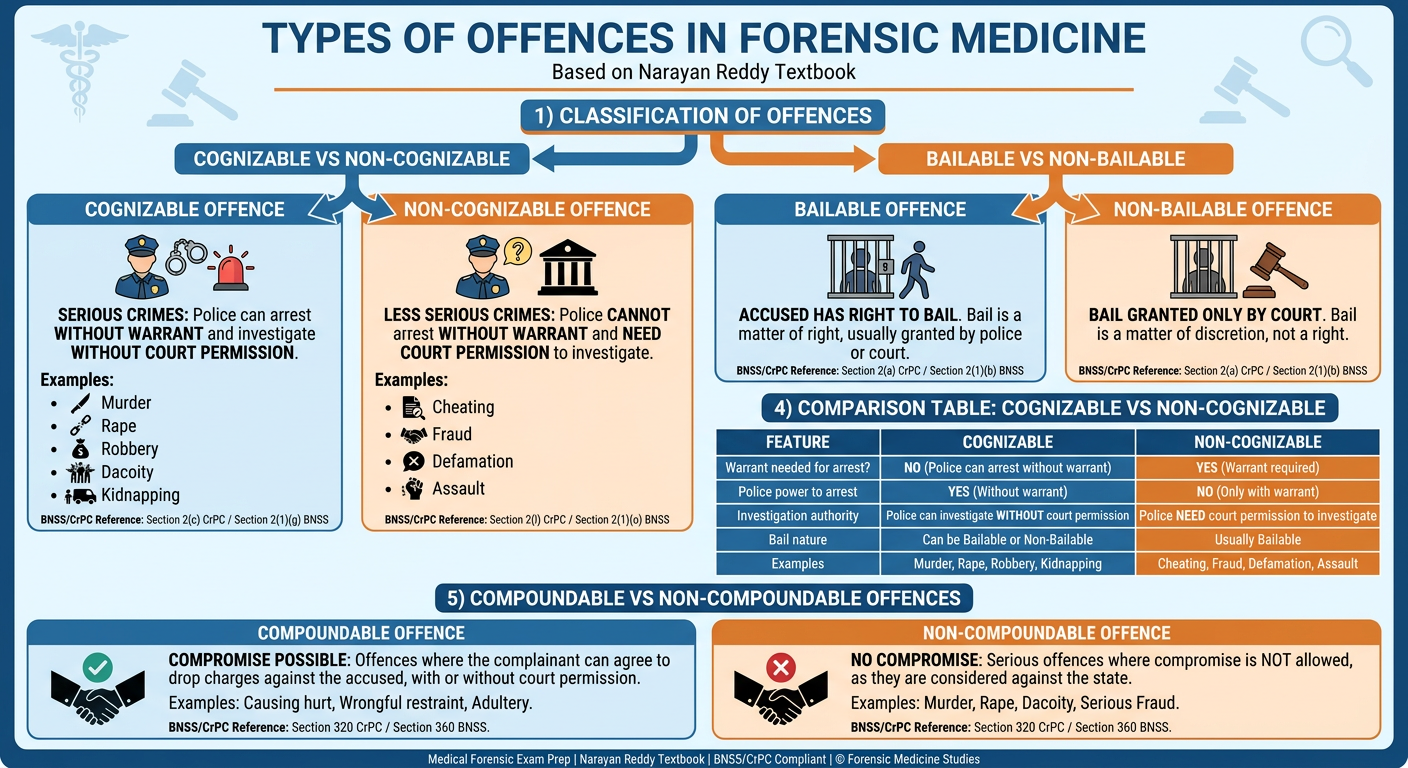
Types of Offences - Forensic Medicine (Narayan Reddy)
Definition of Offence
Classification of Offences
- Cognizable vs Non-Cognizable
- Bailable vs Non-Bailable
- Compoundable vs Non-Compoundable
- Summons Case vs Warrant Case
1. Cognizable vs Non-Cognizable Offences
Cognizable Offence
| Feature | Details |
|---|---|
| Definition | A serious offence in which a police officer can arrest the accused without a warrant and can begin investigation without prior permission of a Magistrate |
| Legal Basis | First Schedule of BNSS (formerly Cr.P.C.) |
| Arrest | Police can arrest without warrant |
| Investigation | Police can investigate without Magistrate's order |
| Bail | Generally non-bailable |
| Examples | Murder, culpable homicide, rape, robbery, dacoity, kidnapping, dowry death, rioting, unnatural offences, hurt by dangerous weapon, acid attack |
Non-Cognizable Offence
| Feature | Details |
|---|---|
| Definition | A less serious offence in which police cannot arrest without a warrant and cannot investigate without Magistrate's permission |
| Legal Basis | First Schedule of BNSS |
| Arrest | Police require a warrant from Magistrate |
| Investigation | Requires Magistrate's prior permission (Section 155, Cr.P.C. / BNSS) |
| Bail | Generally bailable |
| Examples | Cheating, fraud, defamation, simple hurt, assault, mischief, forgery of documents (less serious) |
Comparison Table: Cognizable vs Non-Cognizable
| Feature | Cognizable | Non-Cognizable |
|---|---|---|
| Seriousness | Serious / Grave | Less serious |
| Arrest without warrant | Yes (Police can) | No (Warrant required) |
| Investigation without court order | Yes | No (Need Magistrate order) |
| Bail | Non-bailable (generally) | Bailable (generally) |
| FIR filing | Police must register FIR | Police may refuse; only complaint to Magistrate |
| Trial court | Sessions Court / Magistrate | Magistrate Court |
| Examples | Murder, rape, robbery | Defamation, cheating, simple hurt |
2. Bailable vs Non-Bailable Offences
Bailable Offence
- The accused has a right to demand bail as a matter of right.
