Types of chronic elbow disslocation
Reading File
Finding Sources
Finding Sources
Searching the Web
types chronic elbow dislocation classification orthopedics
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Searching PubMed
chronic elbow dislocation classification treatment
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive overview of chronic elbow dislocation and its types.
Chronic (Neglected) Elbow Dislocation
A chronic elbow dislocation is defined as one that has not been reduced and has been present for >6 weeks (some sources use 3–4 weeks). An unreduced dislocation of 2–6 weeks duration is typically called subacute. These terms reflect the progressive fibrosis, contracture, heterotopic ossification, and joint remodeling that make late treatment increasingly difficult.
Classification Framework
Chronic elbow dislocations are classified along two axes:
1. By Time (Temporal Classification)
| Category | Duration |
|---|---|
| Acute | <2 weeks from injury |
| Subacute | 2–6 weeks |
| Chronic (missed/neglected) | >6 weeks |
This distinction has major therapeutic implications. Dislocations at <2 weeks can usually be managed with primary ligament repair after open reduction. Beyond 6 weeks, extensive soft tissue contracture, ossification, and cartilage changes often require more complex reconstruction, interposition arthroplasty, or staged procedures.
2. By Direction (Anatomic/Directional Classification)
This is the primary classification used in practice. The ulna and radius displace as a unit relative to the distal humerus:
| Type | Features |
|---|---|
| Posterior / Posterolateral | Most common (~80%). Fall on outstretched hand, valgus + axial + posterolateral force. Olecranon prominent posteriorly, elbow held at ~45° flexion. |
| Anterior | Rare. Blow to the olecranon with elbow flexed. Forearm elongated and supinated, elbow fully extended, olecranon fossa palpable posteriorly. Frequently open, often with triceps avulsion or vascular injury. |
| Medial | Uncommon. Similar mechanism to posterior but with a medial force vector. |
| Lateral | Uncommon. Displacement of radius and ulna laterally. |
| Divergent | Very rare. Simultaneous dislocation between the radius and ulna (proximal radioulnar joint dissociation) alongside the ulnohumeral dislocation — the radius and ulna diverge from each other. Requires considerable energy. |
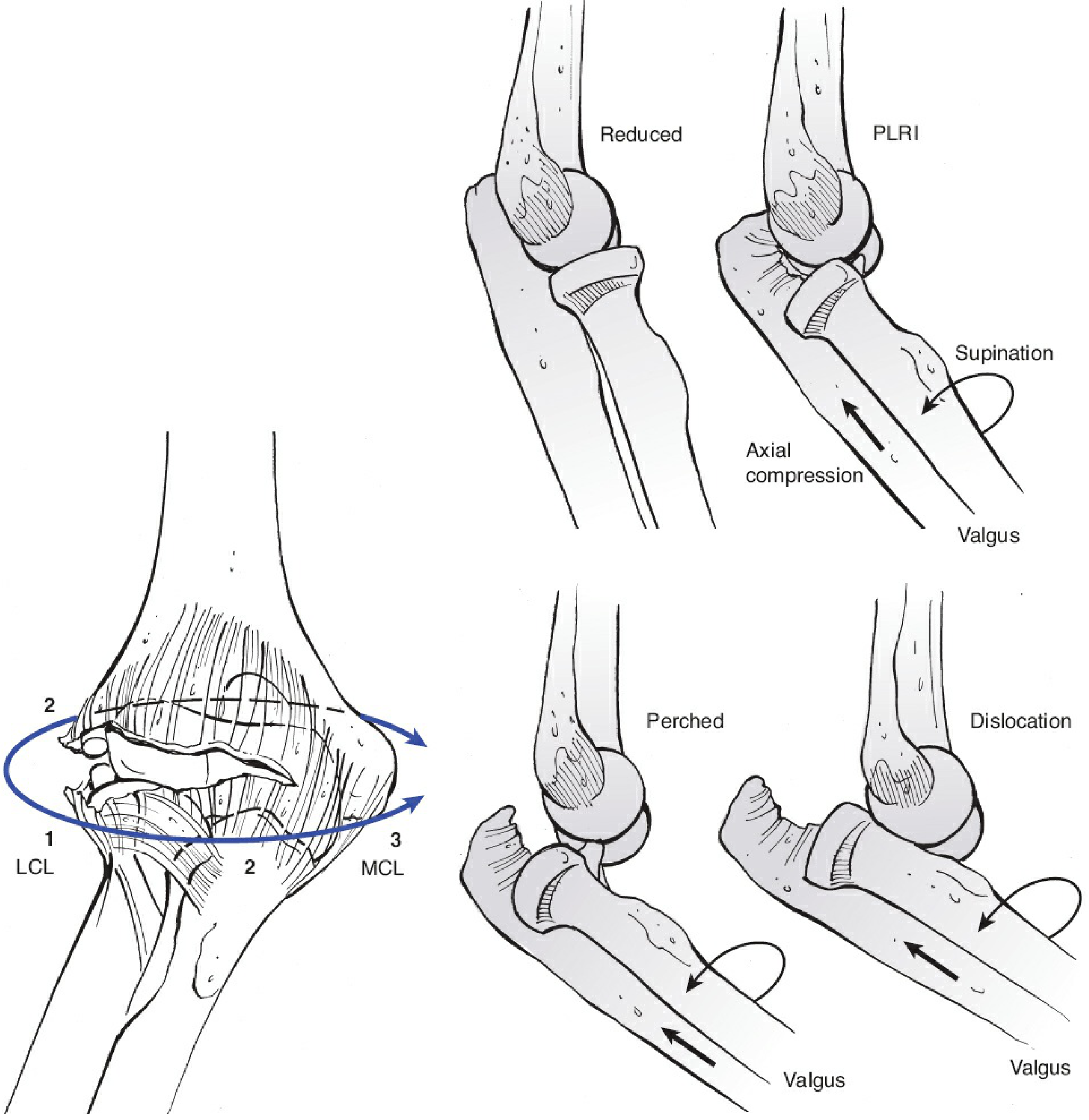
Progression of soft tissue disruption in elbow dislocation (O'Driscoll's "circle of Horii") — begins at the LCL laterally (Stage 1) and progresses medially (Stage 3).
3. By Complexity
| Type | Definition |
