Labor position and role of tens in pain
15 marks question
maternal position during labor role advantages obstetrics 15 marks
https://pmc.ncbi.nlm.nih.gov/articles/PMC6839002
Labor Position and Role of TENS in Pain Relief
PART A: MATERNAL POSITIONS IN LABOR
Introduction
Classification of Positions
| Position | Description |
|---|---|
| Standing / Ambulating | Trunk erect, gravity-assisted |
| Sitting | Trunk tilted >45° to horizontal (chair, bed edge, birth ball) |
| Squatting | Trunk lowered from standing with support |
| Kneeling | On knees with trunk upright or on all-fours |
| Position | Description |
|---|---|
| Lateral (Sims') | Lying on side, upper leg toward chest |
| Supine / Semi-recumbent | Lying flat or trunk <45° to horizontal |
| Lithotomy | Supine with legs elevated in stirrups |
Role/Advantages of Positions During Labor
First Stage of Labor
-
Upright & ambulating positions
- Harness the force of gravity to aid fetal head descent and engagement.
- Improve uterine contraction efficiency and frequency.
- Decrease the duration of the first stage.
- Reduce the need for oxytocin augmentation.
- Associated with less labor pain compared to supine.
-
Lateral (left lateral decubitus)
- Relieves aortocaval compression by the gravid uterus, improving placental blood flow and fetal oxygenation.
- Useful when continuous fetal monitoring is required and ambulation is not possible.
- Recommended after epidural analgesia placement.
-
All-fours / hands-and-knees
- Particularly effective when the fetus is in the occiput posterior (OP) position - the anterior position allows gravity to encourage spontaneous rotation of the fetal head.
- Reduces back pain in labor (back labor).
- "Any maternal position that causes her to curl forward from the hips is felt to be helpful" for OP rotation (Pfenninger & Fowler).
-
Squatting
- Widens the pelvic outlet (increases bi-ischial diameter by ~1-2 cm).
- Beneficial when fetal head is low and pushing is imminent.
Second Stage of Labor
-
Squatting
- Shortens the second stage by ~9 minutes compared to supine in both primiparas and multiparas.
- Utilizes gravity and maximizes pelvic outlet dimensions.
- Disadvantage: increased risk of obstetric anal sphincter injury (OASIS) due to difficulty controlling extension of the fetal head.
-
Sitting on birth seat
- Significantly shorter second stage compared to lateral, supine, and standing positions (RCT evidence).
- Less synthetic oxytocin needed for augmentation.
-
Lithotomy
- Traditional in many hospital settings.
- Allows the provider good perineal visibility and access.
- Loses the advantage of gravity; associated with more perineal trauma.
- Risk of supine hypotension syndrome (aortocaval compression).
-
Lateral (Sims')
- Useful for slow, controlled delivery of the fetal head.
- Good when perineal protection is the priority.
- Less effective use of gravity.
-
Kneeling / all-fours
- Used to manage shoulder dystocia (Gaskin maneuver).
- Helps rotate a persistent OP fetus.
Management of Persistent Occiput Posterior (OP) Position
- The OP position prolongs labor by ~1 hour in multiparas and ~2 hours in nulliparas.
- Position changes to encourage rotation: squatting, ambulating, hands-and-knees, lateral Sims', or back-arched positions.
- Manual rotation if positional changes fail: mother in lithotomy, lateral Sims', or hands-and-knees; hand placed in posterior pelvis behind occiput; rotation during a contraction while mother pushes. (Pfenninger & Fowler)
Supine Hypotension Syndrome (Aortocaval Compression)
- Supine position allows the gravid uterus to compress the inferior vena cava and aorta, reducing venous return and uteroplacental perfusion.
- Can cause fetal asphyxia and maternal hypotension.
- Prevention: Avoid the supine position; use left lateral tilt (15°) during all monitoring and procedures.
PART B: ROLE OF TENS IN LABOR PAIN
What is TENS?