- Bail cannot be refused by police or Magistrate.
- These are generally less serious offences.
- Examples: Simple hurt, mischief, negligent acts.
Non-Bailable Offence
- Bail is not a right - it can only be granted by the court at its discretion.
- Police officer cannot grant bail for non-bailable offences.
- Examples: Murder, rape, dacoity, kidnapping, dowry death.
- Under Section 437, BNSS (S. 437, Cr.P.C.) - Magistrate may grant bail with conditions.
- Under Section 439, BNSS (S. 439, Cr.P.C.) - High Court / Sessions Court can grant bail.
3. Compoundable vs Non-Compoundable Offences
Compoundable Offence
- The complainant (victim) and accused can arrive at a settlement (compromise).
- The complainant can withdraw the complaint with the court's permission.
- Two types:
- With Court's permission: e.g., causing grievous hurt
- Without Court's permission: e.g., simple hurt, defamation (private matters)
Non-Compoundable Offence
- Cannot be settled between the parties.
- The state continues prosecution even if the victim forgives.
- Examples: Murder, rape, dacoity - these are crimes against the state, not just the individual.
4. Summons Case vs Warrant Case
| Feature | Summons Case | Warrant Case |
|---|---|---|
| Punishment | Imprisonment up to 2 years | Imprisonment more than 2 years |
| Procedure | Simpler, quicker | More elaborate |
| Accused summoned by | Summons | Warrant |
Key Points for Forensic Medicine Exam (Narayan Reddy Points)
- Cognizable offence is listed as a short note topic in Narayan Reddy (Short Notes section, Block 1).
- All medicolegal cases (MLCs) seen by doctors - injuries due to assault, rape, acid attack, dowry death, unnatural death - involve cognizable offences and require FIR registration.
- The doctor examining a victim of rape or assault is dealing with evidence in a cognizable, non-bailable offence - this makes accurate documentation critical.
- FIR (First Information Report) is mandatory in cognizable offences - the doctor may be the first person to suspect foul play and must inform police promptly.
