Tension mesh hernioplasty surgery steps
Reading File
Finding Sources
Searching the Web
Lichtenstein tension-free mesh hernioplasty surgical steps technique
Finding Sources
Reading Web Page
https://emedicine.medscape.com/article/1534281-technique
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a complete, step-by-step guide to the Lichtenstein Tension-Free Mesh Hernioplasty (the gold standard open inguinal hernia repair with a recurrence rate of only 1-1.6%):
Lichtenstein Tension-Free Mesh Hernioplasty - Surgical Steps
Overview
First described by Lichtenstein in the 1980s and refined by Amid in 1993, this operation reinforces the inguinal floor with a polypropylene mesh placed between the transversalis fascia and the external oblique aponeurosis, eliminating the tissue tension inherent in older repairs (Bassini, Shouldice). The mesh extends well beyond Hesselbach's triangle so that raised intra-abdominal pressure causes the external oblique aponeurosis to apply counter-pressure onto the mesh, distributing force across a large interface.
- Fischer's Mastery of Surgery, 8th ed., p. 6019
- Mulholland and Greenfield's Surgery, 7th ed., p. 3693
STEP 1 - Patient Positioning & Anaesthesia
- Patient supine, both arms abducted; surgeon stands ipsilateral to the hernia.
- Preferred anaesthesia: Local anaesthesia + monitored anaesthesia care (MAC/sedation). This avoids nausea, vomiting, and urinary retention associated with general anaesthesia and is appropriate for all reducible adult inguinal hernias.
- Local anaesthetic mixture: 50:50 of 1% lidocaine + 0.5% bupivacaine with 1:200,000 epinephrine.
- Injection sequence:
- 5 mL subdermal along incision line
- 5 mL intradermal along incision line
- 10 mL deep subcutaneous (vertical insertions 2 cm apart)
- 10 mL subaponeurotic - bathes the ilioinguinal, iliohypogastric, and genitofemoral nerves; hydro-dissects the cord away from external oblique
- Additional 10 mL injected before closure for prolonged analgesia
- Skin prepped from above the umbilicus to past the inguinal ligament (extend to scrotum if scrotal hernia).
- Prophylactic antibiotics per local practice (coverage of skin flora).
STEP 2 - Skin Incision
- Oblique transverse incision, approximately 6 cm, starting 1-2 cm above the pubic tubercle, extending along Langer's lines.
- Divide subcutaneous tissue; ligate the superficial epigastric vein.
STEP 3 - Opening the External Oblique Aponeurosis
- Expose the external oblique aponeurosis.
- Incise it and separate the lower leaf from the spermatic cord; free the upper leaf from the underlying internal oblique until the internal oblique aponeurosis and conjoined tendon are fully exposed (~3 cm above the upper margin of the inguinal floor).
- Identify and protect three nerves throughout this step:
- Ilioinguinal nerve
- Iliohypogastric nerve
- Genital branch of the genitofemoral nerve (the blue-colored external spermatic vein delineates the adjacent white line of the genital nerve)
STEP 4 - Spermatic Cord Mobilisation
- Using an atraumatic Kittner dissector, separate the cord (with cremasteric muscle fibers) from the floor of the inguinal canal and pubic bone, extending 2 cm caudal to the pubic tubercle to create space for medial mesh overlap.
- Encircle all cord structures (ilioinguinal nerve, genitofemoral nerve, spermatic vessels) in a tape for handling.
- Avoid complete stripping of cremasteric fibers (increases morbidity, exposes the genital nerve, paravasal nerves, and vas deferens to mesh - raising risk of chronic pain and orchialgia).
- Incise the cremasteric sheath longitudinally at the level of the deep ring to detect an indirect hernia sac.
STEP 5 - Hernia Sac Management
Indirect hernia sac
- Dissect the sac free from cord structures toward the internal inguinal ring.
- Reduce it back into the preperitoneal space without ligation (ligation is unnecessary and increases early post-op pain without reducing recurrence).
- For a large sac: open it, inspect contents, resect redundant peritoneum, and ligate the proximal sac. Fenestrate the distal anterior wall to prevent hydrocele.
Direct hernia sac
- Invert the sac without tension to increase mesh-to-floor contact area and prevent pseudo-recurrence below the mesh.
- A broad direct defect: imbricate with an absorbable running suture to recreate the inguinal floor.
- A narrow direct hernia: purse-string suture circumferentially along the transversalis fascia.