Mechanism of Action
-
Gate Control Theory (primary mechanism)
- Pain signals (nociception) are transmitted via small, slow C-fibers and Aδ-fibers to the dorsal horn (T-cells), which convey information to higher brain centers.
- TENS activates large-diameter, fast Aβ fibers, which stimulate inhibitory interneurons in the substantia gelatinosa of the dorsal horn.
- These interneurons "close the gate" - they presynaptically inhibit the transmission of pain impulses to the brain.
- "In a mechanism called the gate control theory, sensory inputs from large-diameter nonpain Aβ fibers reduce pain transmission through the dorsal horn. Thus, TENS devices work to reduce chronic pain by activating Aβ fibers." - Neuroanatomy through Clinical Cases
-
Endogenous Opioid Release
- Low-frequency TENS (<10 Hz) stimulates the release of endorphins and enkephalins from the periaqueductal gray, rostral ventromedial medulla, and spinal cord dorsal horn.
- These endogenous opioids modulate pain at central and spinal levels.
-
Local Vasodilation
- Direct local vasodilation may reduce relative ischemia in the painful area (e.g., uterine ischemia contributing to labor pain), thereby reducing pain.
TENS Parameters
| Parameter | Low-frequency TENS | High-frequency TENS |
|---|---|---|
| Frequency | <10 Hz (acupuncture-like) | 80-150 Hz (conventional) |
| Pulse width | Long (~200 ms) | Short (~50 ms) |
| Mechanism | Endorphin release | Gate control |
| Intensity | High (muscle contraction) | Low-moderate (paresthesia, no motor) |
| Fiber target | Small unmyelinated | Large myelinated |
- Conventional settings for labor: high-frequency, narrow pulse width, intensity set to strong paresthesia without motor stimulation.
- Electrodes placed over the lower back (T10-L1 dermatomes) - the primary pain pathway for first-stage labor (uterine contractions).
Application in Labor
- Indication: Obstetric pain in labor (after the first trimester).
- Electrode placement: Lower back bilaterally, at the level of T10-L1 for first-stage pain; additional sacral (S2-S4) placement for second-stage perineal pain.
- TENS allows the mother to self-administer stimulation, boosting her sense of control over labor pain.
- Can be used alongside other non-pharmacological methods (hydrotherapy, Lamaze, massage, aromatherapy).
Evidence and Effectiveness in Labor
- Results of studies using TENS in labor are inconsistent.
- A systematic review and meta-analysis concluded: "Labor pain does not appear to be lessened by TENS, nor does TENS lower the use of other analgesic modalities." (Barash, Clinical Anesthesia, 9e)
- However, TENS may improve maternal satisfaction and sense of control, and may reduce anxiety.
- It is safe, non-invasive, and carries no pharmacological risk to the fetus, making it an attractive first-line option in non-pharmacological pain management.
