Why is there right heart engorgement in asphyxial death
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a thorough, well-sourced answer. Here it is:
Right Heart Engorgement in Asphyxial Death
Right heart engorgement is one of the classic postmortem findings in asphyxial death. The mechanism involves a cascading series of events driven by hypoxia, CO2 retention, and obstructed pulmonary flow.
Step-by-Step Mechanism
1. Airway obstruction → Deficient oxygenation in lungs
When respiration is obstructed (hanging, strangulation, smothering, drowning, etc.), the lungs fail to oxygenate blood. Oxygen tension in the blood falls progressively.
2. Reduced oxygen tension → Capillary dilatation
Hypoxia and hypercapnia (rising CO2) act as potent vasodilators at the capillary and precapillary level. This is a direct local response of the microcirculation to oxygen lack.
3. Capillary dilatation → Capillary stasis → Capillary engorgement
The dilated capillaries and venules lose their tone. Blood pools within them - a state called capillo-venous engorgement. Blood stagnates rather than returning to the heart.
4. Capillary stasis → Stasis of blood in organs → Diminished venous return to the heart
As blood pools peripherally and in organs, venous return to the right heart is progressively reduced. This creates a paradox: there is a massive volume of blood in the periphery and organs, but the right heart is being "starved" of preload initially.
5. Reduced pulmonary flow → Back-pressure in the pulmonary circuit
The right ventricle tries to pump blood into the lungs, but the lungs are now consolidated and hypoxic, with increased pulmonary vascular resistance (hypoxic pulmonary vasoconstriction). The right heart pumps against a high-resistance, poorly oxygenating lung bed.
6. Right heart continues to beat after respiration stops
This is a key point: the heart continues to beat for several minutes (up to 10-15 minutes in hanging) after respiration ceases. During this time, the right ventricle keeps receiving venous blood from the systemic circulation (which is pooling and being driven back centrally by convulsive muscle activity and peripheral vasoconstriction), but cannot effectively move it through the obstructed/failing pulmonary circuit. Blood accumulates in the right atrium and right ventricle.
7. Final result: Right heart distension with dark, fluid blood
At autopsy, the right heart is found engorged with dark, fluid blood (dark because it is deoxygenated, fluid because hypercapnia prevents clotting - CO2 inhibits the clotting cascade). The left heart, by contrast, tends to be relatively empty, as oxygenated blood could not cross the pulmonary circuit in the final phase.
The Vicious Cycle (textbook diagram)
This diagram from The Essentials of Forensic Medicine and Toxicology illustrates the self-perpetuating mechanism:
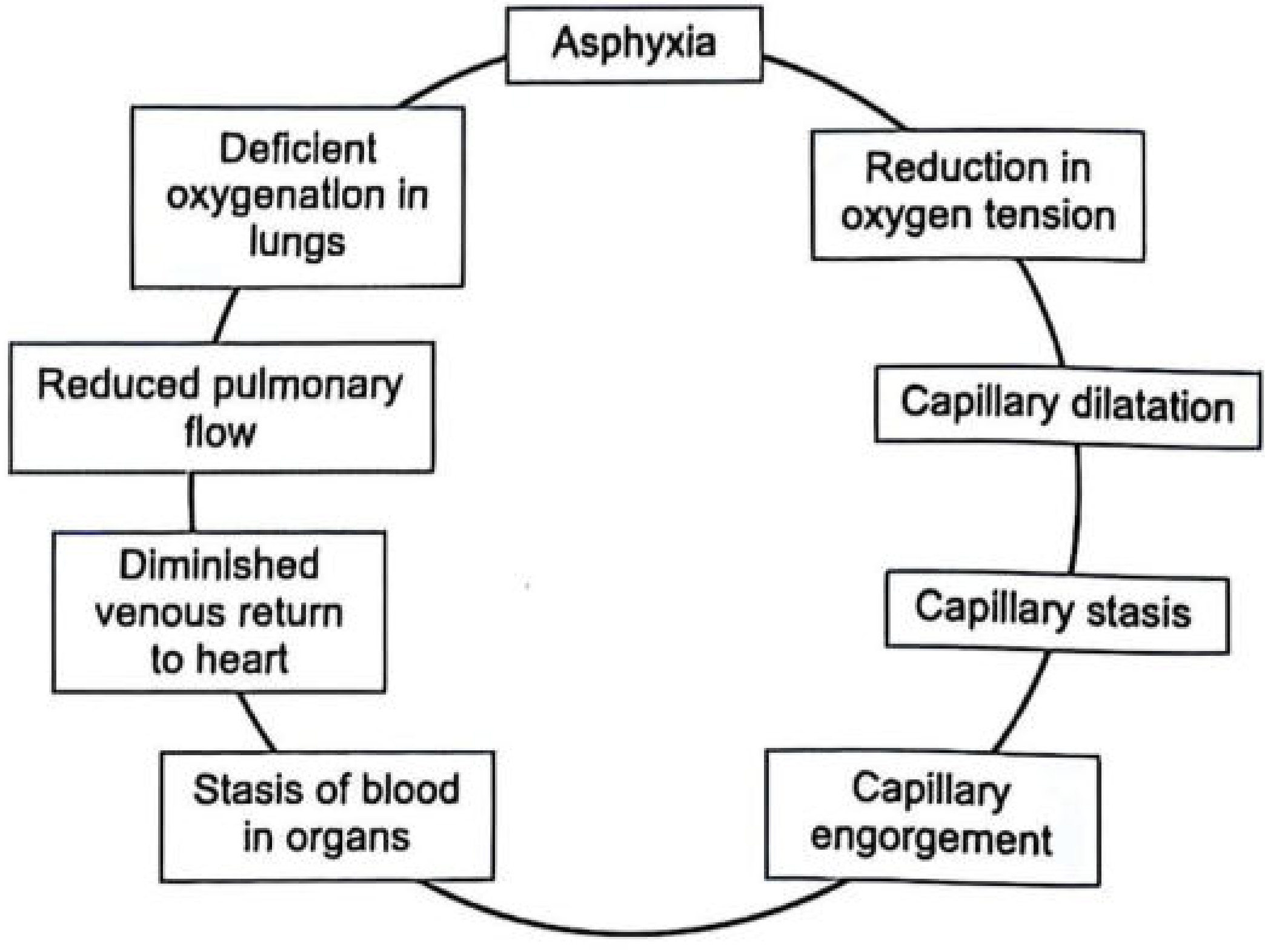
Fig. 6.1 - Vicious cycle of asphyxia
Summary of Contributing Factors
| Factor | Role in right heart engorgement |
|---|---|
| Hypoxia | Causes capillary dilatation and stasis |