- Important: these sutures must avoid the inguinal ligament (reserved for mesh fixation).
Femoral canal check
- Routinely evaluate the femoral canal via the space of Bogros:
- Direct hernia: small opening in the canal floor
- Indirect hernia: through the indirect sac
- If femoral hernia found: open the transversalis fascia, repair simultaneously using a posteroinferior triangular mesh leaflet fixed along the Cooper ligament.
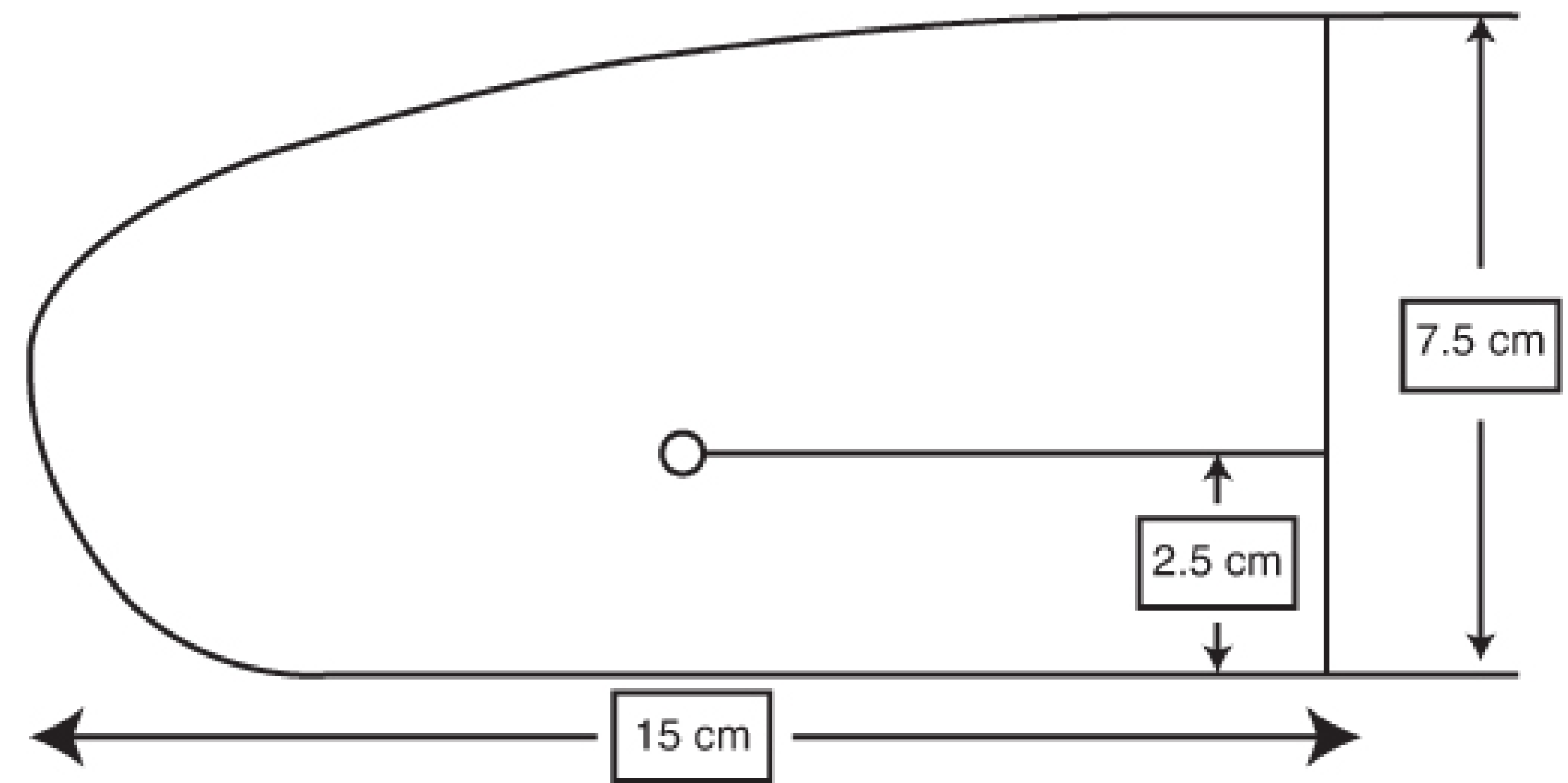
STEP 6 - Mesh Selection & Shaping
- Use a flat lightweight or midweight, monofilament, macroporous polypropylene mesh, 7.5 × 15 cm.