Contraindications to TENS in Obstetrics
- First-trimester pregnancy (absolute)
- Patients with demand-type pacemakers
- Known cardiac dysrhythmias
- Undiagnosed pain syndrome
- Mentally incompetent or uncooperative patients
- Application over carotid sinuses, chest (cardiac history), head/neck (epilepsy history), eyes, or broken skin
Other Non-Pharmacological Methods (Context)
| Method | Evidence |
|---|---|
| Continuous labor support (doula) | Strong evidence - shorter labor, fewer operative deliveries |
| Hydrotherapy (water baths) | Less pain, less analgesia use |
| Acupuncture / acupressure | Modestly lower pain scores (meta-analysis, 13 trials) |
| Intradermal water injections | Inconsistent; no robust evidence for low back pain |
| Hypnosis | Promising but insufficient trials |
| TENS | Inconsistent; may improve satisfaction but not pain scores |
| Lamaze / psychoprophylaxis | Reduces anxiety; evidence on pain sensation unclear |
Summary Table
| Aspect | Labor Position | TENS |
|---|---|---|
| Mechanism | Gravity, pelvic mechanics, fetal rotation | Gate control theory, endorphin release, vasodilation |
| Main benefit | Shortened labor, improved fetal oxygenation, OP rotation | Non-pharmacological pain modulation, maternal control |
| Best stage | 1st stage: upright/ambulating; 2nd stage: squatting/sitting | Both stages; mainly 1st stage back pain |
| Key risk | Supine: aortocaval compression; Squatting: OASIS | Contraindicated in 1st trimester, pacemaker patients |
| Evidence | Moderate-good (RCT data for upright positions) | Inconsistent; does not reduce analgesic consumption |
