Peak expiratory flow rate full details for md exam answer 10 marks
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Here is a complete, exam-ready 10-mark answer on Peak Expiratory Flow Rate (PEFR):
Peak Expiratory Flow Rate (PEFR)
Definition
Peak Expiratory Flow Rate (PEFR) is the maximum airflow velocity (rate of airflow) achieved during a forced expiration delivered with maximal effort starting from total lung capacity (TLC). It is measured in litres per minute (L/min). Physiologically, it occurs during the most effort-dependent, early phase of the forced expiratory maneuver - typically within the first 100 milliseconds of expiration.
- Murray & Nadel's Textbook of Respiratory Medicine, p. 709
- Bailey and Love's Short Practice of Surgery 28th Ed., p. 998
Instrument Used
The most widely used device is the "mini-Wright" peak flow meter - a small, portable, inexpensive handheld device. A Wright peak flow meter (standard) or a peak flow gauge can also be used. Spirometers with flow-sensing technology (pneumotachographs, hot wire anemometers, rotating vane spirometers) can also measure PEFR. Different brands of meters may give slightly varying results, so serial measurements should ideally be done with the same brand.
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 62
Technique / Procedure
- Calibrate the meter; ensure the measurement bar is at the zero line.
- Patient should stand (or sit upright), chin elevated, neck slightly extended.
- After normal breathing, ask the patient to take a maximal inspiration to TLC.
- Seal lips tightly around the mouthpiece (tongue must not obstruct it).
- Perform a rapid, forceful expiration immediately (not slow and sustained).
- Record the value; repeat three times and take the best (highest) value.
- A nose clip is not required for PEFR but may help during formal spirometry.
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, pp. 62-63
Normal Values
Normal PEFR ranges from 350 to 600 L/min in adults. Values are determined primarily by:
- Sex (men > women)
- Age (peaks at 30-35 years in men; women peak earlier)
- Height (taller individuals have higher PEFR)
Estimation formulas (when tables are unavailable):
- Adults:
PEFR = 13 × (Height in inches - 40) + 110 - Female children/adolescents:
PEFR = Height(m) × 5.5 - Age × 0.03 - 1.11 - Male children/adolescents:
PEFR = Height(m) × 6.14 - Age × 0.043 + 0.15
PEFR declines with age: After age 50, the average decline is approximately 4 L/min per year in men and 2.5 L/min per year in women.
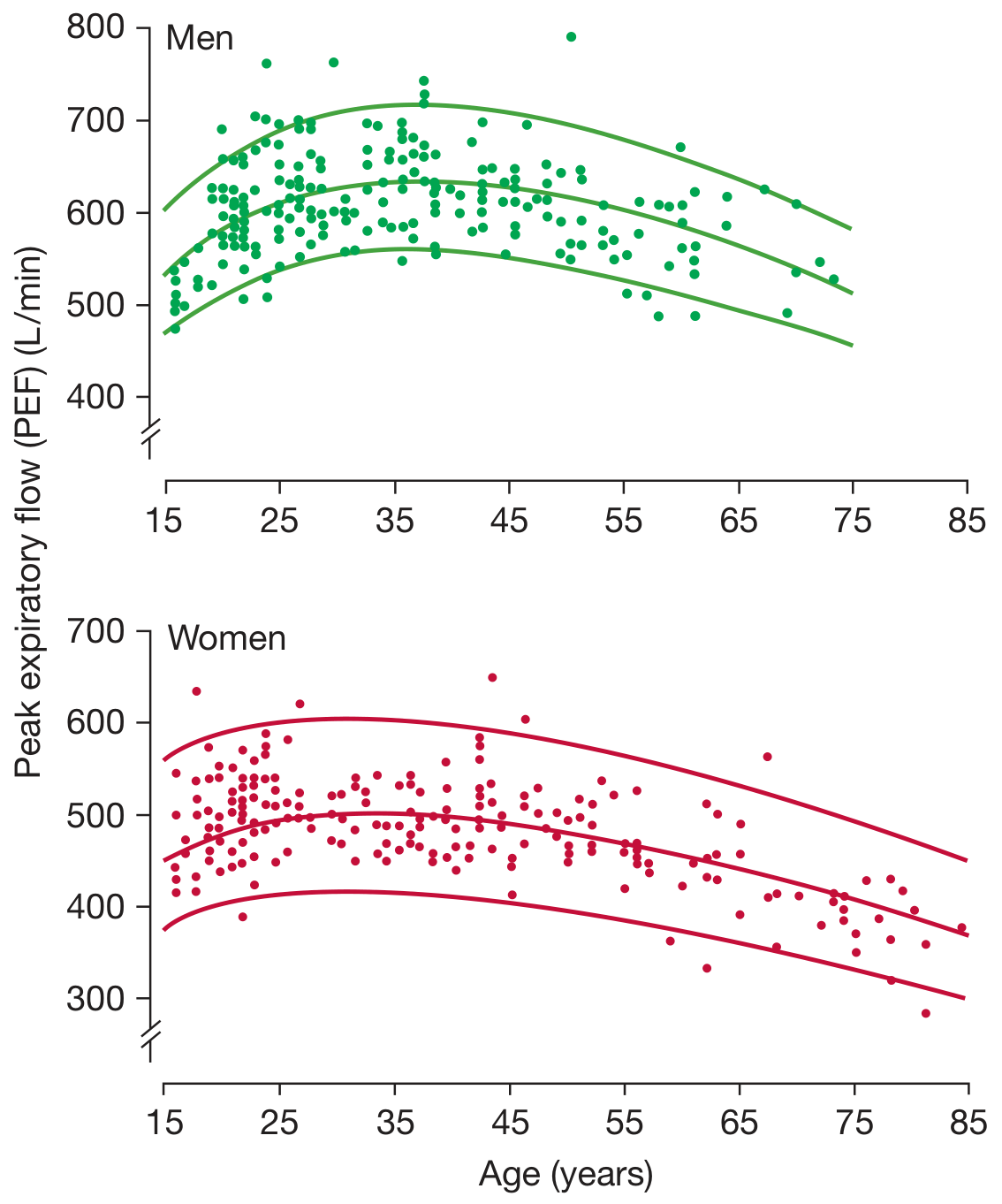
Figure: Peak expiratory flow in 225 males and 228 females who were healthy non-smokers. Center line = regression mean; outer lines = 90% confidence intervals. (Nunn AJ, Gregg I. Br Med J. 1989.) - Fishman's Pulmonary Diseases and Disorders, p. 287
Predicted PEFR for normal children (by height):
| Height (cm) | PEFR (L/min) | Height (cm) | PEFR (L/min) |
|---|---|---|---|
| 109 | 147 | 142 | 320 |
| 122 | 214 | 152 | 373 |
| 132 | 267 | 163 | 427 |
| 140 | 307 | 170 | 467 |
- The Harriet Lane Handbook 23rd Ed., Table 25.1
Physiology: What PEFR Reflects
PEFR manifests during the effort-dependent portion of forced expiration. When maximal effort is made, it is largely a function of the caliber of large (central) airways. It is also transiently influenced by expulsion of air from compressed central airways. For these reasons:
-
Decreased PEFR results from even slightly submaximal effort (not only from pathology)
-
PEFR is abnormally decreased only in moderate to severe airway obstruction
-
It does not reliably detect early small airway disease (unlike FEF25-75%)
-
Murray & Nadel's Textbook of Respiratory Medicine, p. 709
Clinical Uses
- Diagnosis of asthma: Serial PEFR readings varying by >20% either spontaneously or in response to treatment support a diagnosis of asthma.