- Lightweight mesh = lower post-op pain, less foreign body sensation, equivalent recurrence rates.
- Macroporous mesh = more resistant to infection.
- Shape the mesh to an inverted-heel shape:
- Inferior side aligned with the inguinal ligament
- Rounded medial end matched to the angle of the inguinal ligament with the rectus sheath at the pubic tubercle
- Superior curve covering the floor to the conjoined tendon
STEP 7 - Mesh Fixation (Lower Edge)
- Place the medial end of the mesh at least 2 cm medial to the pubic tubercle - this overlap is critical; failure here is the most common cause of inferomedial recurrence as the mesh contracts over time.
- Avoid suturing into the periosteum of the pubic bone (prevents osteitis pubis).
- Using a permanent (non-absorbable) running suture (2-0 monofilament), fix the inferior edge of the mesh to the shelving edge of the inguinal ligament, running continuously from the pubic tubercle laterally to just proximal to the internal ring.
- Control suture depth carefully - too deep risks the femoral artery and vein passing deep to the inguinal ligament.
STEP 8 - Creating the Tails (Lateral Slit)
- At the lateral end of the mesh, make a slit creating two tails:
- Upper (wider) tail: approximately 2/3 of the mesh width
- Lower (narrower) tail: approximately 1/3 of the mesh width
- The slit extends to a point just medial to the internal inguinal ring.
- Grasp the wider upper tail with forceps and pass it cephalad (toward the head) from underneath the spermatic cord - this positions the cord between the two tails of the mesh.
- Cross the upper tail over the narrower lower tail and hold with a hemostat.
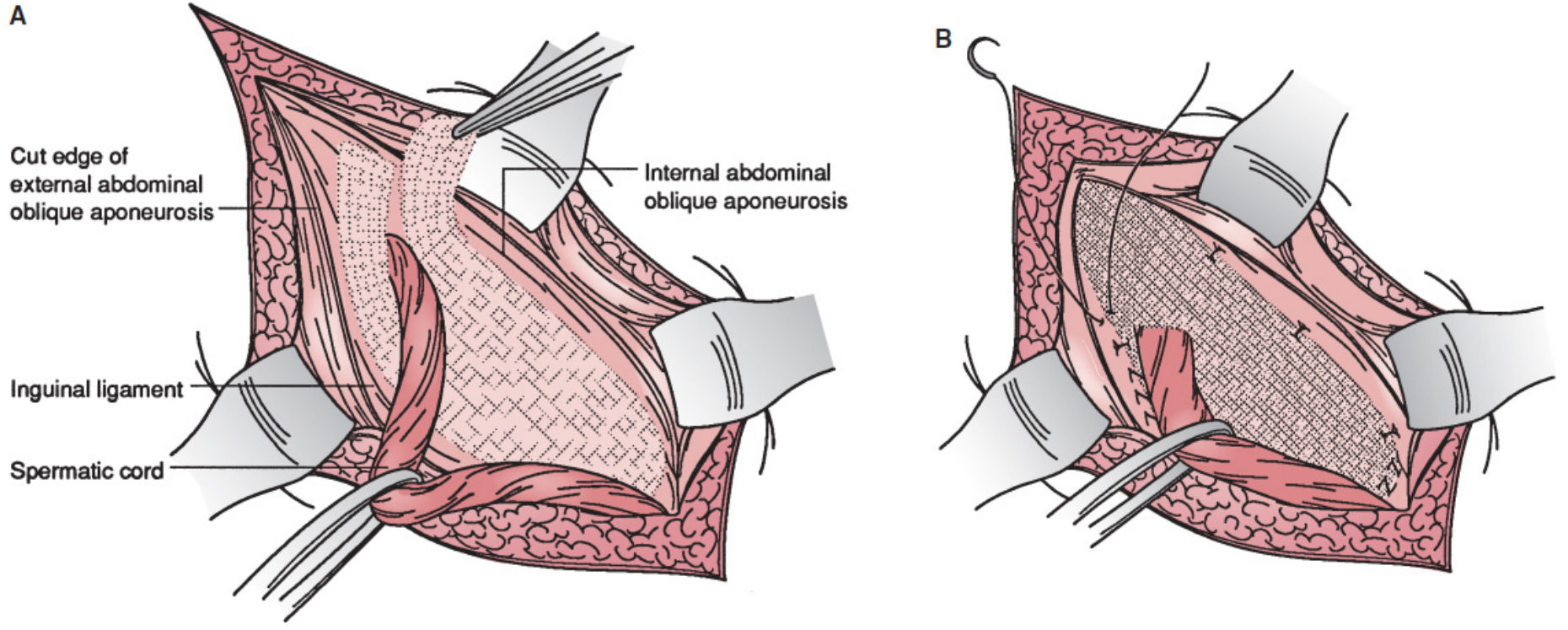
STEP 9 - Mesh Fixation (Upper Edge & Tails)
- Retract the cord downward and the upper leaf of the external oblique aponeurosis upward.