- Barash, Cullen & Stoelting's Clinical Anesthesia, 9e - Nonpharmacologic Methods of Labor Analgesia
- Pfenninger & Fowler's Procedures for Primary Care, 3e - TENS technique and obstetric application
- Neuroanatomy through Clinical Cases, 3e - Gate control theory of pain
- PMC6839002 - Review and comparison of common maternal positions during the second stage of labor
Diagrams
Medical education diagram showing common maternal positions during labor. Include labeled illustrations of: 1) Upright/Standing position, 2) Sitting on birth ball, 3) Squatting position, 4) All-fours/Hands-and-knees position, 5) Left lateral (Sims') position, 6) Lithotomy position. Each position should be a clean anatomical side-view sketch with arrows showing gravity direction where relevant. Clean medical textbook style with white background, clear labels.
Medical diagram showing TENS (Transcutaneous Electrical Nerve Stimulation) electrode placement on a pregnant woman's lower back for labor pain relief. Show a posterior view of the back with 4 electrode pads placed bilaterally at T10-L1 level (upper pair) and S2-S4 level (lower pair near sacrum). Label the spinal levels T10, L1, S2, S4, and indicate "First stage pain" for upper electrodes and "Second stage pain" for lower electrodes. Include a small TENS generator unit connected by wires. Clean medical illustration style.
DIAGRAM 1 — Gate Control Theory of Pain (Kandel's Principles of Neural Science)
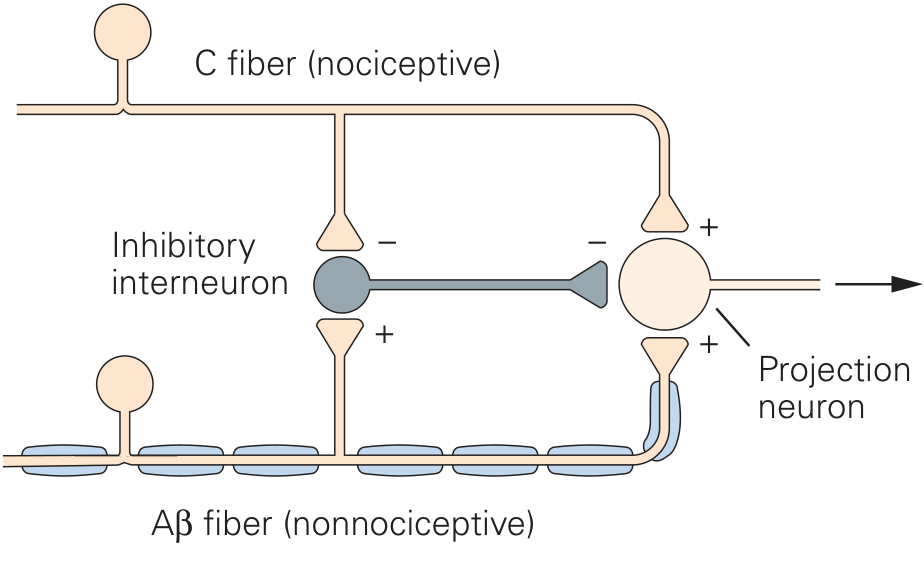
DIAGRAM 2 — Gate Control Theory (Spinal Cord Cross-Section - Neuroscience: Exploring the Brain)