- Diurnal variation monitoring: Twice-daily measurements (morning and evening) demonstrate the characteristic diurnal variation of asthma (typically lowest in the early morning - "morning dipping"). Variation >20% is significant.
- Assessing severity of acute asthma: Objective measure when symptoms and signs do not correlate well with the degree of obstruction.
- Monitoring treatment response: Serial PEFR is compared pre- and post-bronchodilator or pre- and post-systemic steroids.
- Occupational asthma: Regular monitoring identifies work-related patterns of airflow limitation.
- Patient self-monitoring: Patients keep personal records and compare to their "personal best" - the highest PEFR achieved when well-controlled.
- Pre-operative assessment and post-operative monitoring of respiratory function.
PEFR in Grading Acute Asthma Severity (NAEPP/NHLBI)
| Severity | Initial PEF (% of predicted or personal best) | Clinical Features |
|---|---|---|
| Mild | ≥70% | Dyspnea only with activity |
| Moderate | 40-69% | Dyspnea limiting usual activity |
| Severe | <40% | Dyspnea at rest, limits conversation |
| Life-threatening | <25% | Too dyspnoeic to speak; profuse sweating |
An alternative classification (Roberts and Hedges):
| % of Personal Best or Predicted | Severity |
|---|---|
| >80% | Mild |
| 51-80% | Moderate |
| 31-50% | Severe |
| ≤30% | Life-threatening |
- Tintinalli's Emergency Medicine, Table 69-3
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, Table 2.4
Decision thresholds in acute asthma management:
- Initial PEFR <20% predicted: may require further evaluation/intensive therapy
- Post-treatment PEFR <60% predicted: indicates further evaluation or admission needed
- Failure to recover PEFR to >70% personal best after bronchodilators: favors admission over discharge
Limitations of PEFR
- Effort dependent - submaximal effort gives falsely low values (unlike FEV1 which can detect poor effort by flow-volume curve analysis)
- Cannot distinguish obstructive vs. restrictive disease, vocal cord dysfunction, or poor effort (FEV1 is superior for this)
- Insensitive to early or small airway disease - it reflects large airway caliber
- Affected by pain - abdominal or thoracic wound pain prevents adequate effort
- Difficult in young children - not reliably performed by many children under 5-6 years; up to two-thirds of children >5 years cannot complete PEFR testing during an acute asthma attack
- Variation between devices - different brands/types of meters give slightly different readings, making cross-device comparison unreliable
- Normal PEFR does not exclude respiratory disease - patients with poor gas exchange may have normal PEFR
PEFR vs. FEV1 Comparison
| Feature | PEFR | FEV1 |
|---|---|---|
| Reflects | Large airway caliber | Overall airway obstruction |
| Effort dependency | High | Moderate |
| Equipment | Simple, portable, cheap | Spirometer required |
| Distinguishes obstructive vs restrictive | No | Yes |
| Serial monitoring | Excellent | Good |
| Use in acute asthma | Yes | Yes (preferred if available) |
Summary
PEFR is a simple, portable, and inexpensive measure of peak airflow that reflects large airway function. Its greatest clinical value lies in monitoring asthma - detecting diurnal variation, grading severity of exacerbations, and gauging response to treatment. The "personal best" PEFR is the gold standard reference for an individual patient. Despite its limitations (effort-dependence, insensitivity to small airway disease), it remains indispensable as a bedside and home monitoring tool in obstructive airway disease.
Sources: Murray & Nadel's Textbook of Respiratory Medicine | Bailey & Love's Short Practice of Surgery 28th Ed. | Roberts and Hedges' Clinical Procedures in Emergency Medicine | Tintinalli's Emergency Medicine | Fishman's Pulmonary Diseases and Disorders | The Harriet Lane Handbook 23rd Ed.
This is a shared conversation. Sign in to Orris to start your own chat.