- Under BNSS 2023 (new law replacing Cr.P.C.), these definitions and schedules remain essentially the same but the section numbers have changed.
Quick Mnemonics
- Cognizable = Constable can arrest (no warrant needed)
- Non-cognizable = Need warrant
- Bailable = Bail as a right
- Non-bailable = Not automatic - court decides
Describe legal importance of Documentation / Preservation of Medico Legal Records. Provide visual infographic for my exam from latest edition of forensic medicine narayan Reddy in detail for my university
Detailed exam-ready forensic medicine infographic titled "Legal Importance of Documentation and Preservation of Medico-Legal Records" based on Narayan Reddy textbook. Divided into 6 clear sections with icons and color coding: 1) OBJECTIVES OF MEDICAL RECORDS - 7 bullet points: basis for patient care, documentation for reimbursement, medical education/research, communication between doctors, legal protection of patient/hospital/doctor, follow-up and drug evaluation, professional negligence and insurance claims; 2) MANDATORY DOCUMENTATION - numbered list: name/age/sex/address, date-time of visit, informed consent, history, examination findings, diagnostic reports, consultant opinion, diagnosis, progress notes, treatment details, discharge condition; 3) GOLDEN RULES - Accurate, Chronological, Factual, Complete, No Tampering, Corrections with single line + date + signature; 4) PRESERVATION PERIODS - table: Routine records = 3 years, Medico-legally important = 10 years, Public interest records = 50 years, Confidential individual records = 100 years; 5) WOUND CERTIFICATE / MLC - Accident Register mandatory, sealed copy to police, copy retained by doctor, serial number, date/time/place, preliminary particulars, injury type/size/location/age/weapon; 6) LEGAL CONSEQUENCES - Tampering leads to large compensation awards, good notes support doctor in court, confidentiality rules, patient's right to records. Use teal green, dark blue and orange color scheme. Professional clean medical layout.
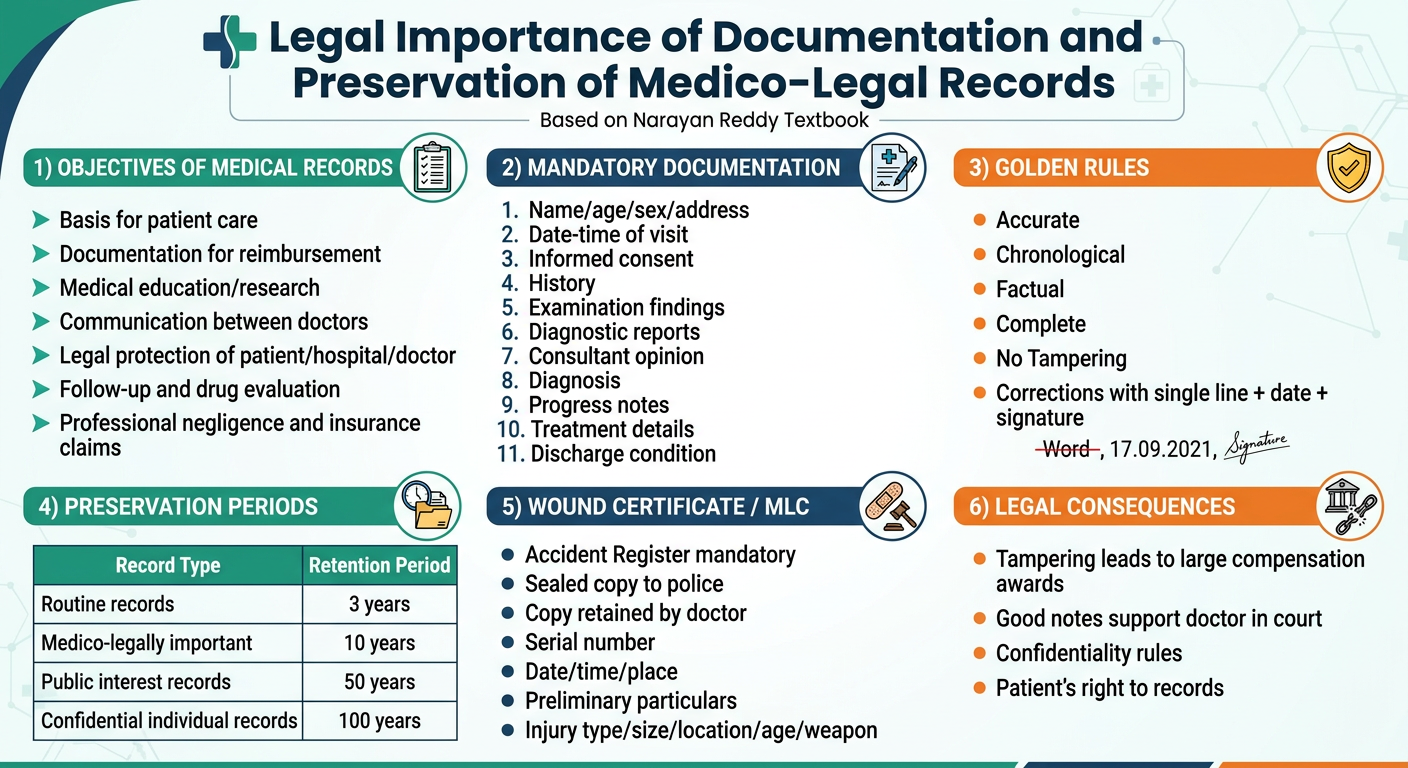
Legal Importance of Documentation / Preservation of Medico-Legal Records
The Essentials of Forensic Medicine and Toxicology, 36th Edition (Narayan Reddy, 2026) - Chapter 3
What are Medical Records?
Objectives / Purposes of Medical Records (Narayan Reddy)