- Fix the upper edge of the mesh with typically 3 interrupted 2-0 absorbable sutures:
- One suture to the rectus sheath
- Two sutures to the internal oblique aponeurosis medial to the internal ring
- Suture parallel to the iliohypogastric nerve direction; tie knots loosely to avoid entrapment.
- Using a single non-absorbable monofilament suture, fix the lower lateral edges and overlapping tails to the inguinal ligament just lateral to the last knot of the lower running suture - this reconstructs the internal ring out of mesh.
- The new internal ring should accept the tip of a forceps but not the surgeon's index finger.
- Trim excess mesh leaving at least 4 cm lateral to the internal ring (to cover any coexisting interstitial or Spigelian hernia).
- Tuck the excess mesh tail underneath the external oblique aponeurosis.
STEP 10 - Wound Closure
- Close the external oblique aponeurosis over the cord with an absorbable running suture - also reconstructs the external inguinal ring.
- Reapproximate Scarpa's fascia with an absorbable suture.
- Close the skin with an absorbable subcuticular suture in a running fashion.
Key Anatomic Landmarks to Protect
| Structure | Importance |
|---|---|
| Ilioinguinal nerve | Provides scrotal/labial sensation; entrapment causes chronic groin pain |
| Iliohypogastric nerve | At risk during upper mesh fixation sutures |
| Genital branch, genitofemoral nerve | Runs alongside external spermatic vein; cremasteric spasm/orchialgia if injured |
| Femoral artery & vein | Deep to inguinal ligament; at risk from deep bites when suturing inferior mesh edge |
| Vas deferens & spermatic vessels | Risk of ischemic orchitis/testicular atrophy |
Outcomes
| Metric | Value |
|---|---|
| Recurrence rate | 1-1.6% |
| Chronic post-herniorrhaphy inguinal pain (CPIP) | 10-15% |
| Anaesthesia | Local + MAC (outpatient) |
| Return to activity | 2-3 weeks |
| Mesh integration | Native tissue ingrowth within 2-3 weeks |
Sources:
- Fischer's Mastery of Surgery, 8th edition, Chapter 220 (Lichtenstein-Amid Tension-Free Hernioplasty), pp. 6019-6030
- Mulholland and Greenfield's Surgery, 7th edition, Chapter 72, pp. 3692-3693
- Medscape - Open Inguinal Hernia Repair Technique