| Hypercapnia (CO2 rise) | Peripheral vasodilation, blood pooling; keeps blood fluid |
| Obstruction of pulmonary flow | Back-pressure on right heart; right ventricle cannot empty |
| Continued cardiac activity after apnea | Heart beats 10-15 min after breathing stops, filling right chambers |
| Convulsive muscle activity | Drives venous blood centrally, adding to right-sided preload |
| Hypoxic pulmonary vasoconstriction | Increases pulmonary vascular resistance, opposing right ventricular outflow |
At Autopsy
The classic postmortem cardiac findings in asphyxial death include:
- Right heart - dilated, engorged with dark, fluid blood
- Left heart - relatively empty (blood could not cross the pulmonary circuit)
- Petechial hemorrhages over the auriculoventricular junction of the heart (due to raised venous pressure from impaired venous return)
- Dark, congested lungs with pulmonary oedema (from hypoxia + raised pulmonary vessel pressure)
- Large veins full of blood throughout
Sources: The Essentials of Forensic Medicine and Toxicology, 36th ed. (2026), pp. 143, and the asphyxia chapter (FM3.1); Parikh's Textbook of Medical Jurisprudence, Forensic Medicine and Toxicology
I didn't understand the sixth point
No tools needed here - this is a clarification of something already in context.
Point 6 Explained: The Heart Keeps Beating After Breathing Stops
Think of it this way:
Breathing stops first. The heart does NOT stop at the same time.
In asphyxial death, there is a gap - the heart keeps beating for 10 to 15 minutes after the last breath. This is the key rule in forensic medicine:
"Breathing stops within 20 seconds of cardiac arrest, but the heart stops within 20 minutes of stopping of breathing."
So what happens during those 10-15 minutes?
Imagine the heart as a pump still running after the pipe gets blocked
- The right side of the heart receives blood from the body via the veins (superior and inferior vena cava) and pumps it into the lungs
- But the lungs are now not working - they cannot oxygenate blood, and the pulmonary vessels have constricted (hypoxic pulmonary vasoconstriction)
- So the right ventricle keeps pumping blood toward the lungs, but the blood cannot move forward through the blocked/congested pulmonary circuit
- Blood backs up into the right ventricle and right atrium
Meanwhile, the body's convulsive muscle activity (the violent struggling seen in asphyxia) is squeezing veins and forcing even more blood back toward the right heart from the periphery.
The result: the right heart keeps receiving blood from behind (veins) but cannot send it forward (into lungs). So it fills up and becomes engorged.
The left heart, on the other hand, receives no oxygenated blood from the lungs, so it empties out and stays relatively empty at autopsy.
Simple analogy
It is like water filling up behind a dam. The river (venous blood) keeps flowing in, the dam (failed pulmonary circuit) blocks forward flow, so the reservoir (right heart) overflows and becomes engorged.
This is a shared conversation. Sign in to Orris to start your own chat.