- To serve as the basis for patient's care and continuity of evaluation and treatment.
- To serve as documentation for reimbursement (insurance, etc.).
- To provide data for medical education and clinical research.
- To document communication between the treating doctor and other healthcare professionals contributing to care.
- To protect the legal interests of the patient, the hospital, and the practitioner responsible for patient care.
- To assist in follow-up of patients, evaluation of drug therapy, and cost accounting.
- Medical records may be required in cases of:
- Professional negligence
- Claims under health and accident insurance
- Life insurance policies
- Disability policies
- Accidental deaths
- Workmen's Compensation Act
- Traffic accidents
Mandatory Information to be Documented
| Sr. No. | Mandatory Entry |
|---|---|
| 1 | Name, father's name, age, sex, occupation, address |
| 2 | Date and hour of visiting doctor/nursing home/hospital |
| 3 | Evidence of informed consent (preferably in local language) |
| 4 | Brief history of present illness, relevant past and family history |
| 5 | Findings of general physical and systemic examination (objective + subjective) |
| 6 | Diagnostic aids used and reports received |
| 7 | Date and hour of consultation with details and opinion of consultant |
| 8 | Clinical impression with provisional and final diagnosis |
| 9 | Progress notes including clinical observations |
| 10 | Instructions given to patient including diet |
| 11 | Complications, if any |
| 12 | Notations about lack of cooperation by patient |
| 13 | Failure of patient to follow advice or keep appointments |
| 14 | Details of treatment, procedures, or operations recommended/performed |
| 15 | In emergency cases - specific clinical data noted periodically |
| 16 | In in-patients - condition at discharge (cured / relieved / referred / discharged on request / absconded) |
Golden Rules for Maintaining Medical Records
"Accurate, Appropriate, Chronological, Factual, Relevant and Complete" - Narayan Reddy
- No tampering - Nothing should be altered, deleted, substituted, or added.
- If tampering is done, the patient may be awarded large sums even if there was no negligence.
- If a correction must be made - draw a single line through the word, write correct information above it with the date and signature/initials of the person making the change + reason for change.