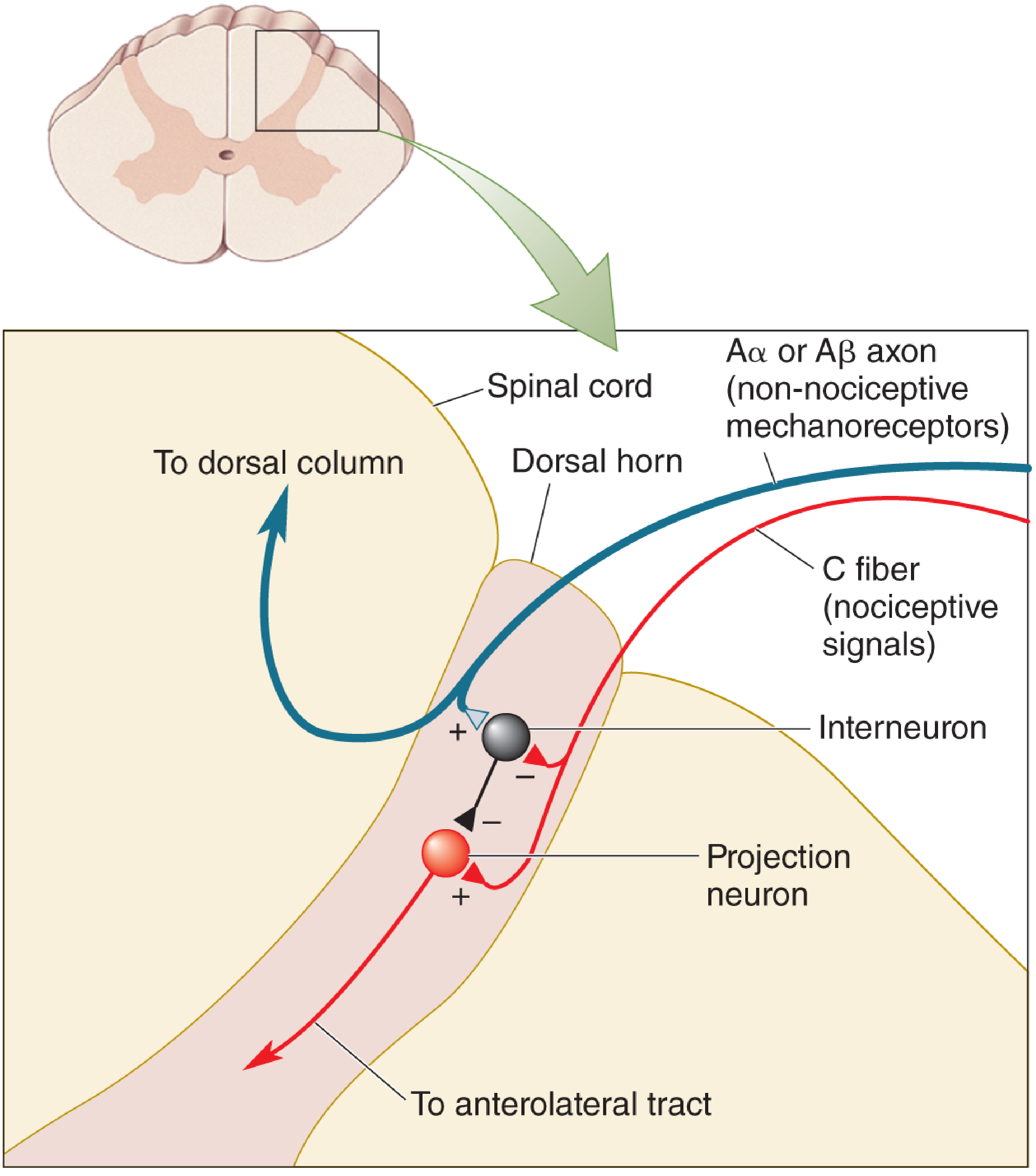
DIAGRAM 3 — Descending Pain Modulation Pathway (PAG → Raphe Nuclei → Dorsal Horn)
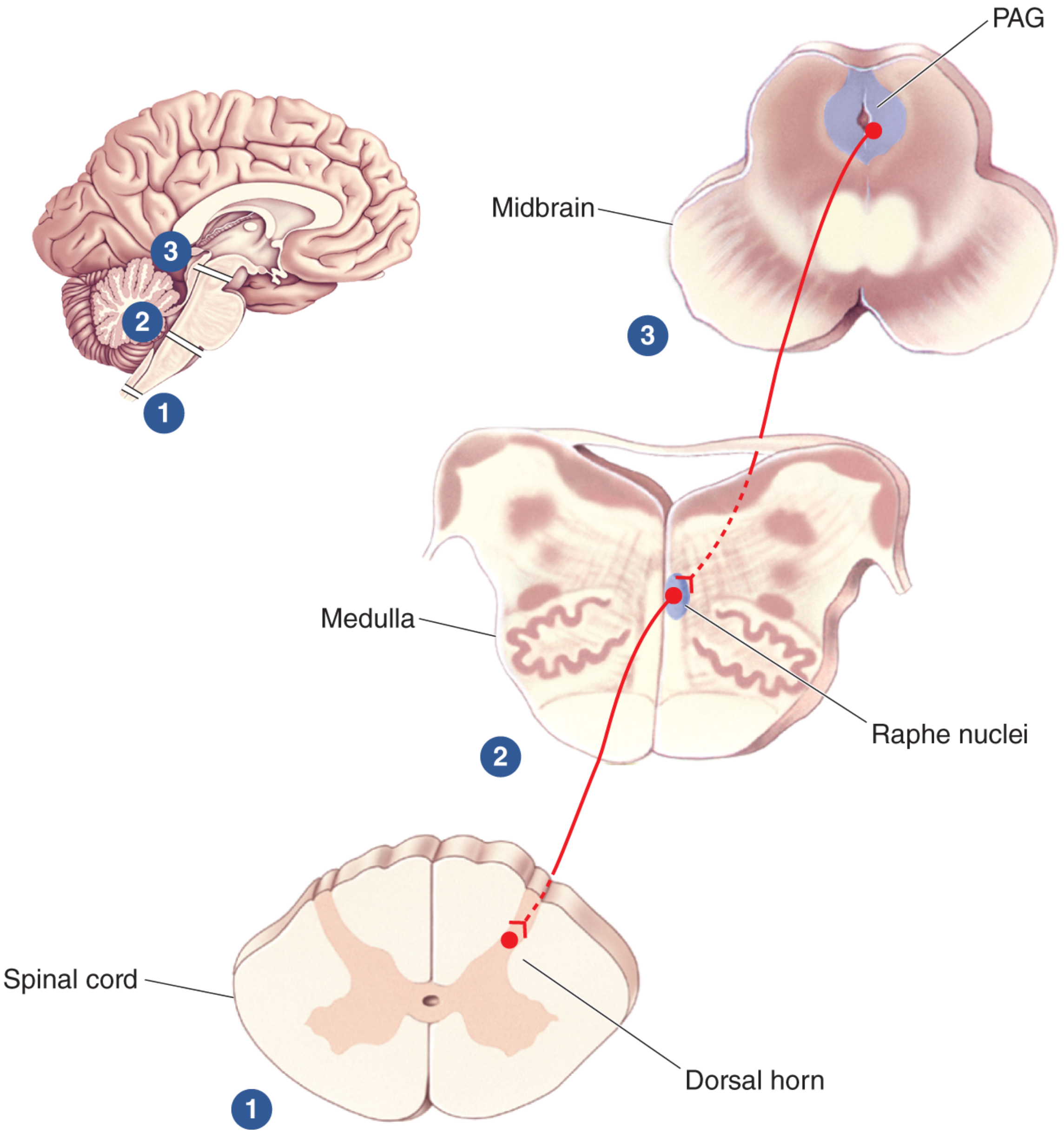
DIAGRAM 4 — TENS Unit Applied to the Back
DIAGRAM 5 — TENS Electrode Placement for Labor Pain (Spinal Levels)
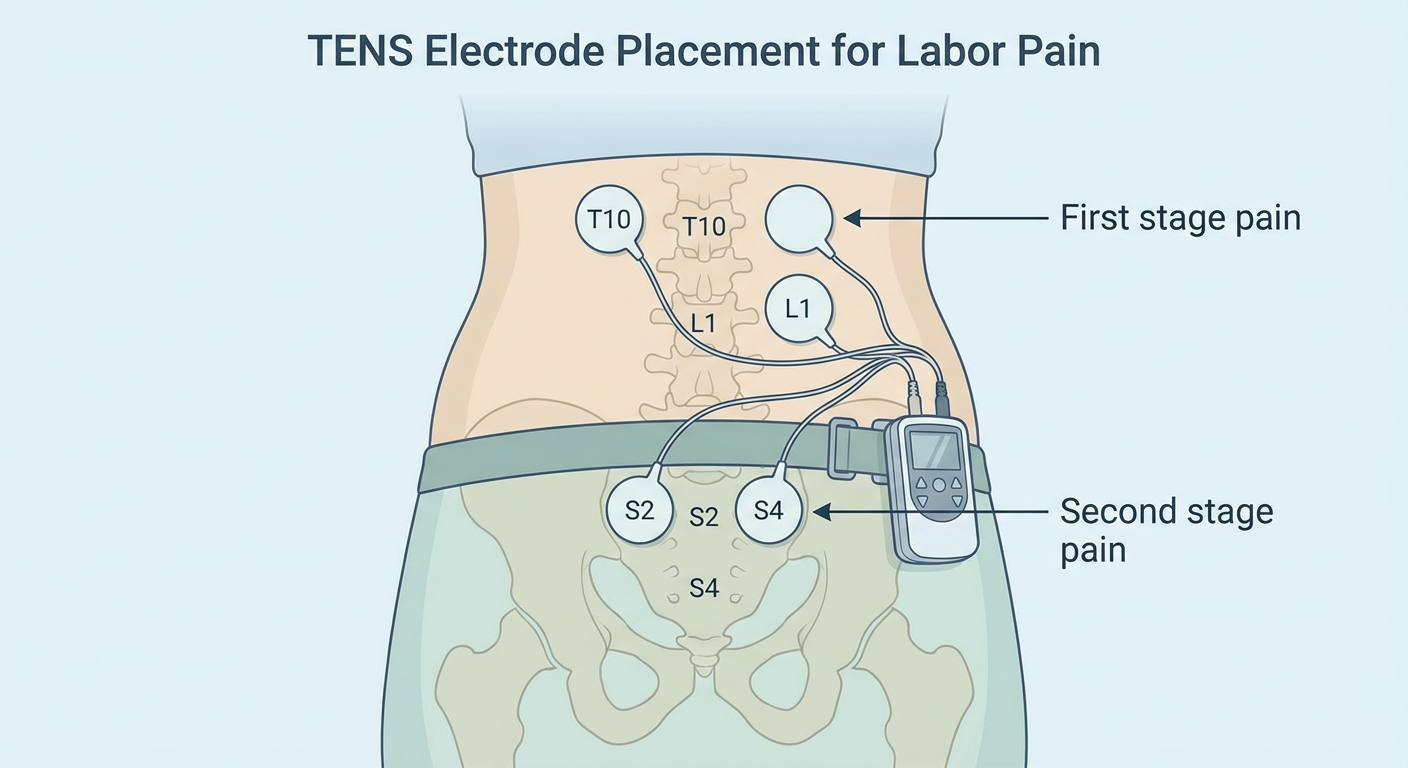
DIAGRAM 6 — Maternal Labor Positions
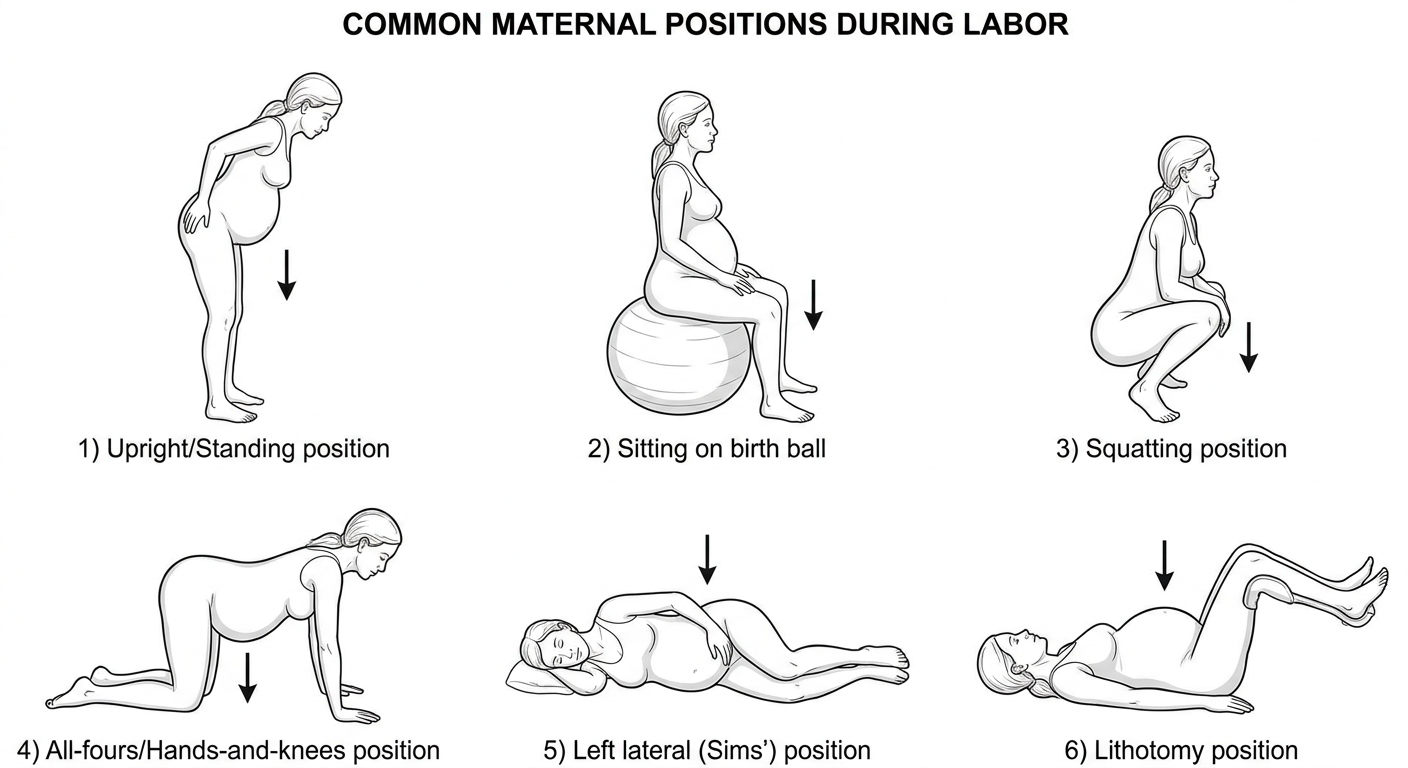
- Upright/Ambulating - gravity aids descent, shortens first stage
- Squatting - widens pelvic outlet, shortens second stage by ~9 min
- All-fours - best for OP rotation and back labor
- Left lateral (Sims') - prevents aortocaval compression, controlled delivery
- Lithotomy - clinical access, but no gravity advantage
- Sitting (birth ball) - significantly shorter second stage vs supine (RCT evidence)