|---|---|
| Simple | No associated fractures |
| Complex | Associated fractures (radial head, coronoid, capitellum, etc.) |
The classic complex injury is the "Terrible Triad" — elbow dislocation + radial head fracture + coronoid fracture + LCL injury. Missed/chronic terrible triad injuries present an even greater reconstructive challenge.
4. By Stability Pattern (O'Driscoll Staging — Posterolateral Rotatory Instability)
| Stage | Pathology |
|---|---|
| Stage 1 | LCL partially/completely disrupted → posterolateral rotatory instability (PLRI) |
| Stage 2 | Additional anterior and posterior capsular disruption. Coronoid "perched" on trochlea (incomplete posterolateral dislocation) |
| Stage 3A | Complete dislocation; posterior MCL bundle disrupted, anterior MCL intact |
| Stage 3B | Entire MCL disrupted — varus, valgus, and rotary instability after reduction |
| Stage 3C | Soft tissues stripped from entire distal humerus including flexor-pronator and extensor origins — grossly unstable even in flexion |
In chronic cases, most untreated injuries are functionally Stage 3B or 3C due to progressive soft tissue failure.
5. Recurrent Dislocation
Recurrent dislocation of the elbow (repeated episodes of dislocation) is rare — unlike the shoulder. When it occurs, extensive disruption of both the MCL and LCL plus the muscle origins is usually demonstrated. Treatment requires ligamentous reconstruction, not just repair.
Radiographic Appearance

Lateral radiograph of posterior elbow dislocation — the classic appearance of a chronic neglected case.
Treatment Principles for Chronic Dislocation
The operative management of chronic elbow dislocation (>6 weeks) reported by Anderson et al. (2018) in 32 patients used a combined medial and lateral approach with triceps preservation, achieving good-to-excellent functional outcome in 79% of cases. Key principles:
- Combined medial and lateral approach to the elbow
- Ulnar nerve identification and protection
- Joint mobilization and reduction
- Ligament repair with transosseous sutures
- Early range of motion is critical — the greatest risk is post-reduction stiffness and flexion contracture (directly correlated with immobilization >3 weeks)
- Supplemental fixation (external fixator, internal joint stabilizer, or temporary cross-screw) if residual instability persists
Sources:
- Rockwood and Green's Fractures in Adults, 10th ed. 2025, Ch. 40 — Simple Elbow Dislocation
- Miller's Review of Orthopaedics, 9th ed. — Elbow Instability
- Rosen's Emergency Medicine, Concepts and Clinical Practice — Elbow Dislocations
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.