- Omission of essential details may cast doubt on the truthfulness of the witness (doctor).
- Good notes have great value when handing a patient over to another doctor and in meeting any criticism.
- When there is conflict of evidence, the court will attach importance to notes written at the time of examination.
- If a patient refuses advice, this fact should be recorded in writing.
Preservation Periods for Medical Records (Medical Council Regulations)
| Type of Record | Period of Preservation |
|---|---|
| Routine in-patient / out-patient records | 3 years from the date of completion |
| Medico-legally important records | 10 years (after which, can be destroyed after making index and summary) |
| Public interest records | Transferred to public record library after 50 years |
| Records involving individual confidentiality | Released to public only after 100 years |
Rights and Confidentiality Rules
- The patient has the right to know what is in his/her records.
- Patient is entitled to a brief report of hospital record on discharge.
- Next of kin can get the record in case of patient's death.
- The hospital must maintain confidentiality of records.
- Police do not have a right to demand medical records except when there is statutory provision (e.g., court order).
- Records cannot be used in educational conferences, clinics, or publications without the patient's consent.
- Hospitals may use medical records (without patient consent) for statistical purposes and quality of care determinations.
- X-ray plates are the property of the treating doctor - the patient buys the skill and treatment, not the X-ray films.
- If disclosure would be harmful to the patient (therapeutic/professional discretion), the hospital can avoid issuing the record.
Wound Certificate and Accident Register (Medico-Legal Records)
Accident Register
- Maintained in all hospitals including clinics and nursing homes.
- All details of examination of injured persons (whether admitted or OPD) must be entered.
- It is a confidential record and kept in safe custody of the medical officer.
- Must be produced in a Court of law if asked for.
Wound Certificate Format - Mandatory Entries
- Serial number of case
- Name, age, sex, address of injured person
- Father's / guardian's name
- Date, time, and place of examination
- Name and number of accompanying police constable and police station
- Names of accompanying persons with addresses
- Brief statement of injured person about nature of incident - recorded as "alleged by the patient"
- Two identification marks
- Stature, body weight, development of victim
- Consent of person for examination; if serious - dying declaration to be recorded
- Type of each injury - abrasion, contusion, incised wound, lacerated wound, stab wound, burns, fracture, dislocation
- Size - length x breadth x depth (in cms)
- Location - on the body surface with exact anatomical site
- Age of injury - fresh, recent, or old
- Weapon likely to have caused the injury
- Whether injury is simple or grievous (to guide the investigating officer)
- General condition of the patient
- One copy sent to investigating police officer in sealed cover, other copy retained for future reference.
Medical Council of India / NMC Regulations on Medical Records (Narayan Reddy)
- Maintain a register of medical certificates giving full details, with signature of patients and at least one identification mark.
- Maintain medical records pertaining to indoor patients for a period of 3 years from the date of completion.
- Medico-legally important records preserved for 10 years.
Legal Consequences of Poor Documentation
| Situation | Legal Consequence |
|---|---|
| Tampering with records | Large compensation awarded to patient even without negligence |
| Omission of essential details | Doctor's credibility questioned in court |
| Poor / incomplete notes | Doctor's version rejected if contradicted by plaintiff/witnesses |
| Refusal to produce accident register | Contempt of court |
| Unauthorized disclosure | Breach of confidentiality; professional misconduct |
| Failure to maintain records for minimum period | Violation of MCI/NMC regulations |
Summary of Legal Importance (Key Points for Exam)
- Medical records are the only objective evidence of what was done clinically.
- In negligence cases, courts rely almost entirely on records - "If it's not written, it wasn't done."
- The Accident Register is a primary legal document in medico-legal cases.
- Wound certificate guides the police and courts on the nature and gravity of assault.
- Records protect both the patient's interests (fair trial, compensation) and the doctor's interests (defence against false claims).
- Preservation for defined periods ensures records are available for litigation, which may arise years later.