Inguinal canal noundaries
Finding Sources
Searching the Web
inguinal canal boundaries anatomy walls roof floor
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Excellent - I now have comprehensive textbook information and anatomical diagrams. Here is the complete answer:
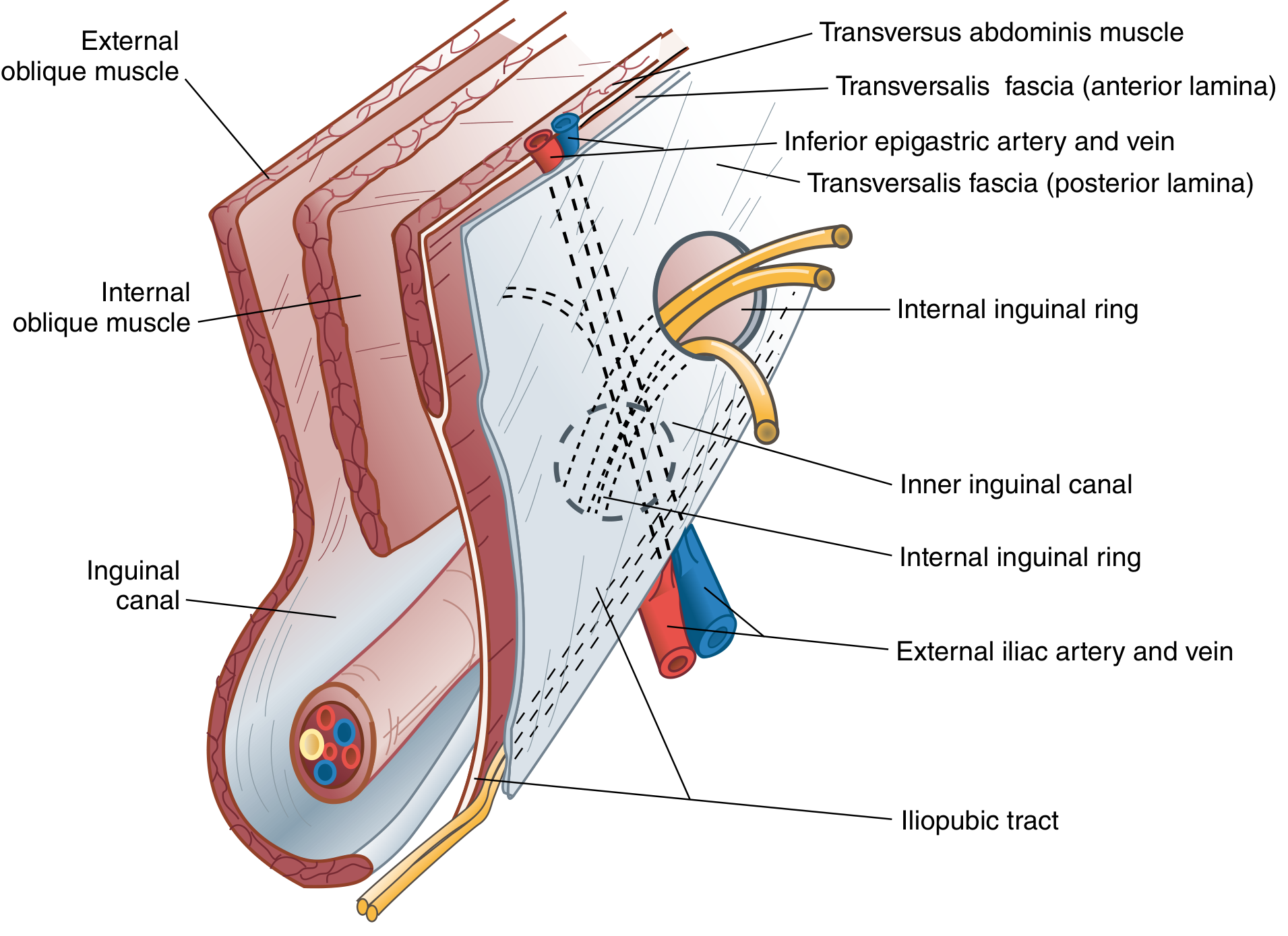
Inguinal Canal - Boundaries
The inguinal canal is an oblique passage, approximately 4-6 cm long, running downward, forward, and medially through the inferior part of the anterior abdominal wall, just above and parallel to the inguinal ligament. It transmits the spermatic cord in males and the round ligament of the uterus in females, plus the ilioinguinal nerve in both sexes.
Openings (Rings)
| Opening | Description | Relations |
|---|---|---|
| Deep (Internal) Inguinal Ring | Defect in the transversalis fascia; outpouching forms the internal spermatic fascia | Midway between ASIS and pubic tubercle; inferior epigastric vessels lie just medial to it |
| Superficial (External) Inguinal Ring | Inverted V-shaped defect in the external oblique aponeurosis | Bounded by medial crus (superomedially), lateral crus (inferolaterally), intercrural fibers, and reflected inguinal ligament; lies lateral to the pubic tubercle |
Boundaries (Walls)
Anterior Wall
- External oblique aponeurosis - present throughout the entire length of the canal
- Reinforced laterally by the lowermost fibers of the internal oblique muscle
Posterior Wall
- Transversalis fascia - throughout the entire length
- Reinforced medially by the conjoint tendon (inguinal falx) - the merged aponeurosis of internal oblique and transversus abdominis, which descends to the pubic tubercle
- (Also partially thickened by the interfoveolar ligament)
Roof (Superior Wall)
- Arching fibers of internal oblique and transversus abdominis muscles, which curve over the canal from lateral to medial before descending to form the conjoint tendon
Functional note: When the internal oblique and transversus abdominis contract, the roof closes down against the floor (shutter mechanism), actively narrowing the canal and preventing herniation during rises in intra-abdominal pressure.