- Any tampering with records is one of the gravest professional misconduct acts and can be penalised severely.
What is the First Information Report? Write about documentary evidence. Provide a visual infographic for this question as a 5 marks in detail in a an attractive manner from narayan Reddy latest edition
Attractive forensic medicine exam infographic for 5 marks question on "First Information Report (FIR) and Documentary Evidence" from Narayan Reddy textbook. Clean, colorful, professional layout with 4 main sections: SECTION 1 - "FIRST INFORMATION REPORT (FIR)" with dark blue header: Definition box "Written complaint given to police officer about a cognizable offence", Legal basis: Section 173 BNSS (formerly S.154 CrPC), 6 key features as icon bullets: 1) Only for cognizable offences, 2) Given to officer in charge of police station, 3) Recorded in writing and read to informant, 4) Signed by informant, 5) Copy given to informant free of cost, 6) Sets criminal law in motion; SECTION 2 - "DOCUMENTARY EVIDENCE" with teal header: Definition "All documents produced for inspection of the court [Sections 56-92 BSA]", Then 3 Types in colored boxes: (A) Medical Certificates - orange box: ill-health/insanity/age/death, only by qualified RMP, retain duplicate 2 years, false certificate punishable S.234 BNS; (B) Medico-Legal Reports - green box: prepared on request of IO, two parts: Facts observed + Opinion, written in duplicate, first copy to IO second retained; (C) Dying Declaration - purple box: statement of dying person about cause of death, Section 26 BSA, recorded by magistrate or doctor if magistrate not available; SECTION 3 - small box: Primary vs Secondary Evidence comparison; SECTION 4 - small "Oral Evidence" vs "Documentary Evidence" comparison. Color scheme: navy blue, teal, orange, white. Exam-ready clean layout with bold headings.
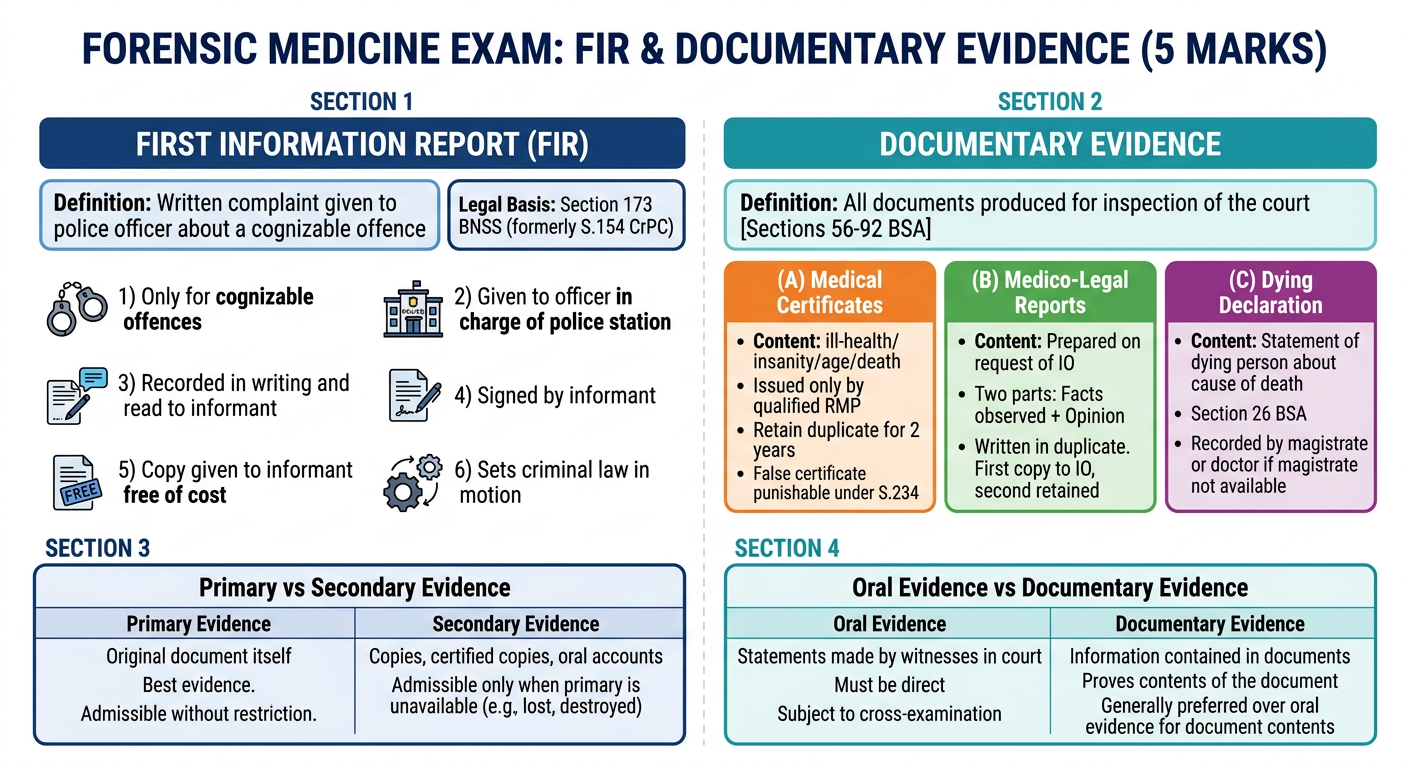
First Information Report (FIR) & Documentary Evidence
The Essentials of Forensic Medicine and Toxicology, 36th Edition - K.S. Narayan Reddy (2026)
FIRST INFORMATION REPORT (FIR)
Definition
Key Features of FIR
| Feature | Details |
|---|---|
| Applicability | Only for cognizable offences (murder, rape, robbery, dacoity, dowry death, etc.) |
| Who gives it | Any person - victim, witness, or even police officer suo motu |
| Recording | Must be reduced to writing by the officer in charge of the police station |
| Reading back | Read over and explained to the informant in the language he understands |
| Signature | Signed or thumb impressed by the informant |
| Free copy | A copy is given to the informant free of cost |
| Registration | Entered in the General Diary / Station House Diary with a unique crime number |
| Legal effect | Sets the criminal law in motion - police investigation begins immediately |
Importance of FIR in Forensic Medicine
- Triggers medical examination - once FIR is registered, police send the victim/accused to a doctor with a requisition letter.
- Acts as the primary document linking a medicolegal case to the criminal justice system.
- Provides the nature of the alleged offence to the doctor - guiding what type of examination to conduct (e.g., rape examination vs. assault).
- In non-cognizable offences (Section 2(l), BNSS), the injured person may go directly to the doctor OR file an affidavit before a Magistrate who then sends him for examination (Section 35, BNSS / S.41, Cr.P.C.).
- The FIR is a public document and is admissible in court.
FIR vs. Non-Cognizable Report (NCR)
| Feature | FIR (Cognizable) | NCR (Non-Cognizable) |
|---|---|---|
| Offence type | Serious / grave | Less serious |
| Police action | Can investigate immediately | Needs Magistrate's order |
| Arrest | Without warrant | Requires warrant |
| Medical examination | Police sends victim to doctor | Victim goes directly to doctor |
MEDICAL EVIDENCE
- All statements which the court permits or requires to be made before it by witnesses in relation to matters of fact under inquiry.
- All documents produced for the inspection of the court [Section 2, BNS].
- Evidence of an eyewitness is positive; evidence of a doctor/expert is only an opinion which is corroborative.