Floor (Inferior Wall)
- Laterally - iliopubic tract
- Centrally - superior (gutter-like) surface of the inguinal ligament (Poupart's ligament) - the thickened, rolled-inward inferior edge of the external oblique aponeurosis
- Medially - lacunar ligament (Gimbernat's ligament)
Summary Table
| Wall | Structure | Reinforcement |
|---|---|---|
| Anterior | External oblique aponeurosis | Internal oblique muscle (laterally) |
| Posterior | Transversalis fascia | Conjoint tendon (medially) |
| Roof | Internal oblique + transversus abdominis (arching fibers) | - |
| Floor | Inguinal ligament (centrally) | Iliopubic tract (laterally), lacunar ligament (medially) |
Anatomical Diagrams

Clinical Relevance to Hernias
The relationship of a hernia to the inferior epigastric vessels (which run just medial to the deep ring) distinguishes the two common types:
| Hernia Type | Path | Relation to Inferior Epigastric Vessels |
|---|---|---|
| Indirect inguinal hernia | Enters via deep ring → travels through full length of canal → exits via superficial ring | Lateral to inferior epigastric vessels |
| Direct inguinal hernia | Pushes directly through the posterior wall (Hesselbach's triangle) | Medial to inferior epigastric vessels |
Hesselbach's triangle (site of direct hernias) is bounded by:
- Superolateral: inferior epigastric vessels
- Medial: lateral border of rectus sheath
- Inferior: inguinal ligament and pectineal (Cooper's) ligament
Sources:
- Campbell-Walsh-Wein Urology, 3-Volume Set, Chapter 109, p. 3231
- Bailey and Love's Short Practice of Surgery, 28th ed., Chapter 64, p. 1087
- Sabiston Textbook of Surgery, Chapter 82, p. 1681
- THIEME Atlas of Anatomy - General Anatomy and Musculoskeletal System, Section 5.7
Conjoint tendon where is it prent
Finding Sources
Searching the Web
conjoint tendon inguinal falx anatomy location formation insertion
Reading File
Reading File
Loading Image
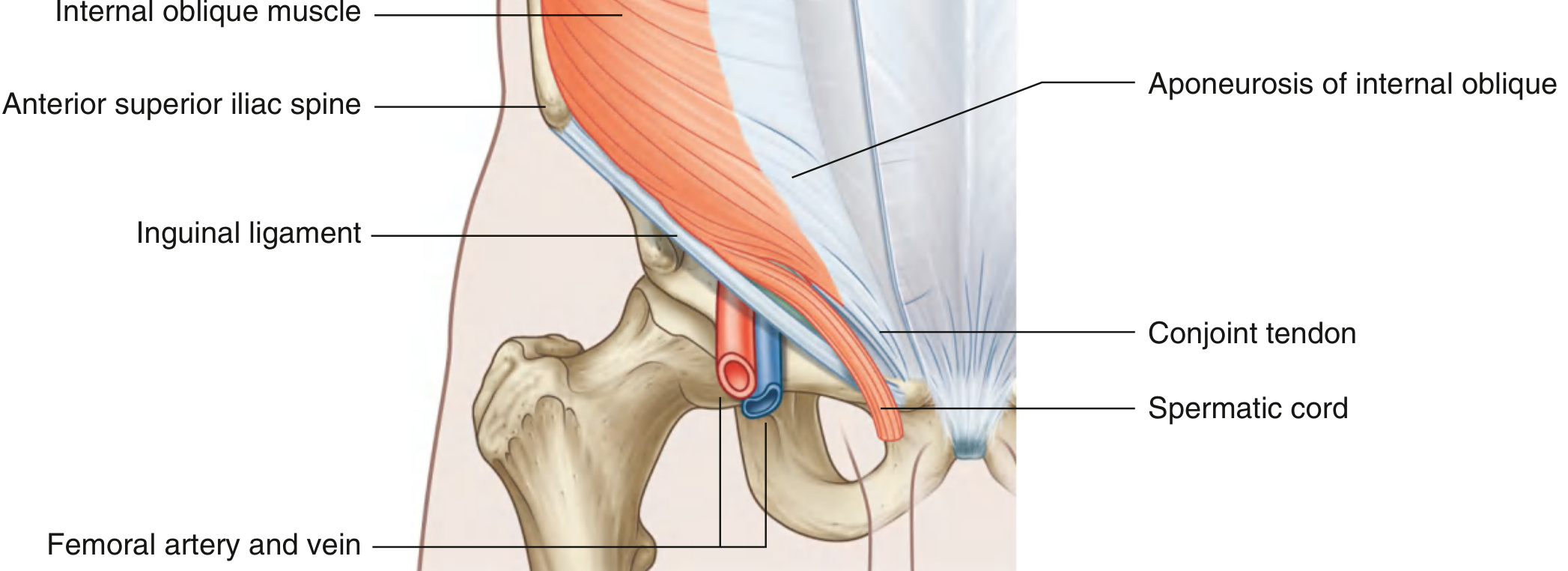
Conjoint Tendon (Inguinal Falx) - Where It Is Present
What It Is
The conjoint tendon (also called the inguinal falx or inguinal aponeurotic falx) is the fused lower aponeurosis of two muscles of the anterior abdominal wall:
- Internal oblique muscle (medial fibers)
- Transversus abdominis muscle (medial fibers)
Important note: True fusion only occurs in about 5% of individuals. In most people, the aponeuroses of the two muscles remain partially separate but lie closely apposed and function together as a unit. The term "conjoint tendon" is still used clinically to describe this region.
Exact Location
The conjoint tendon is located in the lower medial part of the anterior abdominal wall, in the inguinal region. Specifically:
- It lies directly posterior to (behind) the superficial inguinal ring