Types of Evidence
EVIDENCE
├── Documentary Evidence ← (our topic)
└── Oral Evidence
├── Direct
├── Indirect / Circumstantial
└── Hearsay
DOCUMENTARY EVIDENCE (Narayan Reddy - 3 Types)
- Primary evidence = The document itself produced for inspection of the court [Section 208, BNS / Section 59, BSA]
- Secondary evidence = Certified copies, copies made from original by mechanical processes, oral account of document contents [Section 58, BSA]
Type 1 - MEDICAL CERTIFICATES
| Point | Details |
|---|---|
| Definition | Documents issued by a registered medical practitioner referring to ill-health, insanity, age, or death |
| Validity | Accepted in court only when issued by a qualified registered medical practitioner (RMP) |
| Ill-health certificate | Must contain exact nature of illness; issue for not more than 15 days; re-examine and reissue after 15 days |
| No back-dating | Do not give fitness certificate on an advanced or back date |
| Addressee | Must address a specific person (employer, headmaster, principal, etc.) |
| Patient signature | Signature or left thumb impression of patient must be taken |
| Identification marks | Two identification marks should be noted |
| Duplicate retention | Doctor must retain a duplicate of certificate issued for 2 years |
| Death certificate | Doctor legally bound to issue it FREE of charge if attending the last illness; must inspect body; must not be issued if foul play suspected |
| False certificate | Punishable under Section 234, BNS (formerly S. 197, I.P.C.) |
Type 2 - MEDICO-LEGAL REPORTS (MLR)
| Point | Details |
|---|---|
| Definition | Reports prepared by a doctor on the request of the Investigating Officer (IO) usually in criminal cases |
| Occasions | Assault, rape, murder, accident, etc. |
| Two parts | (1) Facts observed on examination (objective + relevant negative findings); (2) Opinion drawn from facts |
| Admissibility | Will NOT be admitted as evidence unless the doctor attends court and testifies under oath |
| Date/time/place | Must be recorded along with name of individuals who identified the person/body |
| Language | Avoid exaggerated terms, technical jargon as far as possible |
| Bias | Opinion based only on facts observed personally - not on information from other sources |
| Format | Clear, concise, complete, legible; sign/initial at bottom of each page |
| Copies | Written in duplicate - first copy to investigating officer, second copy retained by doctor |
Type 3 - DYING DECLARATION
| Point | Details |
|---|---|
| Definition | Statement made by a person who is in danger of dying about the cause or circumstances of his impending death |
| Legal basis | Section 26, BSA (formerly Section 32, Indian Evidence Act) |
| Latin | "Nemo moriturus praesumitur mentire" - "A man will not meet his Maker with a lie in his mouth" |
| Recorded by | Magistrate (preferred); doctor (if Magistrate not available and death is imminent) |
| Condition | Person must be of sound mind at the time of making the declaration |
| No oath needed | It is admissible without oath or cross-examination |
| Medical role | Doctor must certify that the patient was conscious and mentally fit to make the declaration |
| Legal standing | Can form the sole basis of conviction if it is true and voluntary |
Summary Table for 5-Mark Answer
| Category | FIR | Documentary Evidence |
|---|---|---|
| Definition | First written info to police about cognizable offence | All documents produced for inspection of court |
| Legal section | S.173 BNSS | S.56-92 BSA |
| Types | Single type | 3 types: Medical Certificates, MLR, Dying Declaration |
| Who prepares | Police officer | Registered Medical Practitioner |
| Admissibility | Public document, directly admissible | MLR needs doctor's oral testimony in court |
| Forensic relevance | Triggers medical examination of victim/accused | Forms evidence base for prosecution/defense |
Key Points for Exam (5-marker)
- FIR applies only to cognizable offences and sets criminal proceedings in motion.
- Documentary evidence in forensic medicine has 3 types - remember: "MCM" (Medical Certificates, MLR, Dying Declaration).
- Medical certificates must be preserved for 2 years (duplicate); a false certificate is punishable under S.234 BNS.
- MLR must be written in duplicate - first to IO, second retained by doctor - and requires doctor's court attendance for admissibility.
- Dying declaration is the most powerful of the three - can convict even without other evidence.