- It forms the medial one-third of the posterior wall of the inguinal canal
- It is situated between the deep inguinal ring (laterally) and the pubic tubercle (medially)
How It Is Formed
The arching fibers of the internal oblique and transversus abdominis muscles:
- Originate laterally from the inguinal ligament
- Arch superiorly over the deep inguinal ring (forming the roof of the inguinal canal)
- Curve medially and downward
- Fuse into a common tendinous insertion at the medial end = the conjoint tendon
Insertion (Attachment)
The conjoint tendon inserts into two bony points:
| Attachment | Location |
|---|---|
| Pubic crest | Upper border of pubic body, medially |
| Pectineal line (pecten pubis) | Superior ramus of pubis, extending laterally |
These insertions are immediately deep to the superficial inguinal ring.
Role in the Inguinal Canal
| Wall | Contribution |
|---|---|
| Posterior wall | Reinforces the medial 1/3 - the area behind the superficial ring (most vulnerable zone for direct hernias) |
| Roof | The arching fibers of the same muscles, before they descend as the conjoint tendon, form the roof of the canal |
The conjoint tendon acts as a dynamic shutter: when intra-abdominal pressure rises (coughing, straining), the muscles contract, pulling the conjoint tendon downward toward the inguinal ligament, closing the posterior wall and protecting against herniation.
Clinical Significance
| Condition | Relevance |
|---|---|
| Direct inguinal hernia | A weak or deficient conjoint tendon allows bowel/omentum to bulge directly through the posterior wall of the inguinal canal (Hesselbach's triangle), medial to the inferior epigastric vessels |
| Hernia repair (Bassini, Shouldice, McVay) | These tissue repairs all involve suturing the conjoint tendon (or its components) to the inguinal ligament or Cooper's ligament to reinforce the posterior wall |
| Lichtenstein repair | The upper edge of the mesh is sutured to the conjoint tendon (internal oblique aponeurosis) with interrupted absorbable sutures |
Summary
| Feature | Detail |
|---|---|
| Formed by | Merged aponeuroses of internal oblique + transversus abdominis |
| Location | Medial inguinal region, behind superficial inguinal ring |
| Inserts into | Pubic crest + pectineal line (pecten pubis) |
| Role in inguinal canal | Reinforces medial 1/3 of posterior wall |
| Clinical relevance | Weakness here → direct inguinal hernia; sutured to inguinal/Cooper's ligament in tissue repairs |
Sources:
- Gray's Anatomy for Students, Chapter 4 (Posterior wall of inguinal canal), p. 353
- Sabiston Textbook of Surgery, Chapter 82 (Internal Oblique Muscle and Aponeurosis), p. 1680
- StatPearls - Conjoint Tendon (Inguinal Aponeurotic Falx)
This is a shared conversation. Sign in to Orris to start your own chat.